



The increasing average life expectancy, the prevalence of chronic diseases and disabilities, and an underfunded, fragile, and fragmented healthcare system have contributed to a growing demand for informal care (Schulz et al., Reference Schulz, Beach, Czaja, Martire and Monin2020; United Nations Entity for Gender Equality and the Empowerment of Women [UN Women], 2018).
Despite the growing body of literature on the challenges faced by informal caregivers, too little attention has been given to understanding the social perceptions towards this group. Analyzing how informal caregivers are socially perceived is crucial, as negative perceptions can adversely affect their health and well-being, preventing them from receiving the necessary support and ultimately impacting the quality of care they provide (e.g., Ali et al., Reference Ali, Hassiotis, Strydom and King2012). Indeed, there is evidence that informal caregivers remain invisible, unacknowledged, and undervalued by society (Ansello & Rosenthal, Reference Ansello and Rosenthal2007; EUROCARERS, 2019), even though unpaid care work is crucial to economic activity and societal well-being (Peña-Longobardo & Oliva-Moreno, Reference Peña-Longobardo and Oliva-Moreno2022; UN Women, 2018).
The present research presents two experimental studies aimed at better understanding whether and under which conditions informal caregivers are dehumanized.
Informal Care Work
Informal care refers to unpaid care work provided by family members, friends, or neighbors to individuals with physical, mental, or cognitive limitations (EUROCARERS, 2019; Hoffmann & Rodrigues, Reference Hoffmann and Rodrigues2010; Schulz et al., Reference Schulz, Beach, Czaja, Martire and Monin2020). Societal perceptions that often link caregiving to women’s nature result in a disproportionate representation of women (e.g., wives, daughters, and daughters-in-law) in unpaid care work (e.g., Erreguerena, Reference Erreguerena2015; Esplen, Reference Esplen2009; United Nations of Economic and Social Affairs-Population Division, 2019). Nevertheless, men, especially those in the LGBTQ+ community, are also stepping into the role (e.g., Hughes & Kentlyn, Reference Hughes and Kentlyn2011). Moreover, the informal caregiving role predominantly falls on middle-aged individuals, unemployed or domestic workers, and those with lower education and socioeconomic status (Verbakel et al., Reference Verbakel, Tamlagsrønning, Winstone, Fjær and Eikemo2017).
Informal caregivers perform several tasks that, in some cases, require professional skills and high levels of vigilance (Lindeza et al., Reference Lindeza, Rodrigues, Costa, Guerreiro and Rosa2020). They typically provide assistance with activities of daily living (ADLs) (e.g., personal hygiene, dressing, and eating), as well as instrumental activities of daily living (IADLs) (e.g., housework, meal preparation, shopping, or administrative tasks) (Hoffmann & Rodrigues, Reference Hoffmann and Rodrigues2010). Working in such a complex and unpredictable environment can be challenging for informal caregivers, affecting their personal, professional, financial, and social life (e.g., poverty, and social isolation), which is reflected in their health and well-being (e.g., anxiety, depression, and burnout) (Schulz et al., Reference Schulz, Beach, Czaja, Martire and Monin2020, for a review).
Moreover, some studies (e.g., Abojabel & Werner, Reference Abojabel and Werner2019; Kinnear et al., Reference Kinnear, Link, Ballan and Fischbach2016; McGown & Braithwaite, Reference McGown and Braithwaite1992; Yip & Chan, Reference Yip and Chan2022; Zwar et al., Reference Zwar, Angermeyer, Matschinger, Riedel-Heller, König and Hajek2020) have recognized informal caregivers as targets of courtesy stigma (i.e., negative stereotypes, prejudice, and discrimination from the general public due to their association with a stigmatized individual or group) (Goffman, Reference Goffman1963). For instance, McGown and Braithwaite (Reference McGown and Braithwaite1992) found that nurses and the general public tended to perceive informal caregivers of stroke patients as emotionally unstable and incompetent in understanding the care recipient’s condition. Similarly, Kinnear et al. (Reference Kinnear, Link, Ballan and Fischbach2016) and Yip and Chan (Reference Yip and Chan2022) showed that informal caregivers of children with autism spectrum disorder were perceived as incompetent in caring for their children and blamed for their deficits, resulting in high self-stigma, stress, depression, and anxiety. Furthermore, Abojabel and Werner (Reference Abojabel and Werner2019) and Zwar et al. (Reference Zwar, Angermeyer, Matschinger, Riedel-Heller, König and Hajek2020) showed the existence of devaluing and accusative cognitions, disgusted emotions, and behaviors of distance and avoidance towards informal caregivers of elderly individuals.
We believe that the failure to recognize the important contributions of such an important group may be not only a result of complex factors rooted in gender roles (e.g., Erreguerena, Reference Erreguerena2015; Poole & Isaacs, Reference Poole and Isaacs1997) and the stigma faced by care recipients and informal caregivers, but also a consequence of the fact that informal caregivers are dehumanized.
Humanness and Dehumanization
Dehumanization refers to the act of denying individuals their humanness by perceiving or treating them as less than fully human beings (Haslam, Reference Haslam and Kronfeldner2021; Haslam & Loughnan, Reference Haslam and Loughnan2014). This phenomenon is closely associated with categorizing individuals based on personality traits and emotions (Haslam & Stratemeyer, Reference Haslam and Stratemeyer2016).
The Dual Model of Dehumanization (Haslam, Reference Haslam2006) focuses on personality traits as indicators of people’s humanness. In this model, humanness is understood as comprised of uniquely human traits (e.g., rationality, civility, refinement) that distinguish human beings from other animal species due to their emergence later in human development and susceptibility to cultural variation; and by traits that represent the core essence of human nature (e.g., warmth, emotionality, openness) because they are shared by all human beings as they emerge early in human development and remain consistent across different cultures. When individuals or groups are denied uniquely human traits, they are treated or perceived as primitive and irrational animals (animalistic dehumanization); when individuals or groups are denied human nature traits, they are treated or perceived as robots, automatons, or objects (mechanistic dehumanization) (Haslam, Reference Haslam2006).
The Infrahumanization Theory (Leyens et al., Reference Leyens, Paladino, Rodriguez-Torres, Vaes, Demoulin, Rodriguez Perez and Gaunt2000, Reference Leyens, Rodriguez-Perez, Rodriguez-Torres, Gaunt, Paladino, Vaes and Demoulin2001) conceptualizes humanness through the attribution or denial of specific emotions to other people. According to this theoretical framework, secondary emotions (e.g., shame, hope, resentment) are considered uniquely human because they require higher cognition and morality, characteristics that develop later in life and are culturally variable. In contrast, primary emotions (e.g., fear, pain, pleasure) are shared by both humans and animals because they tend to manifest early in development (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004). Several studies within this model have shown that people reserve secondary (uniquely human) emotions for the ingroup while denying them to the outgroup. Conversely, primary emotions are usually equally attributed to both groups (Leyens et al., Reference Leyens, Demoulin, Vaes, Gaunt and Paladino2007; Paladino et al., Reference Paladino, Leyens, Rodriguez, Rodriguez, Gaunt and Demoulin2002; Vaes et al., Reference Vaes, Leyens, Paladino and Miranda2012, for a review). This effect remains independent of negative attitudes and ingroup favoritism (Cortes et al., Reference Cortes, Demoulin, Rodriguez, Rodriguez and Leyens2005; Paladino et al., Reference Paladino, Leyens, Rodriguez, Rodriguez, Gaunt and Demoulin2002, Reference Paladino, Vaes, Castano, Demoulin and Leyens2004). The denial of secondary (uniquely human) emotions to individuals or groups aligns with animalistic dehumanization (Haslam, Reference Haslam2006), as represents a subtle form of dehumanization in which individuals or groups are perceived as being close to animals (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004; Haslam, Reference Haslam and Kronfeldner2021).
Dehumanization is a prevalent phenomenon that impacts a wide range of individuals across various intergroup and interpersonal contexts (e.g., school, work, or society at large) (Haslam, Reference Haslam and Kronfeldner2021, for a review). Examples include dehumanizing attitudes and behaviors towards stigmatized groups, such as disabled individuals (e.g., Betancor et al., Reference Betancor, Ariño Mateo, Rodríguez-Pérez and Delgado Rodríguez2016; Martinez et al., Reference Martinez, Piff, Mendoza-Denton and Hinshaw2011), elderly individuals (e.g., Boudjemadi et al., Reference Boudjemadi, Demoulin and Bastart2017), women (e.g., Fiske et al., Reference Fiske, Cuddy, Glick and Xu2002; Tipler & Ruscher, Reference Tipler and Ruscher2019), and low-status or low-income occupational groups (e.g., Volpato et al., Reference Volpato, Andrighetto and Baldissarri2017).
