Dietary pattern analysis has become a popular method for studying overall diet and associations between diet and disease risk. Pre-specified indices are used to measure adherence to recommendations or diets with hypothesised health implications, whereas data-driven methods, often factor or cluster analysis, are applied to identify underlying food patterns in a population empirically( Reference Hu 1 , Reference Balder, Virtanen and Brants 2 ). Participants’ adherence to the dietary patterns can then serve as a holistic measure of their diet in assessment of diet–disease relationships. Such a holistic approach has several methodological advantages, as it includes unexplored dietary factors and nutrient interactions and increases the chance of detecting small but meaningful associations as they add up in the context of a whole diet, and at the same time not impeded by the disadvantages of correlated intakes( Reference Hu 1 , Reference Jacques and Tucker 3 ). Indeed, throughout the past decades, dietary patterns have been related to multiple health outcomes, mainly morbidity and mortality from CVD and cancer, longevity and neurodegenerative diseases( Reference Wirfalt, Drake and Wallstrom 4 – Reference Schulze and Hoffmann 11 ). From the perspective of public health promotion, dietary patterns reflect the foods commonly consumed together. Hence, promoting healthy dietary patterns, in addition to targeted food-based dietary guidelines, might be a useful approach in order to improve diet and health in a population. Understanding the underlying dietary habits in the population and the associations with lifestyle and demographic characteristics is also valuable for identifying risk groups and to pinpoint strategic implementations.
Principal component analysis (PCA), a data reduction method, has been used with data from different countries and cultures to identify dietary patterns in specific populations. In Swedish settings, cluster analysis( Reference Berg, Lappas and Strandhagen 12 – Reference Winkvist, Hornell and Hallmans 14 ) rather than PCA have been more commonly applied( Reference Terry, Hu and Hansen 15 ). Data from Swedish cohort studies have been included in multicounty studies that used PCA to identify dietary patterns( Reference Balder, Virtanen and Brants 2 , Reference Engeset, Hofoss and Nilsson 16 , Reference Bamia, Orfanos and Ferrari 17 ). However, data-derived dietary patterns have previously not been identified in a nationally representative sample of the Swedish population. The aim of this study was (1) to use PCA to derive dietary patters in the Swedish National Food Agency’s (NFA) most recent national dietary survey in adults, Riksmaten 2010–11, (2) to examine the characteristics of individuals adhering to identified dietary patterns and (3) to characterise the nutrient and food profile of those dietary patterns.
Methods
Participants
Riksmaten is a population-based Swedish dietary survey conducted by the NFA. Riksmaten adults 2010–11 was carried out between May 2010 and July 2011 and included Swedish residents aged 18–80 years. Population sampling and fieldwork was carried out by Statistics Sweden on behalf of the NFA. Sampling was made by proportional allocation based on vital statistics and in strata of sex, age and region for the main sample (n 3995). For an additional sample who were invited to also participate in a parallel biomonitoring study, sampling was done according to affiliation to Swedish Occupational and Environmental Medicine Centres (n 1008). Out of the total 5003 men and women identified, fifty-three individuals had died or moved out of Sweden after the sampling was made, leaving 4950 individuals. Participation rate was 46 % for any of the included parts (i.e. food record, lifestyle questionnaire and (or) biomonitoring) and 36 % for the food record (n 1797, 56 % women), which was the inclusion criteria in the current study. Individuals were excluded from our analyses if reporting extreme energy intakes: women <2092 (n 5) or >14 644 kJ/d (n 5) (corresponding to <500 and >3500 kcal/d) and men <3347 (n 6) or >16 736 kJ/d (n 8) (corresponding to <800 and >4000 kcal/d). In addition, twenty-five women reporting being pregnant and eighteen women currently breast-feeding were also excluded, as they were presumably not following their usual diet. Women with missing data on pregnancy and lactation status (n 46) were assumed not to be pregnant nor breast-feeding, and they were kept in the study. The final study population consisted of 952 women and 778 men (of whom 277 individuals were sampled according to the procedure for the parallel biomonitoring study).
