


The prevalence of overweight and obesity has increased substantially in Finland, particularly among children, adolescents and young adults(Reference Kautiainen, Rimpelä, Vikat and Virtanen1). According to the International Obesity Taskforce(2), the cause of the obesity epidemic is considered twofold: the abundance of energy-dense foods and drinks, leading to passive over-consumption of energy, and an environment with limited opportunities for physical activity, leading to an almost universal sedentary state.
Worldwide, the consumption of caloric sweeteners has increased markedly over the past years with beverages being a major contributor(Reference Popkin and Nielsen3). In Finland, domestic sales of sweets have risen by 40 % over two decades(4) and the consumption of soft drinks has doubled from 1980 to 2004(5). Although the biggest increase has occurred in the consumption of artificially sweetened soft drinks, the proportion of sugar-sweetened soft drinks is still 70 % of all soft drinks(6).
Research regarding consumption of sweets and obesity is rare, and the results are inconsistent. A longitudinal study of children in the USA(Reference Phillips, Bandini, Naumova, Cyr, Colclough, Dietz and Must7) showed no relationship to weight gain, and in a cross-sectional study of thirty-four (primarily European) countries(Reference Janssen, Katzmarzyk, Boyce, Vereecken, Mulvihill, Roberts, Currie and Pickett8) the frequency of sweets consumption was lower in overweight adolescents. The consumption of sugar-sweetened soft drinks has been in focus for its potential role as a risk factor for overweight and obesity(Reference Phillips, Bandini, Naumova, Cyr, Colclough, Dietz and Must7, Reference Bachman, Baranowski and Nicklas9–Reference Schulze, Manson, Ludwig, Colditz, Stampfer, Willett and Hu13). Longitudinal US studies have reported consumption to be directly associated with obesity in children and adult females(Reference Berkey, Rockett, Field, Gillman and Colditz10, Reference Ludwig, Peterson and Gortmaker12, Reference Schulze, Manson, Ludwig, Colditz, Stampfer, Willett and Hu13). In contrast, a Norwegian study with a substantially longer follow-up from adolescence to adulthood (20 years) reported no association between body weight and consumption of sugar-sweetened soft drinks(Reference Kvaavik, Andersen and Klepp11).
Because body weight is a result of health behaviour over time, the effects of sweets and sugar-sweetened soft drinks during a long period are of interest. To our knowledge, only one study(Reference Kvaavik, Andersen and Klepp11) has investigated the association between childhood sugar-sweetened soft drink consumption and adult overweight, and no studies have investigated the association between childhood consumption of sweets and adult overweight. Thus the aims of the present study were to investigate: (i) the associations of BMI and overweight in adulthood with the consumption of sweets and sugar-sweetened soft drinks in childhood; and (ii) the associations of BMI and overweight in adulthood with the change in consumption of sweets and sugar-sweetened soft drinks between childhood and adulthood.
Experimental methods
Study design
The Cardiovascular Risk in Young Finns Study is a large, longitudinal, multi-centre study on CVD risk factors and their determinants among children, adolescents and young adults in Finland. The protocol has included analogous data collection methods over a 21-year period, including physical and biochemical measurements as well as dietary interviews at the study centres, and self-administered questionnaires on diet, smoking, physical activity and other lifestyle factors, and on participants’ and their families’ sociodemographic status. Anthropometric measurements have included the repeated measurement of participants’ weight and height. A written informed consent was obtained from all participants and the ethical committees of the participating centres approved the study protocol of the project. Details of the methods have been described previously elsewhere(Reference Juonala, Viikari, Hutri-Kähönen, Pietikäinen, Jokinen, Taittonen, Marniemi, Rönnemaa and Raitakari14, Reference Åkerblom, Viikari, Raitakari and Uhari15).
Study population
The baseline study was carried out in 1980, when randomly selected participants from both eastern and western Finland were 3, 6, 9, 12, 15 and 18 years of age (total of 3596 subjects, 83 % of those invited), and the same participants have been followed since. After 21 years, those who had participated in 1980 and still had a permanent address in Finland (n 3456) were invited to the follow-up field study; 2280 participants (66 % of those participating at baseline) participated. Lack of time (33 %), absence from the place of residence at the time of the examination (13 %) and unwillingness to participate (13 %) were cited as the main reasons for non-participation(Reference Raitakari, Juonala and Kähönen16). Dropouts were more often men and younger than those who stayed in the study. Comparing dropouts and follow-up participants using age-adjusted analyses separately among men and women, there were no statistically significant differences in baseline BMI, parents’ education, cardiovascular risk factors including serum lipids and blood pressure(Reference Juonala17) or in the baseline frequency of consumption of sweets and sugar-sweetened soft drinks (data not shown). After excluding participants with incomplete data on weight, height or consumption of sweets and sugar-sweetened soft drinks, 2139 participants were included in the current study.