Indeed, evidence suggests that individuals with Down syndrome, compared to those without Down syndrome, are denied uniquely human emotions by professional educators and the general public (e.g., Betancor et al., Reference Betancor, Ariño Mateo, Rodríguez-Pérez and Delgado Rodríguez2016). Similarly, Martinez et al. (Reference Martinez, Piff, Mendoza-Denton and Hinshaw2011) found that individuals with mental illness are dehumanized, and consequently perceived as dangerous and socially rejected. Moreover, Boudjemadi et al. (Reference Boudjemadi, Demoulin and Bastart2017) demonstrated that older individuals tend to be attributed fewer uniquely human traits and emotions and more associated with animal-related words than younger individuals. The animalistic dehumanization also extends to certain subcategories of women, such as those in traditional roles (e.g., housewives and mothers), who are typically perceived with a lack of uniquely human traits (e.g., Fiske et al., Reference Fiske, Cuddy, Glick and Xu2002), and implicitly associated with animals, particularly when their sexual and reproductive functions are emphasized (e.g., Tipler & Ruscher, Reference Tipler and Ruscher2019). Furthermore, individuals in low-status or low-income occupations are animalistically dehumanized, as they are attributed with fewer uniquely human traits and are associated with animal metaphors (e.g., animals, gorillas, savage beasts) (e.g., Volpato et al., Reference Volpato, Andrighetto and Baldissarri2017).
To the best of our knowledge, no research has examined whether informal caregivers are dehumanized compared to individuals who do not assume this role. Nevertheless, given that the profile and work environment of informal caregivers (e.g., unpaid work, mainly performed by women, involving the care of disabled individuals), share similar characteristics with dehumanized groups (e.g., Sakalaki et al., Reference Sakalaki, Richardson and Fousiani2017; Volpato et al., Reference Volpato, Andrighetto and Baldissarri2017), it is plausible that informal caregivers might be targets of dehumanization.
Dehumanization Processes on the Perception of Victims
Dehumanization not only contributes to the suffering of victims (e.g., Viki et al., Reference Viki, Fullerton, Raggett, Tait and Wilthsire2012) but can also follow experiences of suffering or ill-being (e.g., Sakalaki et al., Reference Sakalaki, Richardson and Fousiani2017). Recent studies indicate that groups facing challenging life conditions, such as illnesses (e.g., Fontesse et al., Reference Fontesse, Rimez and Maurage2021), low social status (e.g., Harris & Fiske, Reference Harris and Fiske2006), and lower SES (e.g., Loughnan et al., Reference Loughnan, Haslam, Sutton and Spencer2014; Sainz et al., Reference Sainz, Loughnan, Martínez, Moya and Rodríguez-Bailón2020), are often perceived or treated as less than fully human.
Despite the crucial role of empathy in understanding the feelings of others (Scatolon et al., Reference Scatolon, Sharvit, Huici, Álamo Hernández, Glazer, Lorenzo Sánchez and Michna2023), empathizing with the vulnerability and suffering of others can be inconvenient, stressful, and even dangerous, potentially eliciting a defensive reaction from observers (Fousiani et al., Reference Fousiani, Michaelides and Dimitropoulou2019; Rosenblatt, Reference Rosenblatt and Anderson2017). The dehumanization of victims is considered a functional and adaptive mechanism employed by observers to avoid the personal costs and distress associated with helping or witnessing the suffering of other human beings (e.g., Cameron et al., Reference Cameron, Harris and Payne2016; Trifiletti et al., Reference Trifiletti, Di Bernardo, Falvo and Capozza2014; Vaes & Muratore, Reference Vaes and Muratore2013). For instance, Vaes and Muratore (Reference Vaes and Muratore2013) and Trifiletti et al. (Reference Trifiletti, Di Bernardo, Falvo and Capozza2014) found that healthcare professionals attributing uniquely human traits and emotions to suffering patients experienced more stress and burnout symptoms, especially those with higher direct contact and affective commitment to patients. Moreover, a recent study by Cameron et al. (Reference Cameron, Harris and Payne2016) showed that individuals motivated to avoid emotional exhaustion by helping drug addicts are more likely to dehumanize them.
Perceiving victims as less human is considered crucial for the well-being of observers (e.g., Vaes & Muratore, Reference Vaes and Muratore2013), and for the proper functioning of society as a whole (Bastian et al., Reference Bastian, Jetten, Haslam, Bain, Vaes and Leyens2014). However, this perception worsens the situation in which victims find themselves, as it is associated with reduced helping behavior (e.g., Andrighetto et al., Reference Andrighetto, Baldissarri, Lattanzio, Loughnan and Volpato2014; Cuddy et al., Reference Cuddy, Fiske and Glick2007) and with reduced empathy for victims’ suffering (e.g., Čehajić et al., Reference Čehajić, Brown and González2009; Nagar & Maoz, Reference Nagar and Maoz2017). Indeed, considering others as less than fully human allows individuals to accept, legitimize (Bar-Tal, Reference Bar-Tal2000), or minimize and deny others’ suffering (Čehajić et al., Reference Čehajić, Brown and González2009; Nagar & Maoz, Reference Nagar and Maoz2017).
This defensive dehumanization towards victims is deeply rooted in specific psychological processes, such as the Belief in a Just World (Lerner, Reference Lerner1980), which attempts to explain why observers react negatively toward victims.
Belief in a Just World and Negative Attitudes toward People Suffering
According to the Belief in a Just World theory (BJW; Lerner, Reference Lerner1980), individuals are motivated to perceive the world as a just place where everyone receives what they deserve. This perception of justice gives people confidence that no unjust events will happen to them, despite the injustices in daily life.
However, the existence of innocent victims contradicts this fundamental assumption, thereby threatening people’s BJW. As a result, instead of offering help, observers restore justice cognitively by changing their perceptions of the situation, which may lead to one or more forms of negative attitudes towards the victim, which is frequently named secondary victimization (Brickman et al., Reference Brickman, Rabinowitz, Karuza, Coates, Cohen and Kidder1982). Indeed, aside from dealing with the negative consequences arising from the event that victimized them (primary victimization), victims experience additional victimization from the social reaction of people who know about their situation (secondary victimization). Secondary victimization is a pervasive yet very detrimental phenomenon, given that it exacerbates the adversity faced by victims through various concurrent forms, such as blaming victims for events beyond their control or minimizing and denying the perception of others’ suffering (e.g., Hafer & Bègue, Reference Hafer and Bègue2005).
Most studies exploring individual differences in the BJW have indicated that individuals with higher BJW, when confronted with an innocent victim whose suffering persists, are more likely to engage in secondary victimization than those with lower BJW (e.g., Correia & Vala, Reference Correia and Vala2003). Moreover, recent studies also highlight that sharing an identity with the victim threatens the observers’ BJW and is a predictor of negative reactions towards victims (e.g., Correia et al., Reference Correia, Pereira and Vala2018). Furthermore, research has shown an association between BJW and some ideological variables, such as religiosity and right-wing political orientation (e.g., Dalbert et al., Reference Dalbert, Lipkus, Sallay and Goch2001).
Despite extensive research focused on the impact of observers’ BJW on different forms of secondary victimization, only a few studies have attempted to investigate the dehumanization of victims as a secondary victimization strategy. Indeed, DeVaul-Fetters (Reference DeVaul-Fetters2014) revealed that, across multiple strategies employed to cope with just world threats, the dehumanization of refugees emerged as one of these strategies. Specifically, individuals with a higher BJW dehumanized the refugees more than individuals with a lower BJW. In a related study, Gillmor et al. (Reference Gillmor, Bernstein and Benfield2014) found that victims perceived as being sexually promiscuous were more likely to be dehumanized than those perceived as sexually conservative, especially among observers with higher BJW. The findings of these studies suggest that the dehumanization of victims may serve as a coping mechanism for individuals who feel threatened by the injustices present in the world.
Considering the highly demanding nature of informal caregiving, we believe it has the potential to threaten observers’ sense of justice. Therefore, we propose that participants with higher BJW may be particularly likely to dehumanize informal caregivers and, consequently, minimize the perception of informal caregivers’ suffering.
The Current Research
We conducted two experimental studies to better understand whether and under which conditions informal caregivers are dehumanized. Study 1 aimed to extend the already mentioned studies on the stigmatization of informal caregivers (e.g., Abojabel & Werner, Reference Abojabel and Werner2019; Zwar et al., Reference Zwar, Angermeyer, Matschinger, Riedel-Heller, König and Hajek2020) by investigating whether informal caregivers are targets of dehumanization when compared to individuals who do not perform this role. In Study 2, we further expanded these investigations to examine the moderating impact of participants’ BJW on this process. Furthermore, Study 2 examined the predictive impact of participants’ BJW and the dehumanization of informal caregivers on participants’ perception of informal caregivers’ suffering, while controlling for sociodemographic and individual variables. Lastly, both studies also explored the impact of the targets’ gender on these effects. Based on previous research examining the link between victim dehumanization and perceptions of justice, we measured the attribution of emotions that targets are capable of feeling as an indicator of dehumanization.