In sensitivity analyses, we excluded individuals categorised as low (156 women and 159 men) or high (one woman) energy reporters (for simplicity referred to as misreporters of energy intake), as identified by the Goldberg equation modified by Black( Reference Black 18 ). The procedure, which compares reported energy intake with estimated energy expenditure, has previously been described for the Riksmaten population( 19 ). A total of sixteen individuals did not have information on body weight, and evaluation of their energy intake was not possible; these individuals were consequently also excluded in the sensitivity analyses. The subpopulations of acceptable energy reporters then consisted of 788 women and 610 men.
The study was approved by the Regional Ethical Review Board of Uppsala, and all participants gave oral informed consent before entering the study.
Dietary assessment
Diet intake was assessed by a self-reported estimated web-based food record during 4 consecutive days (Livsmedelssystemet, application 04.1). Participants were given oral (by telephone) and written instructions for recording their intake. Written information included photographs for estimation of portion size. Participants without access to the web-based food record could report by telephone to interviewers. The web-based food record was connected to a survey-specific NFA food composition database (Livsmedelsdatabasen version Riksmaten adults 2010–11), which included approximately 1900 food items. Dietary intakes and energy and nutrient content were derived directly from the system.
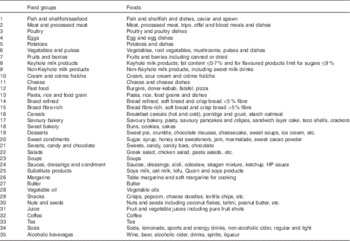
Food intake was categorised into thirty-five food groups based on culinary use and nutrient composition (Appendix 1). To distinguish similar foods with different nutrient profiles, milk products were categorised into two groups: depending on whether they were in compliance with the Nordic Keyhole label( 20 ). The Keyhole is an NFA-labelling scheme, which guides healthy food choices. For milk and yogurt to meet the criteria for the Keyhole, fat content has to be limited to a maximum of 0·7 %, and for flavoured products there is an additional limit for sugars: a maximum of 9 %. Bread was separated into refined bread or bread rich in whole grain and fibre. Breads categorised as fibre-rich had a minimum of 5 % fibre. Unspecified Swedish crisp bread was also included in this category, as most crisp breads have high fibre content. Some foods were kept in separate groups, as they may represent distinct food choices (e.g. butter, margarine and vegetable oils) or simply did not fit into other food groups (e.g. potatoes, coffee, tea).
Background information and covariate assessment
Demographic data (sex, age, educational level, income and living area) were retrieved from the Swedish population register. A web-based questionnaire was used to collect information on residential and lifestyle factors (including some additional dietary information, not included in this study). Education was categorised as high if a university or college degree had been completed, or else it was categorised as low. Income was either above (high) or below (low) sex-specific median income. Living area was classified as urban or rural region, and single household as yes or no. Individuals were considered as either current smokers or non-smokers. BMI (kg/m2) was calculated on the basis of self-reported body weight and height. Physical activity was assessed in two questions: one estimating leisure-time and one estimating work-time physical activity. Answers were given on a four-grade scale, which previously have been given physical activity levels and successfully validated against doubly labelled water( Reference Johansson and Westerterp 21 ). Work-time physical activity was considered sedentary or moderate and leisure-time physical activity was considered sedentary or regular.
Statistical methods
Deriving dietary patterns
Dietary patterns were derived by PCA, which reduces larger amounts of observed variables to a smaller number of principal components, while maximising the variance and identifying structures in the observed data. PCA was based on linear correlation and performed with the ‘pca’ command in STATA (Intercooled STATA 11.0 for Windows; StataCorp LP). We derived dietary patterns separately in men and women, as men and women may have different dietary patterns( Reference Newby and Tucker 5 ). Intake was expressed in g/d, for the thirty-five food groups described above.
The PCA outputs were evaluated on the basis of eigenvalues, scree plots and interpretation of retrieved components, and then repeated with the number of components to keep specified. Identified components were rotated with varimax rotation creating orthogonal, uncorrelated factors. Individuals were assigned a score for each of the retained factors. These ‘factor scores’ were based on the sum of the products of the factor loadings multiplied with the reported intakes of the specific food group. The naming of the dietary patterns, where based on the interpretation of the factors, was founded on nutritional and domestic-cultural knowledge.
To limit the potential effect of non-random misclassification because of misreporting of dietary intakes, we conducted sensitivity analyses in which we repeated the PCA including only acceptable energy reporters (described above).
