


Introduction
Choosing Wisely Canada (CWC) aims to improve healthcare quality and delivery by reducing the burden of unnecessary testing, inappropriate treatments, and adverse outcomes for patients. Choosing Wisely recommendations are compiled into lists generated by medical societies in Canada to promote tangible ways for health providers to apply these principles in practice and begin conversations about overutilization in healthcare. As of January 2019, 49 medical societies had published a collective of more than 250 CWC recommendations. Despite the reflection of CWC principles in neurology education, guidelines, and practice, a CWC neurology list was lacking. The Canadian Neurological Society (CNS) approved the creation of a taskforce. Quantitative and qualitative methods were used to generate a CWC list on behalf of the CNS for both neurologist and non-neurologist physicians and trainees, beginning with reviewing Canadian neurology guidelines and American Choosing Wisely recommendations. This was pared down into a final list of seven recommendations and further refined with feedback from practicing neurologists.
Method
A task force was struck and followed the CWC outline for medical societies to generate a list of recommendations (Figure 1). The process began with careful consideration of each of the 45 Choosing Wisely recommendations published by the American Board of Internal Medicine within the realm of neurosciences from numerous American medical societies (American Epilepsy Society, American Association of Neuromuscular and Electrodiagnostic Medicine, American Academy of Nursing, American College of Emergency Physicians, American Geriatrics Society, American Academy of Neurology, and American Academy of Pediatrics). Each recommendation was evaluated based on its applicability to Canadian neurology practice by generalists and specialists. Ten of the 45 