


The XXX Summer Olympiad and XIV Summer Paralympic Games will run for a 9-week period from 27 July to 9 September 2012. Several million visitors, 15 000 athletes and 14 000 officials will attend from over 200 countries. 1,2 Increased demand on health services in the six host boroughs in north east London has been projected to be 5.07% during the Olympics and 3% during the Paralympic Games. 3 Across London each National Health Service (NHS) trust has been requested to provide assurances to NHS London and the Department of Health regarding preparation for the Games. A comprehensive review of public health systems employed in previous games describes the surveillance systems that were implemented. Reference Enock and Jacobs4 These systems became more robust from the 1990s onwards. However, this review did not describe data collected from surveillance and no reference was made to mental health. Although no specific projections for mental health service usage have been made, the potential for London 2012 to attract people with a mental illness has been acknowledged. 5 Similarly, the potential for fixated persons to travel has also been noted. In light of the uncertainty over potential mental health demand, we aimed to review data from previous Summer Olympics on general health service and mental health service demand specifically.
Method
We limited our search to the previous ten Summer Olympic and Paralympic Games. Papers relating to other mass gatherings were not sought as there is no comparable event matching the size, duration and concentration of visitors attending the Summer Olympics. Differences in the demographics of those attending other mass gatherings are likely, which could decrease the validity of any comparison.
An electronic search of MEDLINE, EMBASE, CINAHL, PsycINFO and Health Business Elite databases was conducted. The following terms were linked by the Boolean operator ‘OR’: olympic games, paralympics games, olympi*, Beijing Olympic games, Beijing Olympic games 2008, Beijing olympi* (with key words repeated for each host city Athens, Sydney, Atlanta, Barcelona, Seoul, Los Angeles, Moscow, Montreal and Munich as described for Beijing) and combined with the following terms by ‘AND’: public health, mental health, disease distribution, psychiatric disorder, psychiatry, psych*, which were linked by ‘OR’. The search was limited to humans and years 1970-2012.
Titles and abstracts were screened by one author (D.D.) to identify English-language papers reporting disease surveillance or health service usage during Summer Olympic and Paralympic Games from the Munich 1972 Olympics onwards. Articles that did not report data or illness trends were not included. Papers retrieved from the initial screen were reviewed by two authors (D.D. and M.K.). Agreement was reached over the inclusion of the papers without the need to refer to a third author. A bibliographic search of all retrieved articles and NHS London policy documents was also conducted.
Results
Our initial search returned 614 papers, with 8 papers identified as relevant. The summary of the selection of papers is described in Fig. 1. The eight retrieved papers related to five of the previous ten Olympics (Table 1). Reference Liang, Lan, Chen, Zhang, Lü and Lü6-Reference Indig, Thackway, Jorm, Salmon and Owen13 No relevant papers for the Barcelona, Seoul, Moscow, Montreal and the Munich Olympics were identified.
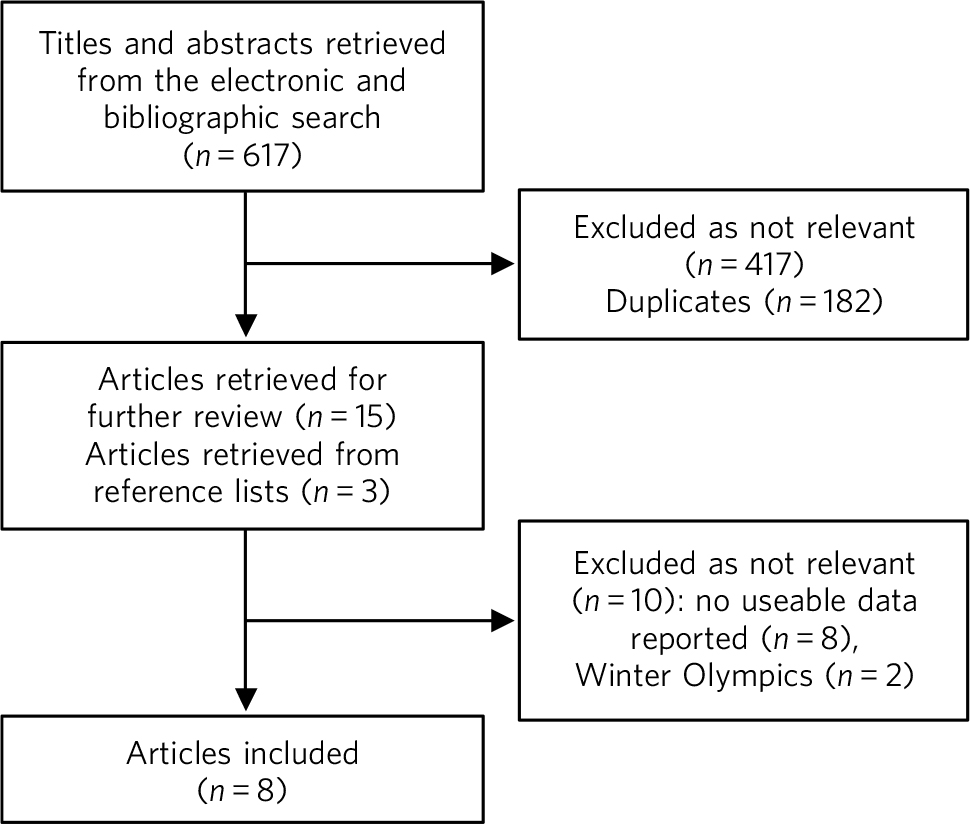
FIG. 1 Summary of the selection of papers.