Pilot Study
We developed written vignettes where we manipulated the type of target (informal caregiver vs. non-caregiver): The informal caregiver condition presented a fictitious description of the name, age, and daily tasks of an informal caregiver target responsible for caring for a spouse who became paraplegic and suffered a brain injury after a car accident; the non-caregiver condition simply presented a fictitious description of the name and age of a target, along with the information that the target is married. The gender of the target was counterbalanced across experimental conditions with corresponding fictitious names of “Mary” or “Joseph”. We tested the written vignettes with a few participants. Changes were made iteratively in response to feedback on the vignette’s credibility, concision, and clarity.
To increase the perception of the descriptions’ realism, the written vignettes were paired with a picture of either a woman or a man. A pre-test of the pictures was conducted following a procedure applied by Bernardes et al. (Reference Bernardes, Tomé-Pires, Brandão, Campos, Teixeira and Goubert2021). For the pre-test of the female picture, we presented three pictures of three different white women to a sample of 20 participants (50% female; M age = 29.10). Similarly, for the pre-test of the male picture, a separate sample of 22 participants (72.7% female; M age = 36.32) rated four pictures featuring four different white men. Participants were asked about their perceptions of the targets’ age, body weight, educational level, occupation, and socioeconomic status (using the MacArthur Scale of Subjective Social Status; Adler et al., Reference Adler, Epel, Castellazzo and Ickovics2000). Based on the pre-test findings, one picture of a woman and one picture of a man, both perceived as middle-aged, with normal weight, and ambiguous for socioeconomic status, were chosen. See Figure 1 for a detailed description of all vignettes, which constitute the four experimental conditions used in Study 1Footnote 1.
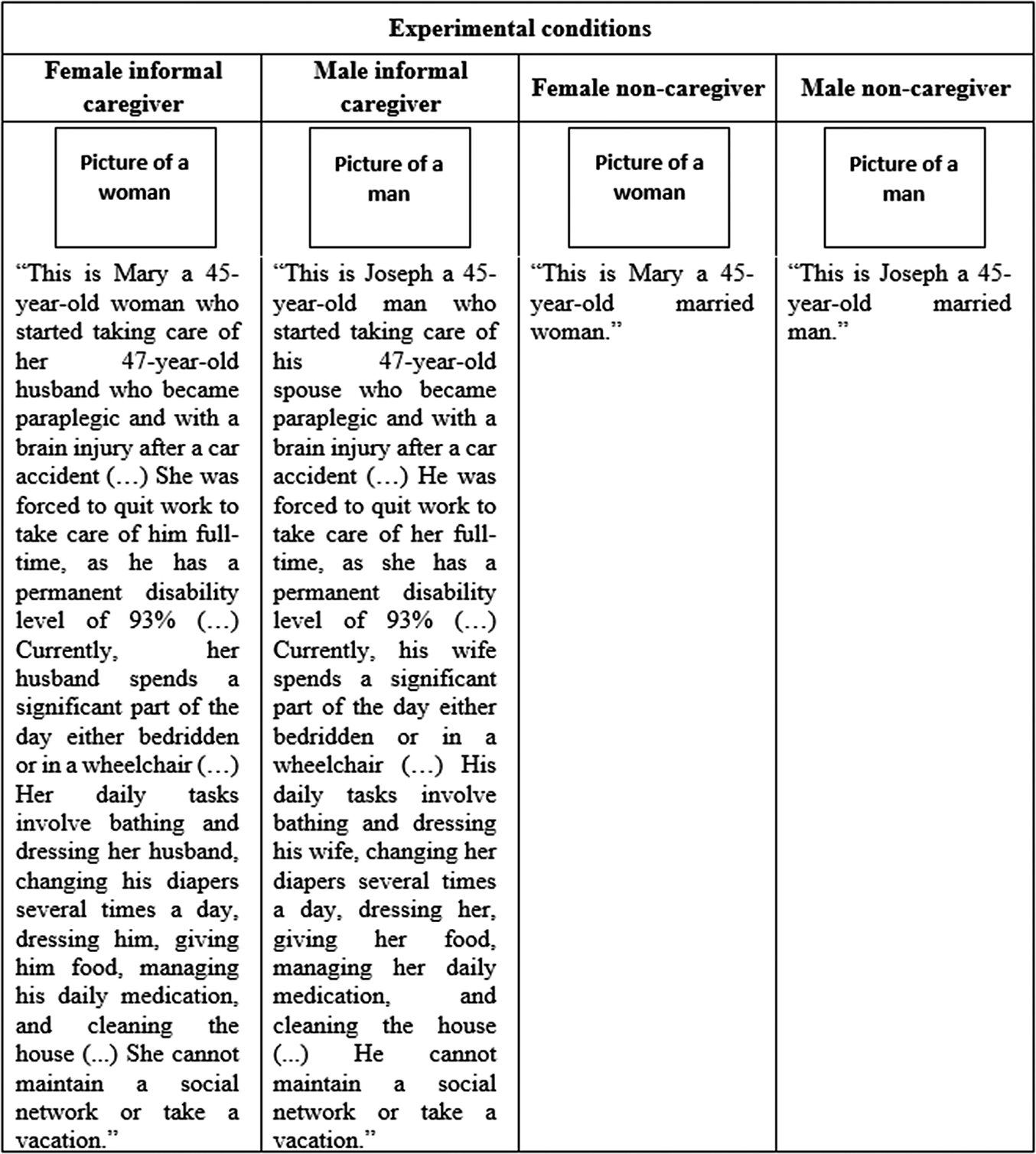
Figure 1. Vignettes describing the Four Experimental Conditions (Study 1).
Study 1
In the present study, we aimed to examine whether informal caregivers are dehumanized by being perceived as experiencing fewer secondary (uniquely human) emotions compared to individuals who do not perform this role. Given that the profile and work environment of informal caregivers (e.g., unpaid work, mainly performed by women, involving the care of disabled individuals), share similar characteristics with dehumanized groups (e.g., Sakalaki et al., Reference Sakalaki, Richardson and Fousiani2017; Volpato et al., Reference Volpato, Andrighetto and Baldissarri2017), we predicted that informal caregivers would be targets of dehumanization. Therefore, we expected participants to attribute fewer secondary (uniquely human) emotions to informal caregivers than to non-caregivers, whereas no differences in the attribution of primary emotions were expected (H 1). We also explored whether the targets’ gender impacts our expected effect; however, we did not advance any priori hypothesis, given the lack of previous supporting evidence.
Method
Participants and Design
The sample comprised 180 participants (66.1% female) aged between 18 and 71 years (M = 32.06, SD = 11.18). Participants were from all regions of Portugal, but mostly resided in the Metropolitan Area of Lisbon (49.4%). Most participants had an undergraduate degree (72.8%) and nearly half were employed (46.1%).
This study used a 2 (Emotion: primary vs. secondary) X 2 (Target type: informal caregiver vs. non-caregiver) X 2 (Target gender: female vs. male) experimental design, with the first factor as within-participants and the two other factors as between-participants.
Procedure
This study was in agreement with the ethics guidelines of the Scientific Commission of the Research Centre where it was conducted and followed the principles outlined in the Declaration of Helsinki. According to the ethics guidelines of the Research Center, formal ethical approval is not required for anonymous surveys that are not compulsory, do not involve sensitive personal information or potentially harmful content, do not use deception, do not require substance ingestion, and do not involve any invasive measures.
Participants were invited to take part in an online survey created on the Qualtrics platform about person perception. Fifty-eight participants completed the study as part of a course requirement, while 122 participants were recruited from the Clickworker website.
After providing informed consent, participants were randomly assigned to one of the four experimental conditions mentioned in the pilot study: Female informal caregiver, male informal caregiver, female non-caregiver, or male non-caregiver (see Figure 1). Participants were informed that the descriptions in the vignettes were real, and to preserve the anonymity of the person, the fictitious names were used. To verify the effect of the experimental manipulation of the target, after reading/seeing the description/picture of the target in the vignette, participants in the informal caregiver’s conditions were asked to recall the target’s age, the spouse’s level of disability, and two daily tasks performed by the informal caregiver target. This task aimed to ensure that participants perceive the informal caregiver target as a middle-aged informal caregiver of a dependent spouse. Participants in the non-caregiver’s conditions were only asked to recall the target’s age.
Following this, participants were asked to complete the dependent measure that assessed their perceptions of the target (dehumanization) and provided demographic information (e.g., age, education, area of the country in which they lived). At the end of the survey, participants were thanked, debriefed about the purpose of the study, and provided with the contact of the main researcher.
Measures
Dehumanization
The dehumanization of the target was measured by asking participants to indicate to what extent they considered the target to experience six different emotions presented in random order. These included three negative primary (fear, sadness, and pain; α = .84) and three negative secondary (bitterness, melancholy, and shame; α = .84) emotions already pre-tested for valence (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004; Martínez et al., Reference Martínez, Rodríguez-Bailón, Moya and Vaes2017). Responses were given on a 6-point scale (from 1 = Not at all to 6 = A lot). Only negative emotions were measured due to the distressing nature of the event, which made it less likely for participants to attribute positive emotions to informal caregivers. This decision was in line with previous studies on adverse situations where only negative emotions were assessed (e.g., Cuddy et al., Reference Cuddy, Fiske and Glick2007; Gillmor et al., Reference Gillmor, Bernstein and Benfield2014).