neuroscience recommendations were deemed to be both relevant and important for Canadian neurosciences, with minimal overlap with neurology recommendations addressed in other pre-existing CWC lists (Figure 2). The supporting literature was reviewed, and the quality therein was assessed for each of the 10 proposed recommendations. Readers will find references in Figure 2. The recommendations were altered slightly to align with current Canadian neurology guidelines, high-quality reviews, and meta-analyses.

Figure 1: List generation process and stakeholder input.
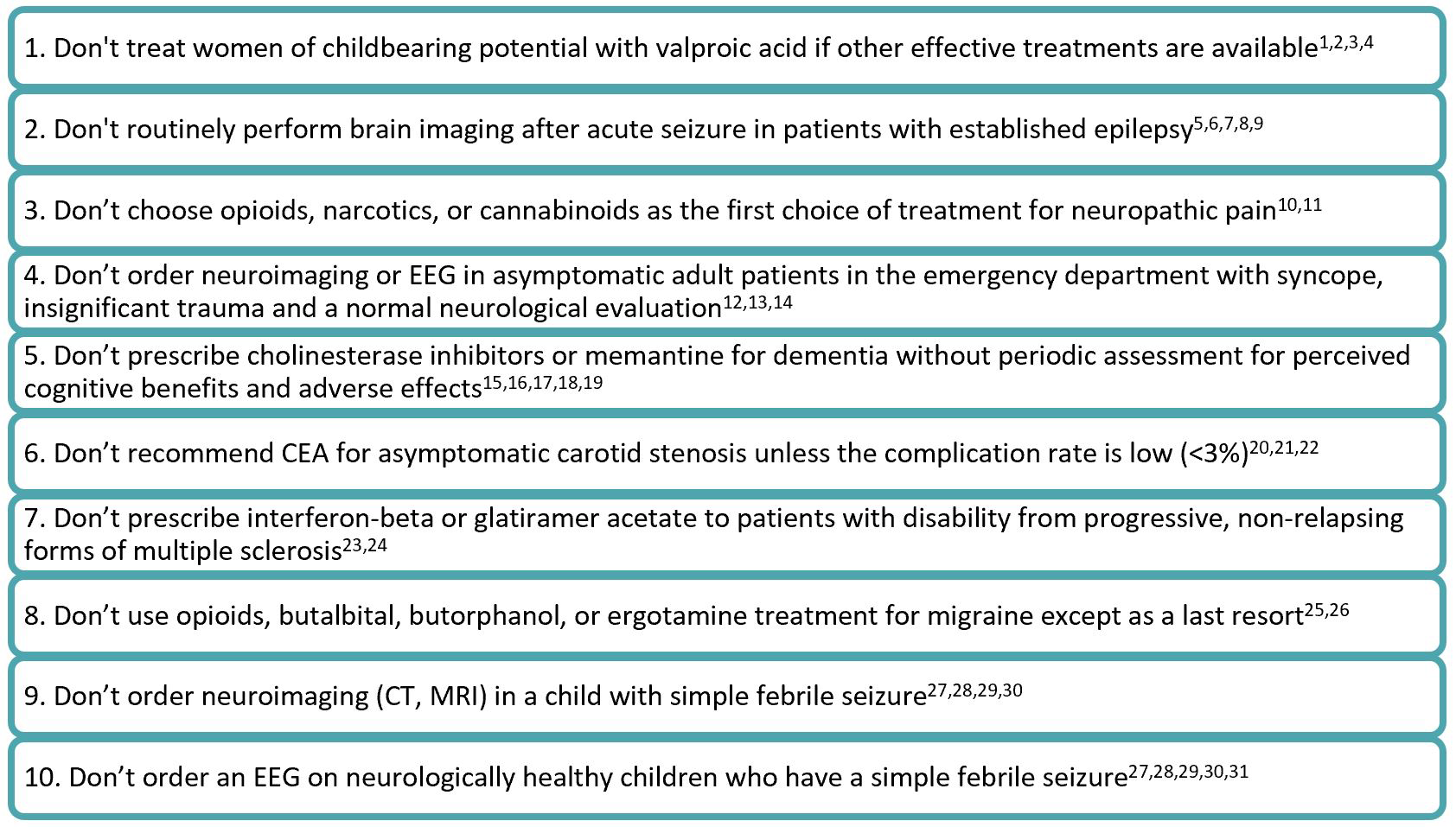
Figure 2: Preliminary list of 10 recommendations adapted from American Choosing Wisely Neurosciences recommendations.Reference Bansal, Jain, Kharbanda, Goyal and Suri1–Reference Harini, Nagarajan and Kimia31
The 10 proposed recommendations were sent to all CNS board members for approval; these recommendations were reviewed and ranked by the CNS members, including neurologists, fellows, and residents. CNS members at large were surveyed regarding their ranking preferences and relevant feedback. The average ranking for each recommendation was scored from which a list of the top five recommendations was compiled.
Results
Survey participants were asked to rank the proposed recommendations from 1 to 10 with the aim of producing a top five list (Figure 3). This quantitative data was combined with qualitative feedback from neurologists across Canada through comments in the survey and verbal input from presentations at conferences. The list of the top five was proposed to CWC who recommended expansion of two of the proposed recommendations (Figure 3: numbers 4 and 5). The list was then expanded into seven recommendations. This allowed for more emphasis for certain points including not using opioids for migraine to fit with CWC’s “Opioid wisely” campaign, which was made separate