Subject characteristics and dietary patterns
Distribution of population demographic and lifestyle factors were assessed by quintiles of factor scores (in which the highest quintile represents the individuals with the highest score) and tested for trend in regression analysis with the score quintiles applied as continuous variables. Because of missing data on demographic and lifestyle variables, the study population in the above analyses was reduced with between zero and fifty-four observations in women and zero and eighty in men. Distribution of low-energy reporters, food intake (g/d) and selected nutrient densities (e.g. per MJ) were also examined by quintiles of dietary pattern scores and tested for trend with the same method as above. Correlations between dietary pattern score and energy intake was tested with Pearson’s correlation. In addition, correlations between dietary patterns and nutrient intake (energy contribution from macronutrients and energy-adjusted intake of micronutrients and cholesterol) were examined with Spearman’s rank correlation, because of data not normally distributed. The correlational analyses were also stratified by age (18–30, 31–44, 45–64 and 65–80 years). All analyses were performed in STATA statistical software with significance level set to 0·05.
Results
Dietary patterns
On the basis of scree plots, eigenvalues and the interpretability of the identified factors, we derived three patterns in women, explaining 19 % of the total variance, and two patterns in men, explaining 13 % of the total variance.
Table 1 shows food group loadings and explained variances for each derived dietary pattern. The loadings can be interpreted as the correlation between the food group and the pattern. The first two patterns were similar in men and women. The first pattern was characterised by high intake of vegetables, fruits and berries, fish and seafood, eggs, hot and cold cereals, and vegetable oils and lower intakes of fast food, refined bread and soda, in both sexes. This pattern was named the ‘healthy pattern’. The second pattern was characterised by intake of traditional Swedish foods such as potatoes, meat and processed meat, sauces (including dressings and condiments), non-Keyhole milk products, sweet bakery products, sweet condiments, desserts and margarine, and lower intake of fast food. This second pattern was named the ‘Swedish traditional pattern’. In women, a third interpretable pattern was derived; this pattern loaded positively on fibre-rich bread, cheese, rice, pasta and food grain dishes, substitute products for meat and dairy products, soya and oat milk, soya, tofu and Quorn (a meat substitute product based on mycoprotein) products, margarine, sweets and candies, snacks, tea, but negatively on potatoes and coffee. This third pattern was named ‘light-meal pattern’.
Table 1 Dietary patterns and rotated (varimax rotation) factor loadings

* Food groups are throughout defined and exemplified in Appendix 1.
† Loadings above 0.15 or less than −0.15.
‡ For milk products, the Swedish National Food Agency Keyhole symbol identifies options that contain less fat and less sugar; fat content has to be limited to maximum 0·7 % and for flavoured products there is an additional limit for sugars, a maximum of 9 %.
§ Fibre-rich bread had a minimum of 5 % fibre; unspecified Swedish crisp bread was also included in this category, as most crisp breads have high fibre content. Bread with fibre content <5 % was considered refined.
∥ Substitute products, used as substitutes for dairy products, meat, fish and so on, includes, for example, soya and oat milk, soya protein and Quorn.
¶ Total variance explained by the derived components: in women 19 % and in men 13·3 %.
In sensitivity analyses, excluding misreporters of energy intake from the PCA did not notably change the patterns derived in women, or the first (healthy) pattern in men. The second pattern in men changed somewhat and yielded additional negative loadings (greater than −0·15): for poultry, rice, pasta and food grain dishes, snacks and nuts and seeds when misreporters were excluded. Still, the interpretation of the pattern as a Swedish traditional dietary pattern remained.
Subject characteristics and dietary patterns
Demographic and lifestyle factors per quintile of factor score are presented in Table 2. Among women, the healthy pattern was positively associated with education and income. Men and women with high healthy pattern score were older, less likely to smoke and more likely to be physically active on their spare time. On the other hand, the Swedish traditional pattern was associated with lower education and living in rural areas, and older age, in both men and women. In men, the Swedish traditional pattern was also associated with less spare-time physical activity. High light-meal pattern score was associated with younger age, lower BMI, living in urban areas, not smoking and having a higher education.
Table 2 Demographic and lifestyle factors per quintile (Q) of dietary pattern scores in women (n 952) and men (n 778) (Numbers and percentages; medians and interquartile ranges (IQR, 25th; 75th percentiles))

† P for trend in regression analysis, with the score Q applied as continuous variables: * P<0·05, ** P<0·01, *** P<0·001.