Analytic Plan
Our Hypothesis 1 was tested in a 2 (Emotion: primary vs. secondary) X 2 (Target type: informal caregiver vs. non-caregiver) X 2 (Target gender: female vs. male) mixed repeated measures ANOVA, controlling for participants’ gender. When differences between conditions were found, pairwise comparisons with Bonferroni correction were examined. The analysis was conducted using IBM SPSS Statistics 28.0.
Results
Manipulation Check
The manipulation check was successful, as all participants in the informal caregiver’s condition correctly described the target’s age, the spouse’s level of disability, and two daily tasks performed by the informal caregiver target; and all the participants in the non-caregiver’s condition were able to correctly describe the target’s age.
Dehumanization of Informal Caregivers
Results showed a main effect of emotion, F(1, 176) = 7.03, p = .009, ηp2 = .04, such that participants attributed more primary (M = 4.10, SD = 1.15) than secondary emotions (M = 3.79, SD = 1.03) to the targets. There was a main effect of the target type, F(1, 176) = 12.04, p < .001, ηp2 = .06, such that participants attributed more emotions to informal caregivers (M = 4.13, SD = 0.80) than to non-caregivers (M = 3.72, SD = 0.87). There was no main effect of target gender, F(1, 176) = 2.04, p = .155, ηp2 = .01.
As expected, there was a two-way interaction between emotion and target type, F(1, 176) = 85.08, p < .001, ηp2 = .33. Pairwise comparisons with Bonferroni correction showed that participants attributed more secondary emotions to non-caregivers (M = 4.02, SD = 0.96) than to informal caregivers (M = 3.59, SD = 1.06), p < .001. In contrast, participants attributed more primary emotions to informal caregivers (M = 4.66, SD = 0.99) than to non-caregivers (M = 3.43, SD = 0.95), p = .006 (see Figure 2).
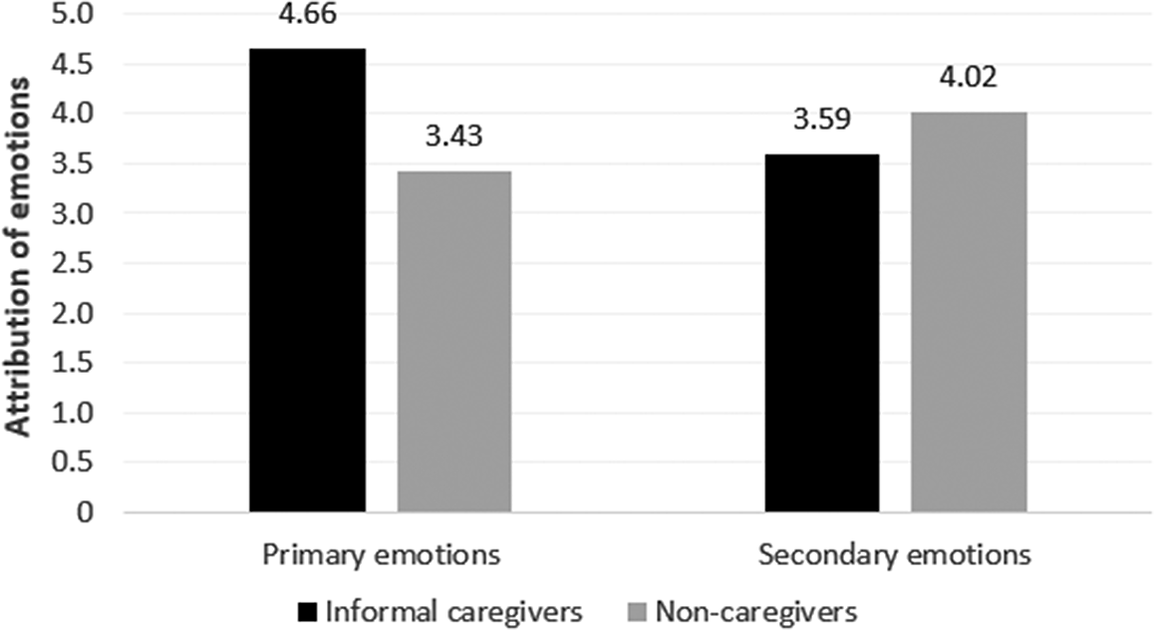
Figure 2. Attribution of Primary and Secondary Emotions according to Type of Target (Informal Caregivers vs. Non-caregivers) (Study 1).
Furthermore, in this same two-way interaction, pairwise comparisons with Bonferroni correction showed that participants attributed more secondary (M = 4.02, SD = 0.96) than primary (M = 3.43, SD = 0.95) emotions to non-caregivers, F(1, 176) = 19.89, p < .001. In contrast, participants attributed more primary (M = 4.66, SD = 0.99) than secondary (M = 3.59, SD = 1.06) emotions to informal caregivers, F(1,176) = 77.13, p < .001.
The two-way interaction between emotion and target gender, F(1, 176) = 1.47, p = .226, ηp2 = .01, and the two-way interaction between target type and target gender, F(1, 176) = 2.16, p = .144, ηp2 = .01, as well as the three-way interaction between emotion, target type, and target gender, F(1, 176) = 0.63, p = .430, ηp2 = .01, were not significant.
Controlling for participants’ gender, the two-way interaction between emotion and target type remained significant, F(1, 175) = 82.87, p < .001, ηp2 = .32; the two-way interaction between emotion and target gender remained non-significant, F(1, 175) = 1.08, p = .300, ηp2 = .01; the two-way interaction between target type and target gender remained non-significant, F(1, 175) = 2.13, p = .147, ηp2 = .01; and the three-way interaction between emotion, target type, and target gender remained non-significant, F(1, 175) = 0.74, p = .392, ηp2 = .01.
Discussion
In this first study, we aimed to empirically examine whether informal caregivers were dehumanized when compared to non-caregivers and to explore the impact of the targets’ gender on this effect.
As expected, our findings suggest that informal caregivers are indeed targets of dehumanization, as they were perceived as experiencing fewer secondary (uniquely human) emotions than non-caregivers, thus supporting our Hypothesis 1. Contrary to the predictions of Leyens et al. (Reference Leyens, Rodriguez-Perez, Rodriguez-Torres, Gaunt, Paladino, Vaes and Demoulin2001) and our prediction that primary emotions would be equally attributed to both groups, participants surprisingly attributed more primary emotions to informal caregivers than to non-caregivers. This may suggest that informal caregivers are not only perceived as less human but also more animal-like, as participants associate them with their animalistic nature, expressed through an over-attribution of primary emotions.
A more detailed examination of the attribution of each emotion separately revealed noteworthy differences. While non-caregivers were attributed with more secondary than primary emotions, informal caregivers were attributed with more primary than secondary emotions. This suggests a distancing of non-caregivers from non-human animals and of informal caregivers from human uniqueness.
Our results also demonstrated that the dehumanization of informal caregivers occurred regardless of their gender: We did not find significant differences between the attribution of primary and secondary emotions to female and male informal caregivers.
This study did not consider potential individual determinants contributing to the dehumanization of informal caregivers. Thus, in Study 2, we aimed to examine the moderating impact of participants’ BJW on the dehumanization of informal caregivers.
Study 2
Extending from our previous study, we aimed to examine the moderating impact of participants’ BJW on the dehumanization of informal caregivers. Based on the findings from Study 1, we expected that informal caregivers would be dehumanized by being attributed fewer secondary emotions (H 1Footnote 2). Framed within the BJW theory (Lerner, Reference Lerner1980), and based on research examining the link between dehumanization and BJW (e.g., DeVaul-Fetters, Reference DeVaul-Fetters2014; Gillmor et al., Reference Gillmor, Bernstein and Benfield2014), we expected that informal caregivers would be dehumanized, especially among participants with higher BJW (H 2).
This study also examined the predictive impact of participants’ BJW and the dehumanization of informal caregivers on the participants’ perception of informal caregivers’ suffering, while controlling for sociodemographic and individual variables. Previous research has indicated that the dehumanization of others (e.g., Čehajić et al., Reference Čehajić, Brown and González2009; Nagar & Maoz, Reference Nagar and Maoz2017) and a higher BJW endorsement (e.g., Hafer & Bègue, Reference Hafer and Bègue2005) are associated with minimizing and denying the perception of others’ suffering. Therefore, we expected that the participants’ perception of informal caregivers’ suffering would be predicted by the participants’ BJW endorsement (H 3) and by the dehumanization of informal caregivers (H 4). Additionally, as in Study 1, we explored whether the targets’ gender impacts our expected effects; however, we did not advance any priori hypothesis, given the lack of previous supporting evidence.
Method
Participants
The sample comprised 205 participants (68.8% female) aged between 18 and 79 years (M = 38.36, SD = 15.02). Participants were from all regions of Portugal, but mostly resided in the Metropolitan Area of Lisbon (71.7%). Most participants had an undergraduate degree (75.6%) and were employed (72.7%). The majority of them reported not being religious at all (61.5%), and not having a political orientation (56.6%). A total of 69.3% of participants reported that, at the time of the study, they were not informal caregivers or had not been informal caregivers in the past. None of these participants completed the previous study.