Assessment of consumption of sweets and sugar-sweetened soft drinks
Both at baseline in 1980 and at the follow-up in 2001, the participants were given a self-administered questionnaire on habitual dietary choices when visiting the research centre and asked to return it by mail when completed. In 1980, a parent or guardian filled in the form for children belonging to the two youngest age cohorts (3 and 6 years). Although the questionnaires were not totally identical in 1980 and in 2001 (consisting of nineteen and twenty-one questions, respectively) they both included identical questions on the consumption of sweets and sugar-sweetened soft drinks, with six frequency categories from ‘daily’ to ‘never’. On the basis of these answers, we calculated a variable representing the number of units consumed per month separately for sweets and sugar-sweetened soft drinks. For example, the frequency category ‘daily’ was transformed to 30 units per month, ‘once a week’ to 4 units per month and the frequency category ‘never’ to 0 units per month. Furthermore, we divided the participants into three age- and sex-specific groups based on the change in the number of units consumed and describing the change in their position relative to other participants: ‘increase’ indicating moving upwards in the groups, ‘decrease’ indicating moving downwards and ‘no change’ indicating remaining in the same group after 21 years. The ‘no change’ group was furthermore divided into ‘stable low’ and ‘stable high’ groups. Stable low indicates being in the lowest and the middle group and stable high being in the highest group.
In addition, we combined the two highest (‘daily’ or ‘nearly’ daily), two middle (‘2–3 times a week’ and ‘once a week’) and the two lowest (‘rarely or never’ and ‘2–3 times a month’) frequency categories. The validity of the questionnaire has been reported elsewhere(Reference Mikkilä, Räsänen, Raitakari, Pietinen and Viikari18); significant correlation was found between information obtained by a 48 h dietary recall and by the questionnaire measuring longer-term food choices.
Assessment of weight status
Weight (to the nearest 0·1 kg) and height (to the nearest 0·1 cm) were measured by a trained nurse. BMI was calculated as the participant’s weight in kilograms divided by the square of their height in metres (kg/m2). For participants aged 18 years and older, overweight and obesity were defined as BMI ≥ 25 kg/m2 and BMI ≥ 30 kg/m2, respectively(19). The sex- and age-defined BMI cut-off points suggested by Cole et al.(Reference Cole, Bellizzi, Flegal and Dietz20) were used for children and adolescents aged 3–15 years.
Assessment of other variables
Information on education, physical activity and smoking was assessed with self-administered questionnaires in 1980 and 2001. We used the length of parents’ education as an indicator of the socio-economic status of the family in childhood. Information on the parent with more years of education was included in the analyses. In adulthood, we assessed the participant’s own years of education. Level of education, based on the schooling system in Finland, was defined by using 9 and 12 years of schooling as cut-off points. Physical activity in adulthood was categorized using the frequency of rigorous exercise (minimum duration of 30 min) into three categories: less than weekly, weekly and more than weekly. According to smoking status in adulthood, participants were classified into three groups: regular smokers, ex-smokers and never smokers.
Statistical analyses
We conducted a multivariable, linear regression analysis to examine the independent associations between consumption of sweets and sugar-sweetened soft drinks and adulthood BMI. Adult BMI (in 2001) was inserted into the models as the outcome, and separate models with the consumption of sweets and sugar-sweetened soft drinks (as units per month) or the change in consumption as the predictor variable were conducted. The first models were adjusted for age and overweight status in childhood. Model 2 was additionally controlled for either parental education (childhood predictors) or participant’s own education (change in consumption as the predictor), and model 3 for smoking and physical activity in adulthood. Associations with a P value of less than 0·05 were considered statistically significant.