‡ P=0·050.
For all patterns derived, the proportion of low-energy reporters decreased with higher dietary pattern score (Table 2). Moreover, all pattern scores, except for the healthy pattern score in women, were positively correlated to energy intake; the healthy pattern in men (r 0·26), the Swedish traditional pattern in both men (r 0·38) and women (r 0·51) and light-meal pattern in women (r 0·41) (all P<0·0001).
Food and nutrient intake
Correlations for the two major patterns, identified in both men and women, and nutrient intakes were similar in both sexes. In summary, the healthy pattern was (with all P≤0·0001) positively correlated with fibre intake (r 0·58 and 0·51, in women and men, respectively), n-3 fatty acids (r 0·25 and 0·31) and negatively correlated to added sugar, in women (r −0·39). The Swedish traditional pattern was (with all P values<0·0001) positively correlated with, for example, added sugar (r 0·20 in women and r 0·25 in men) and SFA (r 0·13 and 0·21) and negatively with protein (r −0·22 and −0·25, in women and men, respectively) and fibres, the latter in men only (r −0·22). The macronutrient profile of this pattern and the light-meal pattern in women were quite similar, except for the correlation between the Swedish traditional pattern and SFA not present for the light-meal pattern (data not shown). The healthy pattern was positively correlated with most micronutrients, whereas the Swedish traditional pattern and the female light-meal pattern showed mainly negative correlations (data not shown; details on nutrient composition are given in Table 3). Correlations did not differ substantially between age groups for any of the dietary patterns (results from age-stratified analyses not shown). In Table 3, the macronutrient and micronutrient qualities of the dietary patterns are further demonstrated in quintiles of dietary pattern score. High agreement with the healthy dietary pattern was associated with higher nutrient density. High score on the Swedish traditional pattern was associated with lower density of Fe, Se and folate, and in men also dietary fibre. The nutrient profile of the light-meal pattern was also less favourable, with lower Fe, Se, folate and vitamin D density in participants with high light-meal pattern score (Table 3). Online Supplementary Table S1 shows details on food intakes (g/d) in quintiles of dietary pattern scores.
Table 3 Nutrient densities in quintiles (Q) of dietary pattern scores in women and men (Mean values and standard deviations)

E%, percentage of total energy.
† P for trend in regression analysis, with the score Q applied as continuous variables: * P<0·05, ** P<0·01, *** P<0·001.
Discussion
In this, the first study that derived dietary patterns from PCA in a nationally representative adult Swedish population, we identified two dietary patterns common in both Swedish men and women: a healthy dietary pattern and a Swedish traditional dietary pattern. In addition, a third light-meal pattern was pronounced only in women.
Dietary patterns in different populations
Dietary patterns similar to our healthy dietary pattern, with positive loadings on foods generally considered healthy such as fruit and vegetables, fish, whole-grain cereals, vegetable oil, etc., have been identified in other populations( Reference Newby and Tucker 5 , Reference Knudsen, Matthiessen and Biltoft-Jensen 22 – Reference Fung, Rimm and Spiegelman 26 ). These patterns are often named ‘healthy’, ‘prudent’ or ‘vegetable’ patterns. The Swedish traditional pattern identified in this study is also similar to what has been reported as traditional patterns in other populations( Reference Knudsen, Matthiessen and Biltoft-Jensen 22 , Reference Beaudry, Galibois and Chaumette 24 , Reference Togo, Osler and Sorensen 27 – Reference Schulze, Hoffmann and Kroke 31 ). Commonly, these patterns load on, for example, meat and meat products, sauce and potatoes and often bread and margarine, and sometimes sweet bakery products and coffee. There are also similarities between our Swedish traditional pattern and the so-called Western dietary patterns frequently identified in modern industrialised populations. However, there are also some important differences. Above all, our traditional pattern loaded negatively on fast food and it did not load on soda, butter or snacks, contrary to what is seen for many Western dietary patterns( Reference Newby and Tucker 5 , Reference Osler, Heitmann and Gerdes 23 , Reference Fung, Hu and Fuchs 25 , Reference Fung, Rimm and Spiegelman 26 ).