from butalbitol, butorphenol, and ergotamines for migraines. Additionally, the separation of investigations for minor head trauma and syncope emphasizes that computed tomography should be considered with a validated screening tool for minor trauma which is separate from neuroimaging and electroencephalogram use for syncope.
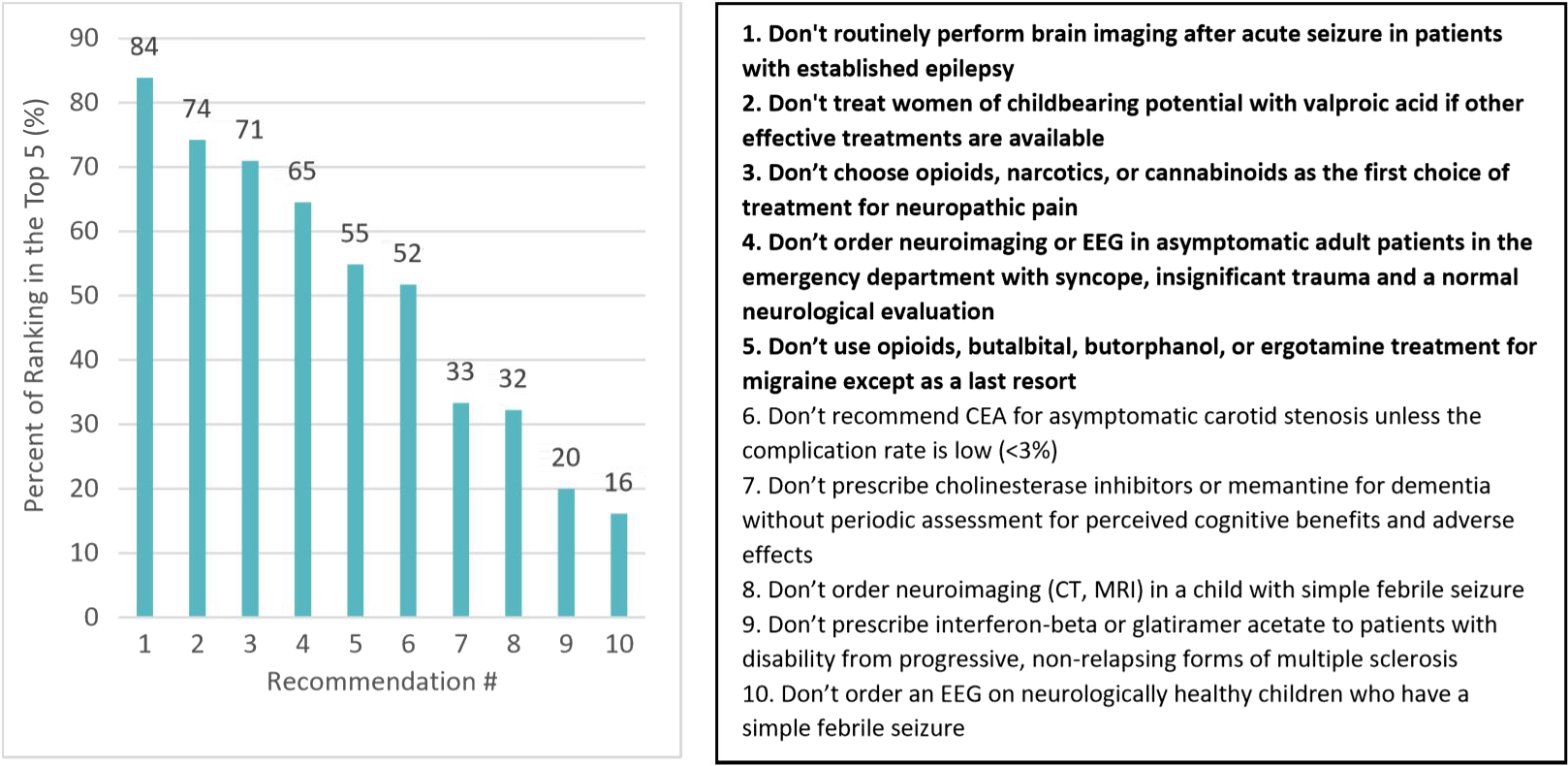
Figure 3: Percentage of each proposed recommendation ranking within the top five by CNS members via online survey (n = 31). Corresponding numbered list of recommendations on the right which emphasizes the top five that were chosen in bold.
Discussion
The list was sent to CWC following CNS membership input and altered for clarity, with feedback from CWC champions from other medical societies. The list was posted and publicized by CWC in January 2020 (Figure 4). Two goals were met. Firstly, to demonstrate support for resource stewardship and patient safety principles in neurology by promoting only what is necessary. Secondly, to generate a usable, evidence-based list of recommendations for physicians, including neurologists and non-neurologists to guide management. Through reducing unnecessary testing and treatments, healthcare spending can be appropriately allocated for evidence-based practices which can help patients and the system at large.
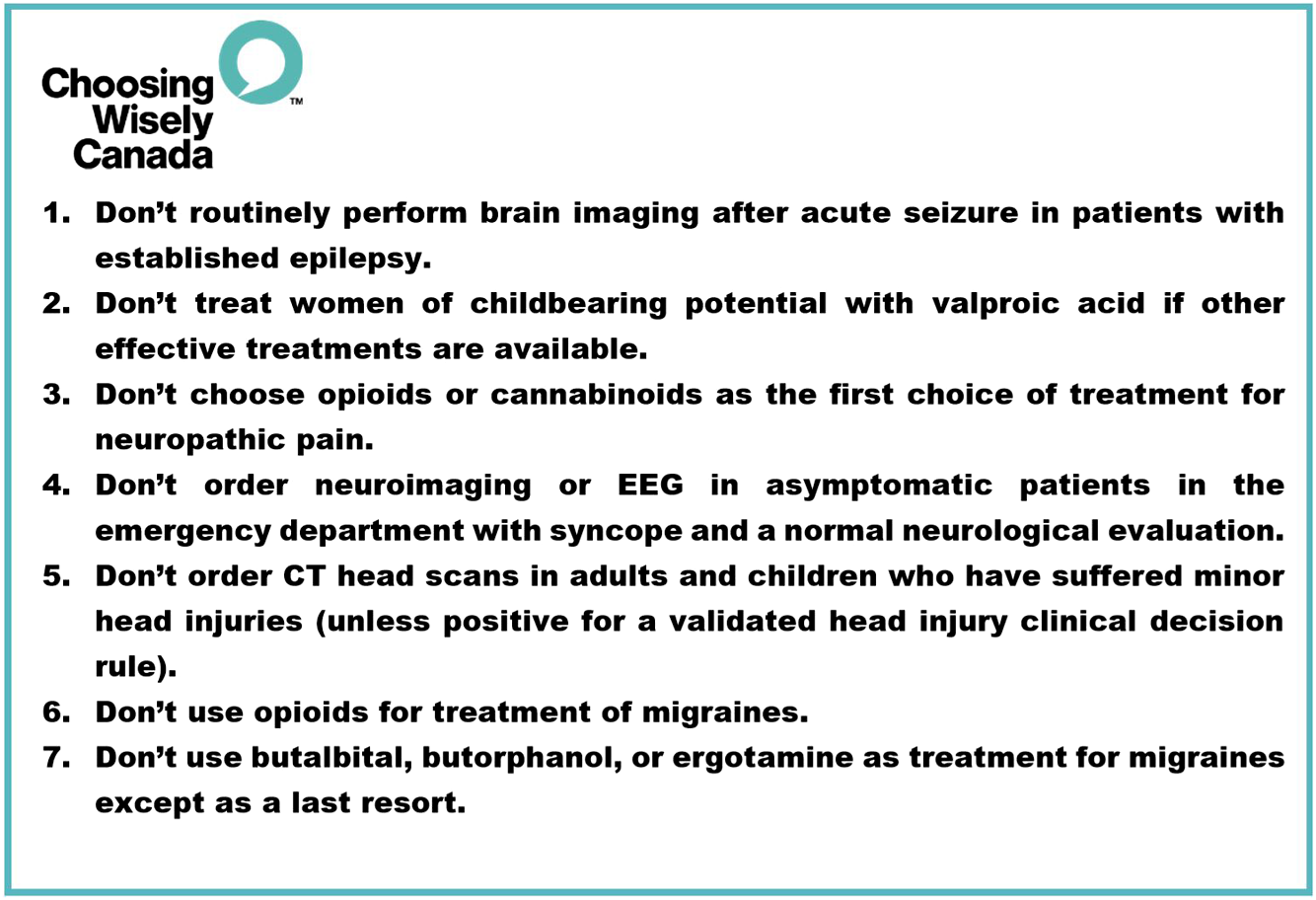
Figure 4: Final list of seven published recommendations in Choosing Wisely Canada January 2020.Reference Harini, Nagarajan and Kimia31
The CWC list might not address specific individual patient complexities and is it not meant to replace clinical judgment. Rather, it provides guidance to the health practitioners. It may serve as a reminder to consider whether imaging, tests, or treatments lacking supportive evidence should be ordered. This list will not replace individual decision-making and careful consideration of each