TABLE 1 Summary of evidence
| Games, author and year | Recorded cases of all health conditions, total n |
Change in general health service demand |
Mental health demand, n |
|---|---|---|---|
| Beijing 2008 | |||
| Liang et al (2011)Reference Liang, Lan, Chen, Zhang, Lü and Lü 6 | Olympic period: 22 029 Paralympic period: 8046 |
Change in demand not stated |
Neuropsychiatric presentations Olympics: 878 Paralympics: 85 |
| Dapeng et al (2010)Reference Dapeng, Ljungqvist and Troedsson 7 | Olympic hospitals: 3567 Other hospitals: 314 Admissions: 128 Polyclinic: 22 137 |
Comparable with the equivalent 2007 period |
Presentations at the polyclinic: 33 No presentations at Olympic designated hospitals |
| Athens 2004 | |||
| Tsouros & Efstathiou (2007)Reference Tsouros and Efstathiou 8 |
Olympic period: 10 564 Paralympic period: 3546 |
No change (communicable disease) |
Olympics: 16 Paralympics: <10 |
| Sydney 2000 | |||
| Jorm et al (2003)Reference Jorm, Thackway, Churches and Hills 9 | Emergency department presentations over 38 days (Olympic period and 3 weeks prior): 55 339 Overseas visitors: 1431 |
5% increase | No reference to mental health |
| Indig et al (2003)Reference Indig, Thackway, Jorm, Salmon and Owen 13 | Illicit drug use presentations over 38 days (Olympic period and 3 weeks prior): 424 |
Illicit drug use increased by over 50% compared with the corresponding period |
No reference to mental health comorbidity |
| Atlanta 1996 | |||
| Wetterhall et al (1998)Reference Wetterhall, Coulombier, Herndon, Stephanie and Cantwell 10 | Encounters over the 30-day monitoring period: 44 142 |
Comparable with previous years |
No recorded mental health admissions |
| Los Angeles 1984 | |||
| Weiss et al (1988)Reference Weiss, Mascola and Fannin 11 | Not stated | Decreased | No reference to mental health |
| Baker et al (1986)Reference Baker, Simone, Niemann and Daly 12 | Cases at 9 event sites: 5516 Cases of drug or alcohol ingestion: 8 |
Not stated | No recorded mental health admissions |
Data reported by all papers originated from centralised health surveillance systems in place during the Olympics period. Health service provision was coordinated by the respective games organising committees with a similar model of health service provision adopted; this included Olympic village polyclinics, medical or first aid stations and Olympic designated sentinel hospitals. The system of data collection was broadly the same, with healthcare professionals required to complete a medical encounter form detailing the nature of the presentation, either in paper or electronic form, which was then collated centrally.
General health service utilisation was reported in detail for the Beijing, Athens, Sydney, Atlanta and Los Angeles Olympics. Reference Liang, Lan, Chen, Zhang, Lü and Lü6-Reference Baker, Simone, Niemann and Daly12 Specific reference to mental health demand was only made in relation to the Beijing and Athens Olympics. Reference Dapeng, Ljungqvist and Troedsson7,Reference Tsouros and Efstathiou8 A single paper detailing drug and alcohol demand was also retrieved. Reference Indig, Thackway, Jorm, Salmon and Owen13
A large number of neuropsychiatric presentations were recorded during Beijing 2008, however the nature or severity of these presentations was not specified. Reference Liang, Lan, Chen, Zhang, Lü and Lü6 An earlier World Health Organization paper did not report any mental health presentations to Olympic designated hospitals, but did report 33 psychiatric encounters at the Olympic village polyclinic, comprising 0.1% of presentations. Reference Dapeng, Ljungqvist and Troedsson7 This suggests the neuropsychiatric presentations were either primarily neurological, less severe psychiatric disorders or both. Athens reported a similarly small number of mental health consultations, consisting of 0.2% of all presentations. Reference Tsouros and Efstathiou8
Sydney was the only host city to experience an increased demand for general health services, which itself was a modest 5% higher compared with the preceding year. Reference Jorm, Thackway, Churches and Hills9 An increase in presentations due to illicit drug use was also reported. Reference Indig, Thackway, Jorm, Salmon and Owen13 Surprisingly, psychiatric comorbidity, which can be associated with such presentations, was not reported.