Procedure
In Study 2 the same ethical procedures of Study 1 were followed. Participants were invited to take part in an investigation introduced as involving two independent studies: (a) A first study about person perception and (b) a second study that aimed to adapt and validate two scales for the Portuguese population. One hundred and twenty-two participants completed the survey online, while 83 participants completed the survey in a paper formatFootnote 3.
After providing informed consent, participants were randomly assigned to one of two experimental conditions: female informal caregiver or male informal caregiver. Specifically, participants read a written vignette with a fictitious description of an informal caregiver target that takes care of a spouse with Alzheimer’s. The gender of the target was counterbalanced, with the alternative wording for each experimental condition highlighted in bold: “ Mary/Joseph a 63-year-old woman/man who started taking care of her/his 67-year-old husband/wife who has Alzheimer’s over more than 5 years (…) She/He was forced to quit work to take care of him/her full-time (…) The doctors estimate that his/her condition may persist for more than 20 years (…) Currently, her/his husband/wife spends a considerable portion of the day bedridden (…) Her/his daily tasks involve bathing and dressing his/her husband/wife , changing his/her diapers several times a day, dressing him/her , giving him/her food, managing his/her daily medication, and cleaning the house (…) She/He cannot maintain a social network or take a vacation.”. Participants were informed that the descriptions in the vignettes were real, and to preserve the anonymity of the person, the fictitious names of “Mary” and “Joseph” were used.
After reading the description of the target in the vignette, participants were asked to complete the dependent measures that assessed their perceptions about the target (dehumanization and suffering) and justice perceptions referring to themselves (BJW). Following this, they provided demographic information (e.g., age, education, area of the country in which they lived, religion), and were asked whether they were or have been informal caregivers. At the end of the survey, participants were thanked, debriefed about the purpose of the study, and provided with the contact of the main researcher.
Measures
Dehumanization
The dehumanization of the target was measured by asking participants to indicate to what extent they considered the target to experience 11 different emotions presented in random order. These included five negative primary (boredom, anguish, terror, tension, and panic; α = .75) and six negative secondary (pity, worry, bitterness, melancholy, resentment, and disconsolation; α = .83) emotions already pre-tested for valence (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004; Martínez et al., Reference Martínez, Rodríguez-Bailón, Moya and Vaes2017). Responses were given on a 5-point scale (from 1 = Much less than the average person to 5 = Much more than the average person). As with Study 1, we only measured negative emotions.
Belief in a Just World
The participants’ BJW was measured with the Portuguese translation of the six-item General Belief in a Just World scale (GBJW) (Dalbert et al., Reference Dalbert, Montada and Schmitt1987) that has been found to be a good predictor of negative reactions towards victims (e.g., Sutton & Douglas, Reference Sutton and Douglas2005). These items assess the extent to which individuals believe that the world, in general, is a just place (e.g., “I think basically the world is a just place”, “I think that, by and large, people get what they deserve”; α = .65). Responses were given on a 5-point scale (from 1 = Totally disagree to 5 = Totally agree). Higher scores reflected higher levels of BJW endorsement.
Perception of Informal Caregivers’ Suffering
The participants’ perception of informal caregivers’ suffering was measured using ten items adapted from Sebastian et al. (Reference Sebastian, Richards and Bilgin2017)Footnote 4. Some of the items have been adapted to the specific context of informal caregivers described in the experimental manipulation (e.g., “The situation in which Mary/Joseph finds herself/himself is pleasant (reversed)”, “Mary’s/Joseph’s present life is a great sacrifice”; α = .79). Responses were given in a 5-point scale (from 1 = Totally disagree to 5 = Totally agree). Higher scores reflected higher levels of participants’ perception of informal caregivers’ suffering.
Control Variables
Besides some relevant participants’ sociodemographic characteristics, we also included participants’ religiosity, empathy, and whether they were or have been informal caregivers as possible controlling variables in the hierarchical regressionFootnote 5. Participants’ religiosity was measured with a single item from the European Social Survey (2018) where participants were asked to rank themselves, regardless of their particular religion, how religious they would say they were. Responses were given on a 5-point scale (from 1 = Not religious at all to 5 = Very religious). Empathy was measured using the Basic Empathy Scale in Adults (BES-A) (Carré et al., Reference Carré, Stefaniak, D’Ambrosio, Bensalah and Besche-Richard2013). We used six items for the disconnection dimension (e.g., “The emotions of my friends don’t affect me much”, α = .78) and eight items for the cognitive dimension (e.g., “I can often understand how people are feeling even before they tell me”, α = .79). Responses were given in a 5-point scale (from 1 = Totally disagree to 5 = Totally agree). To be or have been an informal caregiver was measured with a single item (“Are you or have you ever been an informal caregiver?”), with a (yes/no) answer.
Analytic Plan
Our Hypotheses 1 and 2 were tested in a 2 (Emotion: primary vs. secondary) X 2 (BJW: low vs. highFootnote 6) X 2 (Target gender: female vs. male) mixed repeated measures ANOVA, controlling for whether participants were or have been informal caregivers. When differences between conditions were found, pairwise comparisons with Bonferroni correction were examined. The analysis was conducted using IBM SPSS Statistics 28.0.
For Hypotheses 3 and 4, descriptive statistics (means and standard deviations) were performed to determine the characteristics of the study population and the studied variables. After that, bivariate correlations between all studied variables were conducted. Afterward, a hierarchical regression analysis was conducted to test the predictive impact of participants’ BJW and the attribution of secondary emotions to informal caregivers in participants’ perception of informal caregivers’ suffering. The hierarchical regression analysis included only the variables that significantly correlated with the participants’ perception of informal caregivers’ suffering. The variables were ordered in two blocks: Step 1-socio-demographic and control variables = gender, age, religiosity, cognitive empathy; Step 2-theoretical predictors = BJW, secondary emotions. The analysis was conducted using IBM SPSS Statistics 28.0. A sensitivity power analysis using G*Power (Faul et al., Reference Faul, Erdfelder, Buchner and Lang2009) indicated that we had 80% power to detect an effect size of ηp2 = .05, for Hypotheses 3 and 4.
Results
Dehumanization of Informal Caregivers Moderated by BJW
Results showed a main effect of emotion, F(1, 201) = 33.82, p < .001, ηp2 = .14, such that participants attributed more primary (M = 3.94, SD = 0.62) than secondary emotions (M = 3.69, SD = 0.66) to informal caregivers. There was a main effect of BJW, F(1, 201) = 17.05, p < .001, ηp2 = .08, such that participants with lower BJW attributed more emotions to informal caregivers (M = 3.98, SD = 0.53) than participants with higher BJW (M = 3.67, SD = 0.51). There was no main effect of target gender, F(1, 201) = 0.05, p = .826, ηp2 = .00.
As expected, there was a two-way interaction between emotion and BJW, F(1, 201) = 42.70, p < .001, ηp2 = .18. Pairwise comparisons with Bonferroni correction showed that participants with higher BJW attributed more primary (M = 3.93, SD = 0.66) than secondary emotions (M = 3.41, SD = 0.68) to informal caregivers, p < .001. In contrast, participants with lower BJW did not differently attribute primary (M = 3.96, SD = 0.57) and secondary emotions (M = 3.99, SD = 0.48) to informal caregivers, p = .619 (see Figure 3).
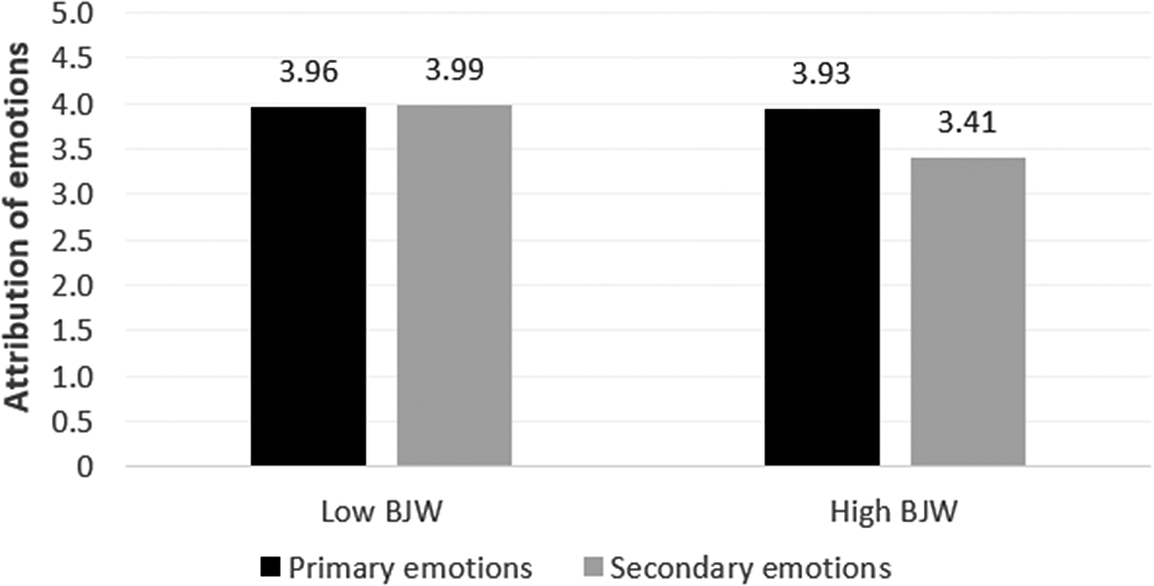
Figure 3. Attribution of Primary and Secondary Emotions According to Participants’ BJW (Low BJW vs. High BJW) (Study 2).