We also carried out logistic regression analyses to study the risk of being overweight in adulthood according to the frequency of sweets and sugar-sweetened soft drinks consumption in childhood or the change in this consumption from childhood to adulthood. Adjustments were carried out as in linear regression analyses. Odds ratios with a 95 % confidence interval excluding 1 were defined as statistically significant. All statistical analyses were carried out using the SAS for Windows statistical software package versions 8·2 and 9·1 (SAS Institute Inc., Cary, NC, USA).
Results
BMI, overweight and obesity
In childhood and adolescence (in 1980), 7·8 % of both boys and girls were overweight (Table 1). In the youngest age group (3–6 years), the prevalence of overweight was higher in girls than in boys (8·8 % v. 5·2 %), whereas in the oldest group (15–18 years), the prevalence of overweight was higher in boys than in girls (8·7 % v. 4·6 %). In adulthood (in 2001, aged 24–39), 52·0 % of men and 36·2 % of women were overweight (BMI ≥ 25 kg/m2), and 13·3 % of men and 11·0 % of women were obese (BMI ≥ 30 kg/m2). The mean BMI in adulthood was 25·7 kg/m2 for men and 24·5 kg/m2 for women. The prevalence of overweight by age varied in men from 39·7 % in the youngest age group (24–27 years) to 58·8 % in the oldest age group (36–39 years) and in women from 31·5 % in the youngest group (24–27 years) to 38·7 % in the middle age group (30–33 years), and that of obesity in men from 7·4 % (24–27 years) to 19·1 % (36–39 years) and in women from 8·4 % (24–27 years) to 13·7 % (30–33 years).
Table 1 Characteristics of study participants at childhood (in 1980) and adulthood (in 2001): Cardiovascular Risk in Young Finns Study
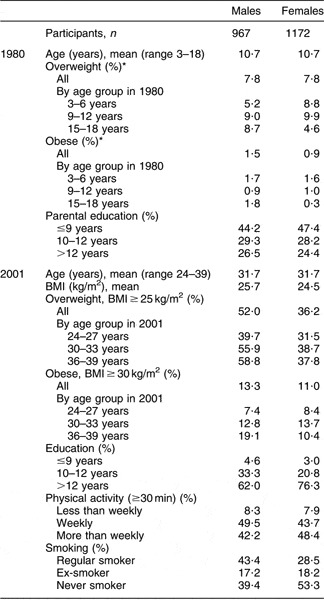
*Defined by Cole et al.Reference Cole, Bellizzi, Flegal and Dietz(20).
Consumption frequency of sweets and sugar-sweetened soft drinks
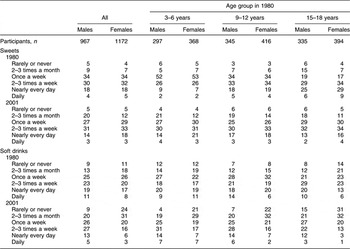
The frequency of consumption of sweets and sugar-sweetened soft drinks between childhood and adulthood is presented in Table 2. In childhood, a bigger proportion of the two oldest groups consumed sweets daily or nearly every day than of the youngest group. However, almost 90 % of the youngest group consumed sweets at least once a week. In adulthood, women were more often daily or nearly every day consumers of sweets than men. The trend was similar in all groups in adulthood. In childhood, more than 70 % of boys from all age groups and of 9- to 12-year-old girls consumed sugar-sweetened soft drinks at least once a week. In adulthood, 45 % of women and 71 % of men consumed sugar-sweetened soft drinks at least once a week.
Table 2 Distribution (%) of frequency of consumption of sweets and sugar-sweetened soft drinks in study participants by gender and by age group: Cardiovascular Risk in Young Finns Study
Sweets and sugar-sweetened soft drinks and BMI
The association between the consumption of sweets and sugar-sweetened soft drinks in childhood and adulthood BMI is shown in Table 3. The consumption of sweets or sugar-sweetened soft drinks in childhood was not significantly associated with BMI in adulthood after adjusting for age and overweight status in childhood and education, smoking and physical activity in adulthood. The change in consumption of sugar-sweetened soft drinks between childhood and adulthood was significantly associated with BMI in adulthood in women but not in men. After adjusting for age and overweight status in childhood (in 1980) and for education, smoking and physical activity in adulthood (in 2001), the estimated BMI was 0·45 kg/m2 (b = 0·45, P = 0·0001) higher for every 10-unit increase in the consumption of sugar-sweetened soft drinks per month in women. The change in consumption of sweets was not associated with adulthood BMI in either men or women.
