


In their basic biological role, amino acids, molecules containing both an amine and a carboxyl functional group, act as structural units in the construction of protein. Twenty standard amino acids are used in this role. However, recent biochemical research has identified functions beyond protein construction, such as the regulation of immunity by arginine(Reference Morris1) and the control of protein synthesis by leucine(Reference Kimball and Jefferson2). In terms of human research, specific amino acids have been indicated in preventing particular diseases. Arginine, for example, a precursor of NO, has a potential protective effect against CHD(Reference Oomen, van Erk, Feskens, Kok and Kromhout3–Reference Wells, Mainous and Everett5), while a number of studies have investigated the association between methionine and colorectal cancer or adenoma(Reference Harnack, Jacobs, Nicodemus, Lazovich, Anderson and Folsom6–Reference Giovannucci, Stampfer, Colditz, Rimm, Trichopoulos, Rosner, Speizer and Willett9). Results to date remain inconclusive, however, at least partly due to difficulties in assessing dietary intake.
Dietary intake in epidemiological studies is often assessed using FFQ. Before any evaluation of estimated intake can be done, however, the validity of the FFQ must be confirmed. The ability of an FFQ to estimate dietary intake is validated by comparing the estimated intake by the FFQ with that by other methods. Typical methods used for reference are multiple day dietary records (DR) or 24 h recall, which directly measure detailed intake in individuals(Reference Willett10). Another reference method is the measurement of biochemical indicators, which represent the physiological status of individuals responding to the dietary intake of nutrients(Reference Willett10). The relative validity is evaluated by different statistical approaches including correlation, cross-classification and comparison of intake estimates(Reference Willett10). Because errors in dietary assessment are unavoidable, correlations of validity generally tend to be in the range of 0·5–0·7(Reference Willett10). The lower the accuracy, the greater the attenuation of association with the disease.
The aim of the present study was to evaluate the validity of an FFQ for estimating amino acids using 28 d weighed DR as the reference method. To our knowledge, no study has comprehensively evaluated the validity of estimations of the twenty amino acids.
Subjects and methods
Study setting
The Japan Public Health Center-based Prospective (JPHC) Study is a population-based prospective cohort study that consists of two cohorts. The first started in 1990 in Ninohe, Yokote, Saku and Chubu (formerly named Ishikawa) public health centre areas (cohort I); the second started in 1993 in Mito, Kashiwazaki, Chuo-higashi, Kamigoto, Miyako and Suita public health centre areas (cohort II). The aim of the JPHC was to investigate associations between chronic diseases and various lifestyle factors such as diet. The study design and participants in the overall cohort have been described previously(Reference Watanabe, Tsugane, Sobue, Konishi and Baba11). The dietary intake of individuals in these populations was assessed using a semi-quantitative FFQ developed based on data from 3 d weighed DR in a random sample from cohort I(Reference Tsubono, Takamori, Kobayashi, Takahashi, Iwase, Iitoi, Akabane, Yamaguchi and Tsugane12).
Two FFQ validation studies were conducted in subsamples of cohort I and cohort II, the former to validate the FFQ within the population for which it was developed and the latter to validate it in a population for which it was not developed (external validity). The cohort I validation study was initiated in February 1994, and that in cohort II in May 1996. Approximately thirty married couples aged 45–75 years (to age 65 years for cohort I) were recruited through the respective public health centres(Reference Tsugane, Kobayashi, Sasaki, Tsubono and Akabane13, Reference Ishihara, Sobue and Yamamoto14). Subjects from both cohorts were healthy volunteers of normal weight and without dietary restrictions. The majority were salaried workers. Oral or written informed consent from the participants was received before the study. The study did not undergo ethical approval since it was conducted before the advent of ethical guidelines for epidemiology research in Japan, which mandate such approval.
Development of a database for amino acids
Energy and protein intake according to the FFQ and DR were calculated using the Standardized Tables of Food Composition, 4th ed.(15), which include 1622 food items. Because the database for amino acids, published as a follow-up to the Standardized Tables of Food Composition, 4th ed.(15), covered only 18 % of these items, however, a comprehensive database of the amino acid content of foods using four substitution methods was developed. Method A used food products derived from the same species of animal, different parts of the same species, cultivated food products for wild products (or vise versa), food products harvested in different countries, or processed food products for raw material (or vise versa); method B used food products of a similar species; method C used composition values from the US Department of Agriculture; method D used values computed with recipe data. These methodologies have been evaluated using a comparison of actual and substituted values for twenty-one arbitrarily selected foods using Pearson's correlation coefficients (r varied from 0·93 for method D to 0·99 for method A).