Furthermore, in this same two-way interaction, pairwise comparisons with Bonferroni correction showed that participants with higher BJW attributed fewer secondary emotions (M = 3.41, SD = 0.68) to informal caregivers than participants with lower BJW (M = 3.99, SD = 0.48), F(1, 201) = 48.58, p < .001; whereas there were no differences on the attribution of primary emotions to informal caregivers by participants with higher BJW (M = 3.93, SD = 0.66) and lower BJW (M = 3.96, SD = 0.57), F(1, 201) = 0.11, p = .742.
The two-way interaction between emotion and target gender, F(1, 201) = 0.79, p = .374, ηp2 = .05, and the two-way interaction between target gender and BJW, F(1, 201) = 0.00, p = .981, ηp2 = .00, as well as the three-way interaction between emotion, BJW, and target gender, F(1, 201) = 1.978, p = .161, ηp2 = .01, were not significant.
Controlling whether participants were or have been informal caregivers, the two-way interaction between emotion and BJW remained significant, F(1, 200) = 42.17, p < .001, ηp2 = .17; the two-way interaction between emotion and target gender remained non-significant, F(1, 200) = 0.81, p = .368, ηp2 = .00; the two-way interaction between target gender and BJW remained non-significant, F(1, 200) = 0.00, p = .981, ηp2 = .00; and the three-way interaction between emotion, BJW, and target gender remained non-significant, F(1, 200) = 1.893, p = .170, ηp2 = .01.
The Predictive Role of Participants’ BJW and the Dehumanization of Informal Caregivers in the Participants’ Perception of Informal Caregivers’ Suffering
The descriptive statistics and the pattern of correlations between all the studied variables are presented in Table 1. The perception of informal caregivers’ suffering was significantly and negatively correlated with BJW (r = –.34, p < .001) and religiosity (r = –.20, p = .004); and positively correlated with secondary emotions (r = .41, p < .001) and cognitive empathy (r = .15, p = .036). The BJW was significantly and negatively correlated with secondary emotions (r = –.44, p < .001); and positively correlated with religiosity (r = .14, p = .046). Cognitive empathy was significantly and negatively correlated with emotional disconnection (r = –.42, p < .001). Being a woman was significantly and negatively correlated with being or having been an informal caregiver (r = –.22, p < .001); and positively correlated with religiosity (r = .15, p = .029) and cognitive empathy (r = .14, p = .042). Finally, a significant negative correlation between age and being or having been an informal caregiver was found (r = –.28, p < .001).
Table 1. Descriptive Statistics and Bivariate Correlations between Study Variables (Study 2)
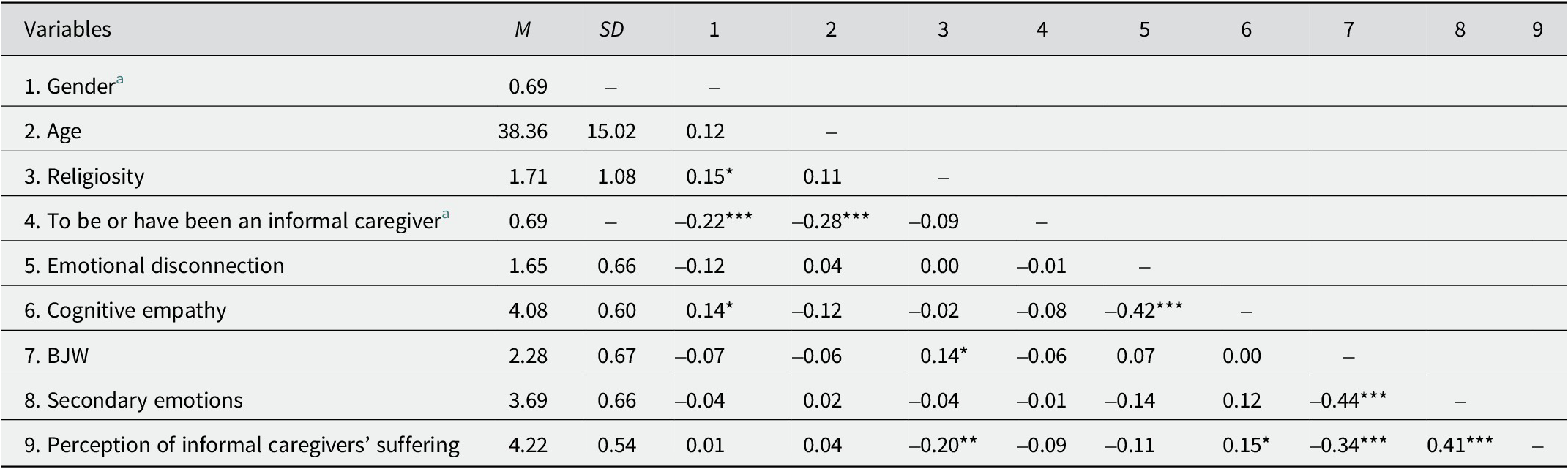
Note. For all measures, scores were computed by averaging across items, with higher scores indicating a higher endorsement of the construct. For gender, 1 indicates “male” and 2 “female”; for to be or have been an informal caregiver, 1 indicates “yes” and 2 “no”. BJW = belief in a just world.
a Dummy variable: It reports the proportion of females, and the proportion of participants that reported were not an informal caregiver at the time of the study or had not been an informal caregiver in the past (respectively).
*p < .05. **p < .01. ***p < .001.
The results of the hierarchical regression analysis are presented in Table 2. The analysis revealed that Model 1 was statistically significant, F(4, 204) = 3.69, p = .006, and that participants’ religiosity (β = –.21, p = .003) and cognitive empathy (β = .15, p = .030) significantly explained 0.7% of the variance in the participants’ perception of informal caregivers’ suffering. Higher participants’ religiosity and fewer participants’ cognitive empathy significantly predicted the participants’ minimization of the perception of informal caregivers’ suffering. In Model 2, the inclusion of participants’ BJW and attribution of secondary emotions to informal caregivers led to a significant improvement in the model, with significant changes in R2 of 18%, F(6, 204) = 10.70, p < .001. Specifically, 25% of the variance in the participants’ perception of informal caregivers’ suffering was predicted by participants’ religiosity (β = –.17, p = .007), participants’ BJW (β = –.18, p = .013), and the attribution of secondary emotions to informal caregivers (β = .32, p < .001). Higher participants’ religiosity, higher participants’ BJW, and a lower attribution of secondary emotions (dehumanization) to informal caregivers significantly predicted the participants’ minimization of the perception of informal caregivers’ suffering.