In the Swedish Mammography Cohort (SMC), a ‘healthy pattern’ (loading positively on e.g. vegetables and fruits, fish, cereals and eggs, poultry, whole grain, low-fat dairy products and juice) and a ‘Western pattern’ similar to our Swedish traditional pattern (loading positively on meat, potatoes, high-fat dairy products and sweets, refined grains and margarine, but also soda and snack) were found( Reference Terry, Hu and Hansen 15 ). The third pattern in the SMC, however, loaded above all on alcoholic beverages and was not comparable with our light-meal pattern. Dissimilarities might be because of the diversities between the populations and the homogeneous population in the SMC (women 40–74 years old), as well as the fact that SMC data were collected more than 20 years before our dietary survey.
The Swedish traditional and healthy patterns in this study clearly resembles the ‘traditional’ and ‘health-conscious pattern’, recently identified in a nationally representative Danish sample( Reference Knudsen, Matthiessen and Biltoft-Jensen 22 ), underlining the similarities in food habits in these two Nordic countries. However, the third pattern identified by Knudsen et al.( Reference Knudsen, Matthiessen and Biltoft-Jensen 22 ), was a ‘fast food pattern’, loading on pizza, hamburgers, crisps, sugar-sweetened beverages and sweets, with few similarities to our light-meal pattern. In the Nordic HELGA project, which included data from the Swedish Västerbotten Intervention Program, Nordic and country-specific dietary patterns were derived( Reference Engeset, Hofoss and Nilsson 16 ). One of the major patterns identified was a ‘bread and potatoes’ pattern similar to our Swedish traditional pattern (with high loadings for potatoes, processed meat, white and crisp bread, margarine, sweet condiments, as well as cakes and biscuits); this pattern persisted also when using only Swedish data( Reference Engeset, Hofoss and Nilsson 16 ). From a European perspective, including older participants (>60 years) from the European Prospective Investigation into Cancer and Nutrition (EPIC) study, two patterns were identified by PCA: a vegetable-based pattern and a sweet- and fat-dominated diet, with some similarities to our healthy and Swedish traditional patterns( Reference Bamia, Orfanos and Ferrari 17 ). Balder et al.( Reference Balder, Virtanen and Brants 2 ) used four EPIC populations (among them the SMC) and derived patterns by exploratory factor analysis. Two patterns were consistent through all populations, a ‘vegetable pattern’ and a ‘pork, processed meat and potatoes’ pattern, with characteristics similar to our healthy and Swedish traditional patterns( Reference Balder, Virtanen and Brants 2 ). Additional patterns were derived, but these were country specific; in the Swedish population, the additional patterns were an alcohol pattern and a margarine/butter substitution pattern.
It might be that there are some principal dietary patterns that are universal, but in addition there are less distinct patterns that are country, culture and population specific. However, all studies using PCA differ somewhat in methods of dietary data collection (e.g. FFQ v. a more detailed food record), food grouping, the number of groups included, the unit of the food groups used and so on. Therefore, direct comparison of results is challenging.
The dietary patterns identified in our Swedish population were clearly associated with other lifestyle and demographic variables. Individuals with more pronounced healthy dietary pattern were also more likely to have other healthy habits and higher socio-economic status. In contrast, high agreement with the Swedish traditional dietary pattern was associated with lower education. In the Danish national sample, the dietary patterns were derived for men and women simultaneously; however, their health-conscious dietary pattern was associated with female sex, older age and education, and their traditional pattern was associated with male sex and older age( Reference Knudsen, Matthiessen and Biltoft-Jensen 22 ). Similar associations as in our study were found between the vegetable-based dietary pattern in EPIC-Elderly and population characteristics – for example positive to educational level, physical activity and not smoking – and also between total energy intake and higher BMI. The sweet-and fat-dominated pattern in the same study was also associated with total energy intake but inversely associated with physical activity( Reference Bamia, Orfanos and Ferrari 17 ). Associations between dietary patterns and demographic and lifestyle factors has also been reported from other EPIC populations( Reference Schulze, Hoffmann and Kroke 32 , Reference Engeset, Alsaker and Ciampi 33 ). In the Nurses’ Health Study, a prudent dietary pattern was, similar to our healthy dietary pattern, associated with higher physical activity and not smoking; opposite associations were seen for these parameters and a Western dietary pattern in the same study( Reference Fung, Hu and Holmes 34 ). Associations between data-derived dietary patterns and lifestyle and demographic factors have been reported in various populations, as reviewed by Newby & Tucker( Reference Newby and Tucker 5 ). As a result, it has been suggested that dietary patterns might represent more than just the diet( Reference Nyholm, Lissner and Hornell 35 , Reference Martinez, Marshall and Sechrest 36 ). Regardless, our results indicate that a healthy diet is seemingly more accessible for parts of the Swedish community, related to socio-economic factors.