Data collection
Data collection has been described in detail elsewhere(Reference Tsugane, Kobayashi, Sasaki, Tsubono and Akabane13, Reference Ishihara, Sobue and Yamamoto14). In brief, each subject completed a 7 d DR during each of the four seasons and two identical FFQ (FFQV and FFQR), conducted for different purposes. The FFQV was completed immediately or 3 months after the last DR was administered to obtain the data required for comparison with the DR. The other FFQ (FFQR) was administered to provide data to evaluate the reproducibility of the FFQV. For the present paper, we analysed the validity of the FFQ in the estimation of amino acids using data from 215 and 350 subjects in cohorts I and II, respectively, who had complete data for the total 28 d DR and the FFQV.
DR were collected over 7 consecutive days in each of the four seasons, except in Chubu (two seasons). Local dietitians instructed the subjects to weigh all foods and beverages with scales and measuring utensils provided, and to record the results in a specially designed booklet. The subjects in cohort I, however, were instructed to use standardised portion sizes for some foods that were difficult to weigh (semi-weighed DR). The subjects described each food, method of preparation, and the names of dishes in detail. They also reported all dietary supplements used, if any. At the end of each season, the DR were reviewed in a standardised manner, and each food was coded using the food item code in the Standardized Tables of Food Composition, 4th ed.(15) by local dietitians. Energy and nutrient intakes were calculated by summing the product of the intake of each food multiplied by the amino acid content of that food.
The self-administered semi-quantitative FFQ consisted of 138 food items and fourteen supplementary questions concerning the use of dietary supplements, dietary habits and others. The results were used to assess the usual dietary intake of the preceding year for each individual. The intake of each food item was calculated by multiplying the frequency of consumption (never, 1–3 times/month, 1–2 times/week, 3–4 times/week, 5–6 times/week, once/d, 1–2 times/d, 4–6 times/d, 7 times/d and more) by the relative portion size (small, medium, and large). The food item code in the Standardized Tables of Food Composition, 4th ed.(15) was also assigned to the respective food item in the FFQ(Reference Sasaki, Kobayashi, Ishihara and Tsugane16), and the daily intakes of energy and nutrients according to the FFQ for each individual were calculated by summing the product of the intake of each food multiplied by the amino acid content of that food for the same nutrients as those calculated for the DR. Because a database for dietary supplements was not available, intake from dietary supplements was not included in calculations for either the DR or FFQ.
Statistical analysis
The mean intakes of total protein and amino acids according to both the 28 d DR (14 d for Okinawa) and FFQ were calculated by sex and cohort group. Percentage differences were calculated using the following formula: (intake according to the FFQ – intake according to the DR)/intake according to the DR. Spearman's rank correlation coefficients between intakes according to the DR and FFQ were calculated for crude value, energy-adjusted (residual model) value and deattenuated value, which was corrected for the attenuating effect of random intra-individual error (deattenuation). Deattenuation was done using the following formula: deattenuated correlation coefficients = ![]() , where r is the observed correlation, λx is the ratio of intra- to inter-subject variation, and nx is number of DR for each subject(Reference Kabagambe, Baylin, Allan, Siles, Spiegelman and Campos17). In addition, the number of subjects classified into the same, adjacent, and extreme categories by joint classification by quintile was computed using energy-adjusted values. Furthermore, Bland–Altman analysis, which assesses the agreement between two methods, was applied for protein intake. This method is achieved by plotting the mean intake from two methods, (FFQ+DR)/2 on the x axis, and the difference between the methods, FFQ − DR on the y axis. Before plotting, protein intake was log-transformed, energy-adjusted by the residual method, and then residuals were added to the constant (predicted protein intake for the mean energy intake) so that the values appear similar to the actual intake values. Overall agreement is assessed by the mean of difference, width of limit of agreement (2 sd) and the dependence of difference on the magnitude of estimates(Reference Flood, Smith, Webb and Mitchell18, Reference Ambrosini, de Klerk, Musk and Mackerras19). All analyses were performed using SAS (version 9.1; SAS Institute Inc., Cary, NC, USA).