Table 3 Predicted difference in adult BMI per 10-unit consumption difference for sweets and sugar-sweetened soft drinks and in change in consumption frequency: Cardiovascular Risk in Young Finns Study
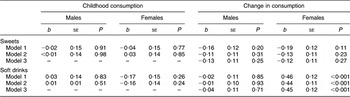
Model 1: adjusted for age in childhood.
Model 2 (childhood consumption): adjusted for age, overweight status and parental education in childhood.
Model 2 (change in consumption): adjusted for age and overweight status in childhood and education in adulthood.
Model 3 (change in consumption): adjusted for age and overweight status in childhood and education, smoking and physical activity in adulthood.
Sweets and sugar-sweetened soft drinks and overweight
No statistically significant association was found between overweight (BMI ≥ 25 kg/m2) in adulthood and the frequency of consumption of sweets and sugar-sweetened soft drinks in childhood using logistic regression analysis (data not shown). The change in the consumption of sweets and sugar-sweetened soft drinks was also assessed with logistic regression analysis (Table 4). In women, an increase (OR = 1·90, 95 % CI 1·38, 2·61) in the consumption of sugar-sweetened soft drinks from childhood to adulthood was associated with being overweight in adulthood. In men, no association was found. Furthermore, after adjusting for age and overweight status in childhood and education, smoking and physical activity in adulthood, the change in consumption of sweets was not associated with being overweight in adulthood. In addition, we compared the risk of being overweight in adulthood between combined frequency categories (daily and nearly daily; 1–3 times a week and less frequently) of sweets and sugar-sweetened soft drinks both in childhood and adulthood (data not shown). No association was found between overweight in adulthood and the frequency of consumption of sweets and sugar-sweetened soft drinks in childhood. In adult women, sugar-sweetened soft drinks frequency categories from daily to 2–3 times a week were associated with being overweight in adulthood (daily and nearly daily: OR = 2·02, 95 % CI 1·27, 3·23; 1–3 times a week: OR = 2·00, 95 % CI 1·51, 2·63) and less frequently: OR = 1·00. In adult men, no association was found.
Table 4 Association of overweight (BMI ≥ 25 kg/m2) in adulthood with change in the frequency of consumption (from childhood to adulthood) of sweets and sugar-sweetened soft drinks: Cardiovascular Risk in Young Finns Study
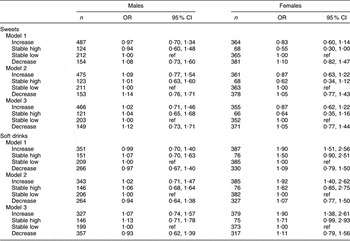
ref, referent category.
Model 1: adjusted for age in childhood.
Model 2: adjusted for age and overweight status in childhood and education in adulthood.
Model 3: adjusted for age and overweight status in childhood and education, smoking and physical activity in adulthood.
Discussion
To our knowledge, the present study is one of the first to investigate the association between childhood consumption of sweets and sugar-sweetened soft drinks and adulthood overweight. Measured as the frequency of consumption, no association was found. However, adulthood BMI and overweight were directly associated with an increase in the consumption of sugar-sweetened soft drinks from childhood and adulthood in women.
Some previous longitudinal studies have observed a direct association(Reference Berkey, Rockett, Field, Gillman and Colditz10, Reference Ludwig, Peterson and Gortmaker12, Reference Schulze, Manson, Ludwig, Colditz, Stampfer, Willett and Hu13) between overweight and sugar-sweetened soft drinks consumption. In studies from the USA, the consumption of sugar-sweetened soft drinks was directly associated with obesity and weight gain in a 19-month follow-up among children aged 11 and 12 years(Reference Ludwig, Peterson and Gortmaker12), in a 2-year follow-up among children aged 9–14 years(Reference Berkey, Rockett, Field, Gillman and Colditz10) and in an 8-year follow-up among adult females(Reference Schulze, Manson, Ludwig, Colditz, Stampfer, Willett and Hu13). The results from a Norwegian study with a follow-up almost as long as in our study are consistent with our findings, observing no association between sugar-sweetened soft drinks consumption and overweight among adolescents followed from 15 to 33 years of age(Reference Kvaavik, Andersen and Klepp11). In our study the association between the change in consumption frequency and overweight was stronger than the association between childhood consumption frequency and overweight. Effectively, the analysis of overweight and the change in frequency can be considered a cross-sectional one, which may at least partly explain the difference in the strength of the associations. However, as the increased risk was observed specifically among those with an increase in the consumption frequency, regardless of the original level, these results indicate the usefulness of the long-term design over cross-sectional.