Public health relevance
In the present study, we identified a major dietary pattern of foods generally considered healthy and with favourable nutrient quality, in the Swedish population. However, our study also shows that the traditional Swedish food habits are important.
The non-communicable diseases burdening public health today are complex diseases that are generally not explained by a single biological mechanism, food or nutrient, but an aetiology including nutrition and lifestyle in a more complex context (of genetic background, etc.). Food patterns and hence the whole diet should be scrutinised for opportunities to change towards a more healthy entity.
Strengths and limitations
A major strength of this study is its national sample and broad age range. However, a limitation of the Riksmaten adults 2010–11 is the low participation rate. Decreasing response rate is a documented problem in population surveys( 37 , Reference de Heer 38 ). In Riksmaten adults 2010–11, non-participation was higher among young men aged 18–30 years (77 %) and non-native Swedes (73 %)( 19 ). Educational level differed between participants (41 % university/college degree) and non-participants (27 % university/college degree), and income level was also somewhat higher among participants compared with non-participants( 19 ). The representativeness of the derived dietary patterns for the general Swedish population might therefore be somewhat limited.
Food records over 3–7 d are considered gold standard for dietary data collection, and preferable in capturing day-to-day variation compared with FFQ and diet history. Nonetheless, longer-term day-to-day variation in food intake is less well covered. Still, good consistency between patterns based on FFQ and food records have been reported( Reference Hu, Rimm and Smith-Warner 39 – Reference Togo, Heitmann and Sorensen 41 ).
Our dietary patterns explained a limited amount of the total variance in dietary intake (between 5·4 and 7·6 %); however, this was similar to what has been reported from other studies( Reference Beaudry, Galibois and Chaumette 24 , Reference Schulze, Hoffmann and Kroke 32 , Reference Newby, Muller and Hallfrisch 42 ). The amount of variance explained has been shown to be largely dependent on the number of food groups included in the analysis( Reference McCann, Marshall and Brasure 43 ).
As in most dietary surveys, under-reporting existed. We choose to perform sensitivity analyses excluding misreporters of energy intake to investigate whether our patterns were affected by a non-random under-reporting. However, the dietary patterns derived were largely consistent.
Conclusion
This study indicates that there are two major dietary patterns in the Swedish adult population: a healthy pattern and a Swedish traditional pattern, similar to dietary patterns identified in other populations. In addition, a light-meal pattern with alternative food choices was identified in women. The patterns can be further used for examining the association between whole diet and health outcomes.
Acknowledgements
This project would not have been possible without the goodwill of the participants of the Riksmaten adults 2010–11 survey, who deserve the greatest thanks for their time and effort.
This project was supported by FORTE: Swedish Research Council for Health, Working Life and Welfare (2011-1166), and by Henning and Johan Throne-Holsts Foundation, whose financial support enabled the cooperation between Uppsala University and Harvard T.H. Chan School of Public Health. The funders had no role in the design, analysis or writing of this article.
The project was led by E. A. who also processed the data for the current study, performed the analyses and was responsible for writing the manuscript. Authors contributed as follows – acquisition of data: E. W. L., W. B. and A. K. L.; study concept and design: E. A., T. T. F., P. S., A. K. L., W. B., A. A. and T. C.; preparation of data: E. A., T. T. F. and E. W. L.; statistical analysis and interpretation of data: E. A. and T. T. F.; drafting of the manuscript: E. A.; critical revision of the manuscript for content and form, and final approval: all authors; administrative, technical or material support: E. A., E. W. L. and T. C.
The authors declare no conflicts of interest.
Supplementary material
For supplementary material/s referred to in this article, please visit http://dx.doi.org/doi:10.1017/S0007114515004110