Table 2. Hierarchical Regression Analysis Predicting the Perception of Informal Caregivers’ Suffering (Study 2)
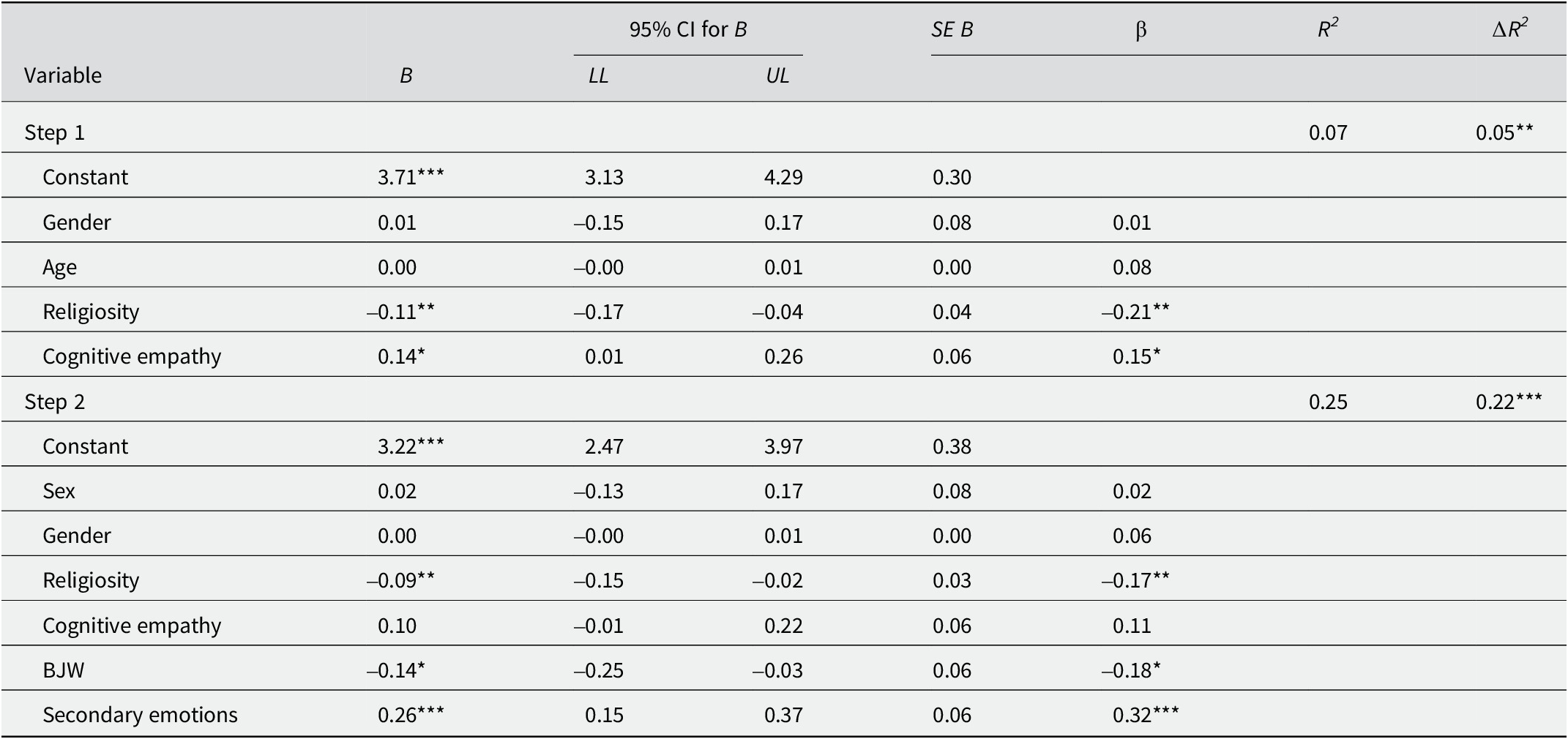
Note. For all measures, scores were computed by averaging across items, with higher scores indicating a stronger endorsement of the construct. For gender, 1 indicates “male” and 2 “female”
Abbreviations: BJW = belief in a just world. B = unstandardized coefficients; β = standardized coefficients; CI = confidence interval; LL = lower limit; UL = upper limit.
*p < .05. **p < .01. ***p < .001.
Mediating Effect of Dehumanization of Informal Caregivers on the Relationship between BJW and the Perception of Informal Caregivers’ Suffering
Given the results consistently found the impact of participants’ BJW and the attribution of secondary emotions to informal caregivers on the participants’ perception of informal caregivers’ suffering, we tested a model of the relationship between these variables. Specifically, to test the possible indirect effect of the participants’ BJW on the participants’ perception of informal caregivers’ suffering through the attribution of fewer secondary emotions (dehumanization) to informal caregivers, we computed a mediation model using PROCESS macro (Model 4; Hayes, Reference Hayes2017) with 5,000 bootstrap samples. Our analysis revealed a significant indirect effect, β = –.11, 95% CI [–0.19, –0.05], which suggests that the participants’ BJW impacts their perception of informal caregivers’ suffering through the attribution of fewer secondary emotions (dehumanization) of informal caregivers (see Figure 4). These results demonstrated that the higher the participants’ BJW and the less they attribute secondary emotions to informal caregivers, the more they minimize the perception of informal caregivers’ suffering. When considering secondary emotions in the path between participants’ BJW to their perception of informal caregivers’ suffering (the indirect effect), the direct path between participants’ BJW to their perception of informal caregivers’ suffering (direct effect) is no longer significant, β = –.16, p = .05, 95% CI [0.01, –0.27], which indicates a mediation effect.
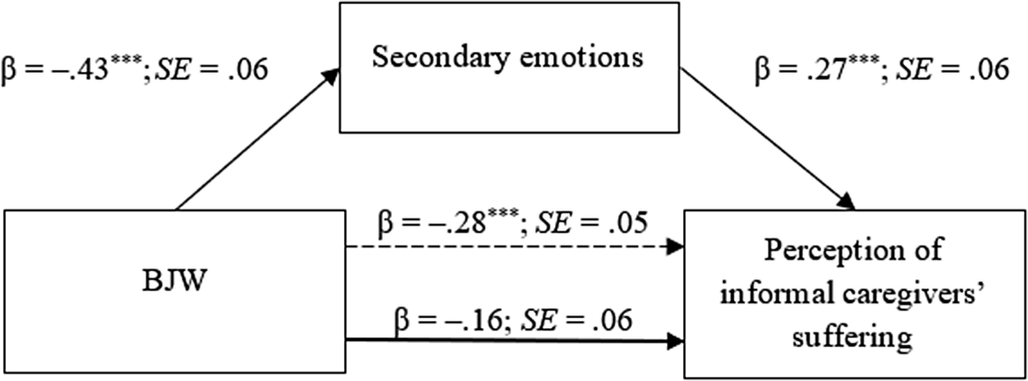
Figure 4. Test of the Indirect Effect of BJW on the Perception of Informal Caregivers’ Suffering through Dehumanization of Informal Caregivers (Study 2).
Note. The dotted line shows coefficient weights for the relationship before mediation by the attribution of secondary emotions to informal caregivers (total effect). β = nonstandardized coefficients; SE = standard error.
***p < .001.
Discussion
This study aimed to build upon the findings of Study 1 by examining the moderating impact of participants’ BJW on the dehumanization of informal caregivers. Additionally, we aimed to examine the predictive impact of participants’ BJW and the dehumanization of informal caregivers on the participants’ perception of informal caregivers’ suffering, while controlling for sociodemographic and individual variables. As in Study 1, we also explored whether the targets’ gender impacts the dehumanization effect.
As expected, our findings replicated the findings of Study 1 by showing that individuals dehumanize informal caregivers, thus supporting our Hypothesis 1. In line with Study 1, our results also provided additional support for the over-attribution of primary emotions to informal caregivers, suggesting that informal caregivers are relegated to a lower and more primitive order of humanity, as primary emotions are more rapidly associated with animals than with humans (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004). Moreover, our results also showed that the dehumanization of informal caregivers occurred regardless of the gender of informal caregivers.
We also extended these findings by showing that the dehumanization of informal caregivers was moderated by participants’ BJW endorsement. Specifically, while participants with lower BJW did not differ on the attribution of primary and secondary emotions to informal caregivers, participants with higher BJW attributed them more primary than secondary emotions, supporting our Hypothesis 2. These findings suggest that individuals with higher BJW are more likely to dehumanize informal caregivers, possibly as a cognitive coping mechanism when confronted with the challenging life conditions faced by informal caregivers, serving as a means to restore their BJW.
Moreover, our findings also revealed the predictive impact of participants’ religiosity, participants’ BJW, and the dehumanization of informal caregivers on the participants’ perception of informal caregivers’ suffering. These findings support our Hypotheses 3 and 4 and suggest that higher participants’ religiosity, higher participants’ BJW, and the lower attribution of secondary emotions (dehumanization) to informal caregivers predicted the participants’ minimization of the perception of informal caregivers’ suffering.
Furthermore, we tested the possible indirect effect of participants’ BJW on the participants’ minimization of the perception of informal caregivers’ suffering through the attribution of fewer secondary emotions (dehumanization) to informal caregivers. Notably, we found that the dehumanization of informal caregivers was an underlying process between participants’ BJW and their minimization of the perception of informal caregivers’ suffering.
General Discussion
Our studies address for the first time the dehumanization of informal caregivers and the conditions in which this phenomenon seems to occur. Results from Study 1 showed that informal were dehumanized, as they were perceived as experiencing fewer secondary emotions compared to non-caregivers. Study 2 while not directly comparing informal caregivers and non-caregivers, still showed a consistent pattern of attributing fewer secondary emotions to informal caregivers. This aligns with prior research on the dehumanization of stigmatized groups facing difficult conditions, like disabled individuals, elderly individuals, women, and low-status occupational groups (e.g., Boudjemadi et al., Reference Boudjemadi, Demoulin and Bastart2017; Fiske et al., Reference Fiske, Cuddy, Glick and Xu2002; Volpato et al., Reference Volpato, Andrighetto and Baldissarri2017), which share similarities with the profile and role of informal caregivers. Indeed, informal care is mostly performed by women who provide care without monetary compensation to dependent elderly or disabled individuals, often dehumanized and facing challenging conditions. Moreover, the caregiving role involves emotional involvement, nurturing, and sensitivity, characteristics often associated with animals. Furthermore, perceiving informal caregivers as less than human may lead to their social devaluation and invisibility in society, despite their crucial contributions. Indeed, dehumanization has the potential to result in reduced opportunities for intergroup engagement (Haslam & Loughnan, Reference Haslam and Loughnan2014), reduced empathy for others’ suffering (e.g., Čehajić et al., Reference Čehajić, Brown and González2009; Nagar & Maoz, Reference Nagar and Maoz2017), reduced prosocial behavior (e.g., Andrighetto et al., Reference Andrighetto, Baldissarri, Lattanzio, Loughnan and Volpato2014; Cuddy et al., Reference Cuddy, Fiske and Glick2007), and reluctance to support for welfare policies (e.g., Sainz et al., Reference Sainz, Loughnan, Martínez, Moya and Rodríguez-Bailón2020).