Dietary habits
One explanation for our result is that although body weight is a consequence of health behaviour over time, dietary habits seem to affect body weight and BMI fairly immediately, and therefore a 21-year period may be too long a time to detect any association between dietary habits and body weight. Studies investigating whether dietary habits change or remain similar from childhood to adulthood have given inconclusive results, possibly due to cultural and methodological differences(Reference Mikkilä, Räsänen, Raitakari, Pietinen and Viikari18, Reference Bertheke Post, de Vente, Kemper and Twisk21–Reference Kelder, Perry, Klepp and Lytle24). Childhood diet has been shown to be a significant determinant of diet in adulthood in the present study cohort(Reference Mikkilä, Räsänen, Raitakari, Pietinen and Viikari18, Reference Mikkilä, Räsänen, Raitakari, Pietinen and Viikari25). Thus, it is reasonable to expect that dietary habits in childhood and adolescence may play a role in adulthood obesity. Other foods, dietary variables or habits may influence body weight or the consumption frequency of sweets and sugar-sweetened soft drinks. However, there is evidence that the association of sugar-sweetened beverages and weight is independent of the influence of other foods(Reference Bes-Rastrollo, Sanchez-Villegas, Gomez-Gracia, Martinez, Pajares and Martinez-Gonzalez26) and therefore we did not control for other dietary variables or dietary habits in the current study.
Portion size
Portion sizes of many foods, such as sweets, soft drinks, fast food and bread, have increased in the last few decades in both the USA(Reference Young and Nestle27) and Europe(Reference Matthiessen, Fagt, Biltoft-Jensen, Beck and Ovesen28). Portion sizes of sweets and soft drinks have also been on the rise in Finland (S Heiskanen, Director, Finnish Food and Drinks Industries Federation, personal communication, April 2006). For soft drinks, the most popular portion size sold is 1·5 litres, replacing the previous portion size of 1 litre. For sweets, not only bigger package sizes but also increased sales of separately sold sweets that are consumer-selected have increased the consumed portions of sweets. The increase in the prevalence of obesity has occurred in parallel with increased portion sizes, which suggests that large portion sizes may play a role in the obesity epidemic(Reference Ledikwe, Ello-Martin and Rolls29). This suggestion has been presented and considered with caution since it is difficult to establish a causal relationship between portion sizes and obesity(Reference Ello-Martin, Ledikwe and Rolls30). Nevertheless, previous data indicate that portion size does indeed influence energy intake(Reference Ello-Martin, Ledikwe and Rolls30). In our study, the consumption of sweets and sugar-sweetened soft drinks was assessed with a short FFQ without any information on portion sizes. It can be assumed, however, that at baseline the portion sizes of sweets and soft drinks were on average smaller than today, and therefore, with present portion sizes and consumption, the results of our study might be different.
Liquid v. solid carbohydrate
We found in women direct associations between increase in the consumption frequency of sugar-sweetened soft drinks and BMI and overweight in adulthood. The consumption or the change in consumption of sweets, by contrast, was not associated with BMI or being overweight. One explanation for this result could be related to the type of carbohydrates in these foods. Evidence that liquids have less impact on satiety than solid foods is inconclusive(Reference Almiron-Roig, Chen and Drewnowski31) when only the form (liquid v. solid) is investigated, regardless of the nutrient or energy content. When investigating the type of carbohydrate, the effect on energy compensation or satiety seems to be different(Reference DiMeglio and Mattes32). In a 4-week study, solid carbohydrates (as jellybean sweets) were compensated in total energy intake, whereas liquid carbohydrates (as soft drinks) were not compensated but rather added to the total energy intake, resulting in a positive energy balance and a significant increase in BMI. DiMeglio and Mattes(Reference DiMeglio and Mattes32) suggested that the act of masticating the solid carbohydrate may provide an internal satiety signal not triggered by swallowing a liquid carbohydrate.
