



Introduction
Thailand’s Emergency Medical Services (EMS) are initiated with a call to the 1669 national emergency hotline from patients or other individuals; after that, the medical call center will dispatch either the nearest or most appropriate EMS units to provide emergency care. Reference Ienghong, Cheung, Tiamkao, Bhudhisawasdi and Apiratwarakul1,Reference Huabbangyang, Klaiangthong and Prasittichok2 In the case of an emergency patient being put in an ambulance, the assessment and treatment process starts with taking into account patient history, measuring vital signs, giving physical examinations, and providing necessary treatment. Reference van Vliet, Ebben, Diets, Pelgrim, Loef and Vloet3 Once the standard of emergency care has been implemented, the patient will be transported to the designated hospital via an emergency ambulance.
During the journey, the medical personnel on board the ambulance, such as doctors or nurses, are responsible for continuously assessing the patient’s condition. This involves observing the patient’s symptoms, conducting periodic questioning, and monitoring vital signs. Reference Pochaisan, Pattanarattanamolee, Pongphuttha, Chadbunchachai and Nakahara4 The collected information is then communicated via radio to the destination hospital or the hospital command center. This communication serves to provide crucial information about incoming patients to the emergency department (ED). As a result, the ED can prepare the necessary personnel and medical equipment to promptly initiate treatment upon the patient’s arrival at the hospital. Reference Apiratwarakul, Suzuki and Celebi5,Reference Pattanarattanamolee, Sanglun and Nakahara6
However, the process of transferring information from an ambulance to the destination hospital takes a lot of time. During this period, the EMS members who are responsible for reporting the information must take their eyes off the patient assessment due to the radio base station on Thai ambulances that are designed to be mounted on the front of the vehicle so that the reporter cannot continuously see and assess the patient’s condition. As a result, the diagnosis of changing symptoms of patients is sometimes delayed, resulting in worsening clinical conditions. Therefore, to shorten that period, smart glasses play an important role in emergency medical operations. Reference Ishikawa, Yanagawa and Ota7,Reference Diaka, Van Damme, Sere, Benova, van de Put and Serneels8 The data can be visible from the ambulance to the hospital with real-time information. This means that EMS staff do not have to take their eyes off patients. Furthermore, smart glasses are used to get the orders directly from the hospital to the ambulance members in case of time-sensitive conditions of the patients, such as cerebrovascular disease, multiple traumas, and cardiac arrest. Doctors on duty at the destination hospitals can see the process of care on an ambulance and provide additional history directly to the team in the ambulance. The suggested treatment can also be provided to ambulance personnel in cases whose symptoms were not clear. The use of smart glasses in EMS is recognized as a form of online medical oversight, aimed at enhancing the efficiency and safety of services delivered to emergency patients. By enabling real-time communication and video streaming, smart glasses allow remote medical professionals to provide guidance, support, and oversight to EMS personnel on the scene.
The primary objective of this study was to compare the duration of patient care in the ambulance between smart glasses and no smart glasses used. The secondary outcome was to identify the type and characteristics of data transfers via smart glasses during EMS operations.
Methods
Design and Setting
This retrospective study was carried out utilizing various EMS units at Srinagarind Hospital, Thailand. The hospital is the primary center in the region for training emergency physicians and EMS technicians with 1,500 EMS (basic level) and 1,000 EMS (advanced level) operations carried out annually. In the EMS unit, there is a dispatch center which operates and controls six ambulances. The smart glasses were implemented in the EMS units starting in 2021. This equipment was new in the health care system. The EMS providers who used smart glasses were well-trained in the instruction of this equipment and no motion sickness was reported during the operations.
Participants
All data on patients treated with an EMS ambulance during the study period and recorded in a closed-circuit television (CCTV) database were collected. Cases with incomplete data and cases where the patients were not found were excluded from this study. Furthermore, cases in which EMS members experienced motion sickness while wearing smart glasses were excluded from this study.
Data Collection
Data were collected from July through December 2021. The data were extracted from four CCTVs, which were provided in the ambulances. In each EMS operation, the data were reviewed on a case-by-case basis in the process of EMS transport being carried out. The EMS practitioners proceeded to transfer the patient to a hospital via ambulance for specialized care and provided medical care during transportation. The primary data obtained were the duration of patient care in the ambulance, which was overseen by three emergency physicians, each with over ten-year experience in EMS. The type of data communication between ambulance and hospital via smart glasses was divided into visual and audio data.
Definition
Transport time is defined as the period of time from when the patient has been placed in the ambulance and ends when the patient’s care is transferred to the destination hospital.
Patient care time is the sub-period of the transport time, defined as the duration during which EMS providers provide medical attention and care to a patient while they are only in the ambulance. It includes the time spent assessing the patient, administering treatments or interventions, monitoring vital signs, and addressing any immediate medical needs or emergencies.
Sample Size
The sample size was calculated based on previous studies. Reference Apiratwarakul, Suzuki and Celebi5 Thus, the authors determined that a sample size of 256 would be required. The statistical analysis was performed with Khon Kaen University’s (Khon Kaen, Thailand) license for IBM SPSS for Windows version 27.0 (IBM Corp.; Armonk, New York USA). The categorical data obtained are presented as frequencies and percentages. Continuous data are presented using the means and standard deviations (SD). The chi-square test was used to assess the relationship between categorical variables. A two-tailed P <.05 was considered statistically significant.
Smart Glasses
The smart glasses were manufactured by The Real Wear Company (Vancouver, Washington USA). It was the HMT-1 model. Android 10.0 was the operating system, and it was connected via Wi-Fi 2.4 GHz and 5 GHz or Bluetooth Low Energy 4.1. The data were from smart glasses including visual and audio with real-time two-way communications. The EMS members who responded to those wearing smart glasses were the team leaders (doctor or nurse; Figure 1).