Surprisingly, in both studies, informal caregivers were attributed with more primary than secondary emotions, suggesting an attempt to differentiate them from the non-caregivers. At this point, only a few studies have identified a similar over-attribution of primary emotions to outgroups (e.g., Leyens et al., Reference Leyens, Rodriguez-Perez, Rodriguez-Torres, Gaunt, Paladino, Vaes and Demoulin2001, Study 1; Rodrigues et al., Reference Rodrigues, Fasoli, Huic and Lopes2018; Rohmann et al., Reference Rohmann, Niedenthal, Brauer, Castano and Leyens2009; Viki & Calitri, Reference Viki and Calitri2008). Because caring is an integral part of women’s identity (e.g., Erreguerena, Reference Erreguerena2015; Esplen, Reference Esplen2009; United Nations Department of Economic and Social Affairs-Population Division, 2019), we could perceive the over-attribution of primary emotions to informal caregivers as a simple reflection of the traditional stereotype by which women are perceived (e.g., emotional, warm, and affectionate). However, the same pattern of results was not found for the female non-caregiver, which suggests that this effect is not driven by the target’s gender but by the characteristics associated with the informal caregiving role. We believe that the over-attribution of primary emotions to informal caregivers and the tendency to associate this group more closely with animals than with humans (Demoulin et al., Reference Demoulin, Leyens, Paladino, Rodriguez-Torres, Rodriguez-Perez and Dovidio2004), may suggest a devaluation of their role and a reduced social status.
In addition to this, both studies contribute to understanding the impact of informal caregivers’ gender on their dehumanization. Specifically, the results reveal no significant difference in the attribution of secondary emotions based on the gender of informal caregivers. This suggests that perceiving informal caregivers as less human is more influenced by their caregiving status than their gender.
Moreover, the results of Study 2 further reveal that individuals’ BJW endorsement plays a role in the dehumanization of informal caregivers. Specifically, participants with higher BJW were more likely to dehumanize informal caregivers as they attributed them more primary than secondary emotions. In contrast, participants with lower BJW showed no difference in the attribution of primary and secondary emotions to informal caregivers. This supports previous research indicating that dehumanization is a strategy employed by those with higher BJW to cope with injustices in the world (e.g., DeVaul-Fetters, Reference DeVaul-Fetters2014; Gillmor et al., Reference Gillmor, Bernstein and Benfield2014). The dehumanization of victims may serve as another form of secondary victimization used by individuals motivated to perceive the world as just. Considering that the highly demanding nature of informal caregiving has the potential to threaten participants’ sense of justice, it is plausible that the dehumanization of victims represents another form of secondary victimization, especially by those individuals more motivated to perceive the world as a just place.
Study 2 also highlights for the first time the relationship between BJW, dehumanization, and the perception of suffering. Indeed, we aimed to test the predictive impact of participants’ BJW and the dehumanization of informal caregivers on the participants’ perception of informal caregivers’ suffering. Moreover, we included individual variables such as participants’ religiosity and participants’ cognitive empathy as control variables in the analysis. Our findings suggest that higher participants’ religiosity, higher participants’ BJW, and the dehumanization of informal caregivers contributed to the participants’ minimization of the perception of informal caregivers’ suffering. This suggests that the dehumanization of informal caregivers may be considered a functional and adaptive mechanism for individuals with higher BJW to cope with the distress linked to witnessing others’ suffering.
Additional analysis indicated that the association between participants’ BJW and the participants’ minimization of the perception of informal caregivers’ suffering was mediated by the dehumanization of informal caregivers. This finding not only adds to previous literature on the association between BJW endorsement and dehumanization in minimizing others’ suffering but also establishes a theoretical connection between these three areas of research. It emphasizes the importance of recognizing and valuing the unique emotional experiences of informal caregivers and the potential harm caused by their dehumanization.
The strengths inherent in our studies are evident through several key aspects. Firstly, in Study 1, we presented vignettes of a paraplegic spouse accompanied by a picture of a woman or a man depending on the experimental condition, while in Study 2, we presented vignettes of a spouse with dementia without accompanying pictures. Even though there was this difference in the experimental manipulations, getting similar results in both studies strengthens the validity of the findings. This suggests that the observed effects are not dependent on specific details of the experimental manipulation or context, but rather represent a robust and generalizable phenomenon.
Another strength is related to the dehumanization measures used. It is reasonable to expect that using both absolute and relative measures to assess the degree of dehumanization of informal caregivers could lead to different results (Dawtry et al., Reference Dawtry, Callan, Harvey and Olson2018). In Study 1 participants assessed the dehumanization of the target without making comparisons to anyone else (absolute measure; from 1 = Not at all to 6 = A lot). In Study 2 participants were asked to assess the dehumanization of the target in comparison to others (relative measure; from 1 = Much less than the average person to 5 = Much more than the average person). Relative measures are less susceptible to the impact of social norms and may provide a more precise understanding of the underlying motivation driving derogatory behavior towards victims compared to absolute measures. However, our investigation produced consistent results across both objective and relative measures of dehumanization.
However, it is important to recognize certain limitations that might have affected the scope and generalizability of our findings. One major limitation is the use of convenience sampling, which may have restricted the representativeness and generalizability of our findings. Moreover, most of our participants were women, who might generally show more empathy and willingness to help others compared to men (MacGeorge et al., Reference MacGeorge, Gillihan, Samter and Clark2003). Additionally, the limited age range of our sample may have limited the generalizability of our conclusions to other age groups, as they may have had less contact with informal caregivers. To improve the external validity of our studies, future research should aim to recruit a more diverse sample in terms of gender and age.
Furthermore, while previous studies examining adverse situations have only assessed dehumanization through negative emotions (e.g., Cuddy et al., Reference Cuddy, Fiske and Glick2007; Gillmor et al., Reference Gillmor, Bernstein and Benfield2014), it is possible that considering positive emotions might yield different results. To disentangle this possibility, future research could build on our findings by investigating the dehumanization of informal caregivers using both positive primary and secondary emotions. Moreover, future studies should extend our results and investigate other forms of dehumanization of informal caregivers using for example other subtle measures of dehumanization (e.g., attribution of uniquely human and human nature personality traits; Haslam, Reference Haslam2006), or an explicit and direct blatant dehumanization measure (e.g., Ascent of Human measure; Kteily et al., Reference Kteily, Bruneau, Waytz and Cotterill2015). Future studies should also seek to understand how these forms of dehumanization might influence not only the perception of informal caregivers’ suffering but also prosocial behavior towards them. Lastly, future studies should examine the self-dehumanization of informal caregivers and should seek to understand the actual implications of such dehumanization for their psychological and physical well-being.
Another limitation relates to the use of self-reported measures for all predictors and outcome variables in the linear regression raises concerns about potentially shared method variance, which could lead to an overestimation of the associations between them.
One final limitation concerns the mediation analysis. Even though the direct effect between participants’ BJW and the participants’ perception of the informal caregivers’ suffering is no longer significant, caution is needed in interpreting the causal relationship between the dependent and mediator variables since the association is correlational in nature (Pirlott & MacKinnon, Reference Pirlott and MacKinnon2016).
To the best of our knowledge, our research is pioneering in examining whether and under which conditions informal caregivers are dehumanized. This investigation contributes to the literature by revealing that informal caregivers are dehumanized, regardless of their gender. Indeed, informal caregivers were attributed fewer secondary emotions compared to non-caregivers. Moreover, this effect was moderated by participants’ BJW endorsement, as participants with higher BJW were more likely to dehumanize informal caregivers. Furthermore, our results showed that the dehumanization of informal caregivers serves as an underlying process in the relationship between participants’ BJW and the minimization of the perception of informal caregivers’ suffering. We hope that these results open a new avenue for the study of informal caregivers because they offer both theoretical and practical insights for addressing the dehumanization processes that take place toward informal caregivers.
Authorship credit
A.R.: Conceptualization; methodology; data curation; formal analysis; writing-original draft; writing-review & editing. I.C.: Conceptualization; methodology; writing-original draft; writing-review & editing.
Data sharing
The datasets presented in this article are not publicly available because the participants of this study did not give the permission for their data to be shared publicly. However, the datasets can be available under request directed to Angela_Romao@iscte-iul.pt.
Funding statement
This research was partially funded by Fundação para a Ciência e Tecnologia (FCT) (Grant number PD/BD/150571/2020) awarded to the first autor, and by Centro de Investigação e Intervenção Social (CIS-Iscte) through funding atributed by FCT, Reference UIDB/03125/2020, https://doi.org/10.54499/UIDB/03125/2020.
Conflicts of interest
None.
Author note
Isabel Correia works for the Centro de Investigação e Intervenção Social (CIS-Iscte).