patient will still be necessary. On the other hand, it may help patients in understanding that oftentimes, doing less can lead to better outcomes. Additionally, a succinct list of seven recommendations is simpler to generate and disseminate, but it cannot be all encompassing; there are likely more areas of overuse in clinical neurology that are not addressed in this list. It will also require updates if more or contradicting evidence becomes available. Input from stakeholders was sought to ensure that the most important principles were conveyed in the list on behalf of the CNS. This short list should be one of the small steps in propelling resource stewardship in neurology forward.
Conclusion
Participating in the CWC national campaign is an important health advocacy task that has been undertaken by the CNS. By providing an outline on how the list was generated, it is hoped a review can be conducted at regular intervals to improve care for neurology patients while reducing unnecessary tests and treatments. This list can adapt over time, as treatment paradigms change and arise in neurology.
Acknowledgments
The authors would like to acknowledge members of the CNS who participated in the survey. The authors would like to acknowledge Joanna Wong and Wendy Levinson at CWC for their guidance.
Disclosures
Dr. Costello has received consultancy Honoria from Roche, Alexion. The other authors have no conflicts of interest to declare.
Statement of Authorship
CB: conception, data collection, data analysis and interpretation, drafting the article, and final approval of the version to be published. FC: critical revision of the article and final approval of the version to be published. JMB: critical revision of the article and final approval of the version to be published. PC: design of the work, critical revision of the article, final approval of the version to be published.