A particularly extensive hospital monitoring system was employed during the Los Angeles Games, including 46 hospitals, 24 Olympic first aid stations and the three Olympic polyclinics. Reference Weiss, Mascola and Fannin11 Remarkably, a decreased demand for general health services was experienced. No data on psychiatric presentations were reported, although it was not clear whether psychiatric presentations were recorded as part of the monitoring system. A more limited report focusing on nine Olympic sites recorded the reasons for hospital admission, of which there were none for psychiatric disorders. Reference Baker, Simone, Niemann and Daly12
Discussion
The NHS 2012 Programme does not have a pan-London strategy for mental health planning for the Games. Modelling specific to mental health service demand has not been conducted. Prima facie this may not be imprudent, as data from previous Olympics do not suggest there will be a substantial rise in demand for mental health services. There may even be a decrease. However, the lack of data may be more reflective of monitoring practices, priorities in health surveillance systems or variations in service models resulting in people with mental illness being less likely to access or be referred to services.
Difficulty in estimating visitor numbers to the Games adds further uncertainty. Modelling by the Office for National Statistics suggests there will be an additional 510 000 visitors in London each day during the Games period. 3 This projection needs to be cautioned, as predictions for visitor numbers for previous games have been unreliable. Post hoc estimates of visitor numbers show large variations in attendance between games. This variation is likely to be multifactorial, with sociopolitical, cultural and geographical determinants. Both Sydney and Athens received fewer visitors than expected, with Beijing experiencing a 30% reduction of overseas visitors in contrast with the predicted increase. 14 Indeed, there is increasing evidence for displacement of visitors to London, with data published by the European Tour Operators Association in November 2011 indicating that bookings for the 16-day Olympic period were down 95%. 15
London may be considered unique when compared with recent host cities, as it is already well established as one of the most visited cities in the world, accommodating large numbers of visitors. Foreign visitor numbers to Beijing in 2008 were in the region of 4-5 million over the year. 16 In London during the third quarter of 2010 alone (corresponding with the Olympic months of July to September) there were a total of 4.24 million overseas visitors. 17 Greater accessibility through the proximity to the large population density of Europe, with cheap, visa-free travel also contrasts with other recent host cities.
Other factors may also mean mental health demand does not substantially rise during the Games period. The Olympics will run for a relatively short period in relation to the time course of mental illness and visitors are unlikely to stay for long periods and may only hold a ticket for a single event, resulting in a visit lasting only a few days. The incidence of new episodes of mental illness or recurrence of pre-existing illness may therefore be expected to be low. The demography and levels of affluence of visitors attending the Olympics may be different to the profile of regular visitors, due to the need to fund higher travel and accommodation costs. A corollary may also be that private mental health services are accessed in preference to public services. The combination of increased security and cost may also reduce the rate of unplanned travel that can be associated with mental illness, such as impulsive travel in the context of acute mania or other psychoses, which has been the authors’ experience working in central London.
Evidence from the football World Cup indicates that the UK's team performance may positively or negatively have an impact on morbidity. However, we are cautious in extrapolating this evidence to the Olympics as it is open to debate whether the Olympics will garner a level of passion comparable with the World Cup. A study of German football fans found that when they watched their own team they had higher pulse rates and blood pressures than when they watched other teams. Reference Reppel, Franzen, Bode, Weil, Kurowski and Schneider18 Acute cardiovascular events were found to be doubled during a stressful match. Reference Wilbert-Lampen, Leistner, Greven, Pohl, Sper and Völker19 More positively, when a team did well the rate of myocardial deaths fell. Reference Berthier and Boulay20 Notably the suicide rate fell in France during the football World Cup in 1998, which the French team won, with the greatest fall in men aged between 30 and 44. Reference Encrenaz, Contrand, Leffondré, Queinec, Aouba and Jougla21
Implications
The possibility that demand may not dramatically rise does not mean mental health trusts in London can be complacent. High rates of bed occupancy in mental health units may magnify the impact of even small increases in demand for in-patient treatment. 22 Decreased availability of transport, access to embassy support and interpreting services, may increase the length of in-patient stays and the overall burden on units. Antisocial behaviour or behaviour secondary to drug and alcohol misuse may also be misattributed to mental health disorders and lead to greater demand on assessment and liaison services in particular.
The NHS London guidance recommends ‘business as usual’ during London 2012. 23 Although this seems appropriate given the evidence, the degree of uncertainty may make the maxim ‘business as unusual’ more astute.



 Open access
Open access
eLetters
No eLetters have been published for this article.