Figure 1. Smart Glasses on Ambulance.
Ethical Considerations
Ethical approval was provided by the Khon Kaen University Ethics Committee for Human Research (HE651049). Requirement for informed consent from the patients was waived since patient confidentiality protection had been guaranteed, as patients were not identified by name, but by a unique study number.
Results
Over the period of the six-month study, 256 EMS operations were collected from the EMS CCTV database, the characteristics of which are shown in Table 1. A total of 53.1% (N = 68) were male in the smart glasses group. Operation times were most frequent in the afternoon shifts in both groups. In the smart glasses group, non-trauma patients accounted for 68.7% of all cases in the study.
Table 1. Characteristics of the Subjects (N = 256)

The average time from dispatch to vehicle en route (activation time) for the smart glasses and the no smart glasses groups were 1.02 minutes and 1.00 minutes, respectively (P = .442; Table 2). The average patient care time in the smart glasses group was 10.07 minutes, and the no smart glasses group was 5.10 minutes (P <.001).
Table 2. Comparing Service Times between Smart Glasses and Non-Smart Glasses Groups in the Ambulance

a Statistical significance.
The type of visual data communication between the ambulance and hospital via smart glasses primarily accounted for vital signs (100.0%), physical examinations (56.3%), and neurological examinations (42.2%). In Table 3, the primary types of audio data conveyed from ambulance to hospital were gender, age, and chief complaint (100.0%). The study found that the type of audio data transmitted from the hospital to the ambulance showed a significant increase in obtaining patient history (26.6%) and conducting physical examinations (19.5%). This suggested that during the ambulance journey, medical personnel at the hospital provided important information related to the patient’s medical history and instructions regarding physical examinations to be performed.
Table 3. Characteristics of Data Communication via Smart Glasses (N = 128)
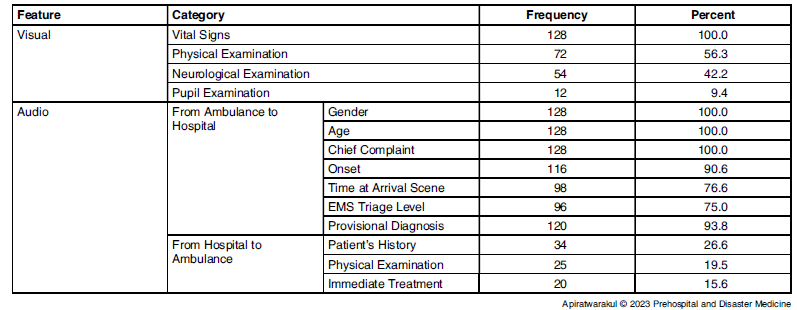
Abbreviation: EMS, Emergency Medical Services.
Discussion
This study focused on the implementation of smart glasses, a new technology that will increasingly be employed in Thailand’s EMS, in order to improve the efficiency of patient care while in the ambulance, and to assist in the capacity of doctors stationed at destination hospitals to transmit patient information and analyze symptoms. Reference Zhang, Joy, Harris, Ozkaynak, Adelgais and Munjal9–Reference Zhang, Ramiya Ramesh Babu, Adelgais and Ozkaynak11 The Faculty of Medicine, Khon Kaen University has been using smart glasses on ambulances since 2021.
The traditional method of transferring information from ambulances to hospitals in Thailand without telemedicine systems is radio. Reference Huabbangyang, Klaiangthong and Prasittichok2,Reference Apiratwarakul, Suzuki and Celebi5,Reference Pattanarattanamolee, Sanglun and Nakahara6 This has been found to have many limitations, such as unclear radio communication, requiring a long time to make contact, confusion over codes used to communicate via radio communication, and no visual aids to help in the assessment of the patient’s physical examination. For these reasons, smart glasses technology has been adopted to solve such problems. Reference Follmann, Ohligs, Hochhausen, Beckers, Rossaint and Czaplik12 The expectation is to more effectively convey information from ambulances, both audio and visual, to accurately assess symptoms and prepare for treatment at the ED.
According to the study, using smart glasses in ambulances increased patient care time more than not using them. The main reason was that the use of smart glasses required personnel stationed in the ambulance to monitor the patient at all times, as well as observe changes and transmit data of vital signs utilizing equipment installed on the ambulance. As a result, when there was a change in the patient’s condition, the personnel in the ambulance were able to assess the condition in a timely manner. Furthermore, the increased period of care for patients in the ambulances demonstrated that unnecessary time was effectively reduced because EMS members no longer had to rely solely on radio communication to report patient information, which was prone to errors. Therefore, the adoption of smart glasses technology in EMS will support more effective patient evaluation, diagnosis, and treatment with reduced duration of time. Moreover, the use of smart glasses did not affect the delay of the scene time and transport time due to the EMS members wear the equipment during the moving ambulance.