Gender differences
In our study, the increase in sugar-sweetened soft drink consumption was associated with overweight only in women, not in men. This may be due to gender differences in consumption. In our study, boys and men consumed sugar-sweetened soft drinks more often than girls and women. Consumption of sugar-sweetened soft drinks could be a better marker of unhealthy eating behaviour in women than in men. It is possible that women who frequently consume sugar-sweetened soft drinks more often have unhealthy eating behaviour than women who infrequently consume sugar-sweetened soft drinks.
Strengths and limitations
Data for the present study were derived from the Cardiovascular Risk in Young Finns Study, where the same participants were followed for 21 years. The main strength of this study is the longitudinal study design, which allows us to investigate the diet and BMI of the same participants as children and as adults. Instead of self-reports, body height and weight were measured, and thus no self-report bias in BMI or in the prevalence of overweight and obesity exists. In the regression models we controlled for physical activity level as suggested in reviews by Malik et al.(Reference Malik, Schulze and Hu33) and Bachman et al.(Reference Bachman, Baranowski and Nicklas9).
Since the present study was observational, we cannot establish causal relationships from the results. The method of assessment of sweets and sugar-sweetened soft drinks consumption describes the frequency of consumption, and not the absolute amounts consumed. Furthermore, we cannot exclude under-reporting, which is a common error in self-reports of food intake(Reference Hill and Davies34–Reference Johansson, Wikman, Ahren, Hallmans and Johansson36). Foods considered unhealthy or fattening(Reference Lafay, Mennen, Basdevant, Charles, Borys, Eschwege and Romon37, Reference Scagliusi, Polacow, Artioli, Benatti and Lancha38) or high in carbohydrates(Reference Poppitt, Swann, Black and Prentice39) are under-reported more frequently. BMI also affects self-reports of food intake, with people with high adiposity tending to under-report more often(Reference Hill and Davies34–Reference Johansson, Wikman, Ahren, Hallmans and Johansson36, Reference Bedard, Shatenstein and Nadon40). Under-reporting may partly explain why we did not find any association between sweets and soft drinks consumption and overweight. Since we did not assess the amount or the portion sizes of sweets and soft drinks consumed, it is possible that the overweight participants actually consumed sweets and soft drinks less often than their normal-weight peers, but ate or drank larger portions, thus consuming comparable or even greater amounts of sweets or soft drinks. Furthermore, a possible confounder could be artificially sweetened soft drinks since these drinks might have been preferred by participants who tried to lose weight. Artificially sweetened beverages were not included in the frequency questionnaire of our study.
Conclusions
In conclusion, we found in women direct associations between both adulthood BMI and overweight and increasing sugar-sweetened soft drinks consumption from childhood or adolescence. Although our study did not find any association between overweight and childhood consumption of sweets and sugar-sweetened soft drinks, we emphasize that sweets and sugar-sweetened soft drinks are important when considering weight management or body weight. Obesity is not merely a consequence of eating too much of just one or two foods (e.g. sweets or soft drinks), but rather an overall imbalance of the diet and other lifestyle factors. Body weight is an outcome of balance between energy intake and energy expenditure, and especially if sugar-sweetened soft drinks are not compensated in the total energy intake, the balance can become positive, resulting in weight gain. Furthermore, consumption of sweets and sugar-sweetened soft drinks may be a marker of unhealthy lifestyle or unrecognized factors that affect body weight. There is evidence, supported by our results as well, that sugar-sweetened soft drinks are associated with weight gain and obesity. With parallel increases in the prevalence of obesity and the consumption of sweets and sugar-sweetened soft drinks, more research is needed to clarify the association between obesity and diet in general, including the consumption of sweets and sugar-sweetened soft drinks. As obesity is such a widespread problem among young adults – in our study, 52 % of men and 36 % of women were at least overweight – identification of underlying causes of obesity in young adults is essential.
Acknowledgements
Sources of funding: This study was financially supported by the Academy of Finland (grant no. 77841 and 210283), the Finnish Cultural Foundation, the Juho Vainio Foundation and the Yrjö Jahnsson Foundation. Conflict of interest declaration: None declared. Authorship responsibilities: K.N., V.M., S.M., M.L.-K. and L.R. designed the study and the statistical analyses and models. K.N. and V.M. drafted the initial manuscript. K.N. drafted the final manuscript. V.M. ran the statistical analyses. L.R. is responsible for the nutritional field studies of the project. O.T.R. and J.V. are responsible for the project. All authors contributed to the interpretation of the data, revised the manuscript critically and approved the final version of the manuscript.