Types of communication data transmitted through smart glasses can be divided into two categories: visual and audio data. In the field of visual information, referral of information from the ambulance to the destination hospital with patient vital signs and physical examinations are provided to doctors stationed at the destination hospitals. In addition, if necessary, specific medical equipment at the ED will be prepared ahead of patient arrival.
In the field of audio data, there is a two-way communication route; from the ambulance to the hospital, and from the destination hospital is also transferred to the personnel in the ambulance. In accordance with the standards of EMS operations in Thailand, personnel on board the ambulance will report preliminary patient information consisting of gender, age, chief complaint, and onset, which is important information to the hospital. There is also a provisional diagnosis from EMS members in an ambulance.
The use of smart glasses in EMS creates an additional channel for the transfer of essential information from the destination hospital to the ambulance, especially for medical history, physical examinations, and treatment. Reference Zhao, Heida, van Wegen, Bloem and van Wezel13,Reference Boillat, Grantcharov and Rivas14 In the case where initial diagnosis is not possible, further medical examination will be required, which has a positive effect. This allows the patient to be diagnosed quickly. In addition, in cases where resuscitation is needed, the doctor stationed at the destination hospital can also order immediate treatment in the ambulance. The procedure in the ambulance (chest compression, prehospital point-of-care ultrasound, and endotracheal intubation), with the guidance and monitoring from the staff at the hospital, will allow the EMS members to have more confidence to perform these procedures. Reference Ienghong, Cheung, Tiamkao, Bhudhisawasdi and Apiratwarakul1,Reference Huabbangyang, Klaiangthong and Prasittichok2,Reference Pattanarattanamolee, Sanglun and Nakahara6
Development of Thailand’s EMS by using modern technology has always and will continue to play an important role in public health policy. Efficient communication equipment and communication networks will change the treatment guidelines in ambulances to be more convenient, faster, and more efficient in response to the ever-growing needs of society, ensuring sustainable development, and increasing service safety records. Reference Suryanto and Boyle15,Reference Chowdhury, Mok and Leenen16
Limitations
This study analyzes operational data in the EMS through a CCTV database recorded through cameras installed on ambulances. It relies on experienced doctors who make judgment calls and analyze the duration time of EMS operations. In addition, efficient databases with clear audio and visual aids are an important factor in the data analysis.
The characteristics of EMS in each country vary in terms of personnel, vehicles, and treatment guidelines, so the use of information depends on such key factors.
Conclusions
The implementation of smart glasses increased patient care time in EMS ambulances and created effective channels of real-time two-way communication between ambulance and hospital.
Conflicts of interest/funding
This research was supported by the Fundamental Fund of Khon Kaen University which has received funding support from the National Science, Research, and Innovation Fund (NSRF). No conflicts of interest were declared.
Acknowledgments
The authors would like to express their sincere gratitude to Josh Macknick for acting as an English consultant. They would additionally like to acknowledge Prof. Wanida Kanarkard and her colleagues from the Department of Computer Engineering, Faculty of Engineering, for providing the smart glasses used in this study.





 Open access
Open access