, where r is the observed correlation, λx is the ratio of intra- to inter-subject variation, and nx is number of DR for each subject(Reference Kabagambe, Baylin, Allan, Siles, Spiegelman and Campos17). In addition, the number of subjects classified into the same, adjacent, and extreme categories by joint classification by quintile was computed using energy-adjusted values. Furthermore, Bland–Altman analysis, which assesses the agreement between two methods, was applied for protein intake. This method is achieved by plotting the mean intake from two methods, (FFQ+DR)/2 on the x axis, and the difference between the methods, FFQ − DR on the y axis. Before plotting, protein intake was log-transformed, energy-adjusted by the residual method, and then residuals were added to the constant (predicted protein intake for the mean energy intake) so that the values appear similar to the actual intake values. Overall agreement is assessed by the mean of difference, width of limit of agreement (2 sd) and the dependence of difference on the magnitude of estimates(Reference Flood, Smith, Webb and Mitchell18, Reference Ambrosini, de Klerk, Musk and Mackerras19). All analyses were performed using SAS (version 9.1; SAS Institute Inc., Cary, NC, USA).
Results
Subject characteristics are presented in Table 1. Mean age was slightly higher for men than women, and higher for participants in cohort II than cohort I, since cohort II included older subjects.
Table 1 Basic characteristic of the study participants
(Mean values and standard deviations)

DR, dietary records.
Mean intakes of total protein and amino acids according to DR and FFQ are presented in Table 2. Amino acid intake according to the FFQ was lower than intake by the DR. The difference was greater for men than women, and for the cohort II than cohort I population (median percentage differences of twenty amino acids were − 14 % for cohort I men, − 4 % for cohort I women, − 18 % for cohort II men and − 9 % for cohort II women).
Table 2 Amino acid intake assessed with dietary records (DR) for 28 d (or 14 d for Okinawa) and FFQ and their correlations
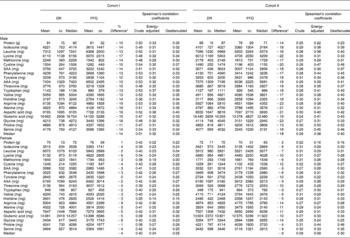
SAA, sulfur-containing amino acids (methionine and cystine); AAA, aromatic amino acids (phenylalanine and tyrosine).
* (Intake according to the FFQ – intake according to the DR)/intake according to the DR.
Deattenuated Spearman's correlation coefficients of energy-adjusted intakes of protein and amino acids according to the FFQ and corresponding intake according to the DR ranged from 0·15 to 0·52. Median correlation coefficients for twenty amino acids were 0·33 and 0·25 for cohort I men and women, and 0·40 and 0·30 for cohort II men and women, respectively.
A comparison of FFQ and DR for amino acid intake based on joint classification by quintile is presented in Table 3. The median percentage of subjects whose amino acid intake according to the DR and FFQ were categorised into the same quintile was 25–32 %, and was higher among men than women, and in cohort I than cohort II. However, fewer subjects had their amino acid intake categorised into the extreme quintile in cohort II than cohort I.
Table 3 Comparison of FFQ with dietary records (DR) for amino acid intake based on joint classification by quintile (%)*
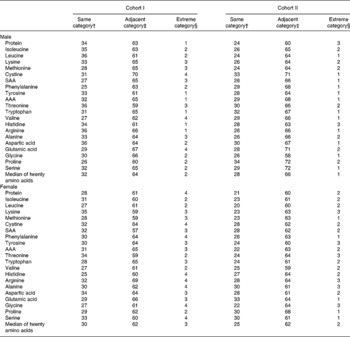
SAA, sulfur-containing amino acids (methionine and cystine); AAA, aromatic amino acids (phenylalanine and tyrosine).
* Energy-adjusted intakes of amino acids according to DR and FFQ for each individual classified into quintiles.
† Percentage of subjects whose FFQ and DR were classified into the same quintile.
‡ Percentage of subjects whose FFQ and DR were classified into the same or adjacent quintile.
§ Percentage of subjects whose FFQ and DR were classified into the extreme quintile (lowest or highest).
Agreement between the two methods examined by the Bland–Altman plot in Fig. 1 showed that the mean difference for men was greater for cohort II, indicating that the degree of relative bias was greater for the external population. Further, the larger width of limit of agreement indicated greater random error in the external population.

Fig. 1 Bland–Altman method of assessing agreement between the FFQ and dietary records (DR) for energy-adjusted protein intake in (a) cohort I males (y = 0·36x − 45·7; P < 0·01), (b) cohort II males (y = − 1·03x+58·1; P < 0·01), (c) cohort I females (y = 0·18x − 24·6; P = 0·19) and (d) cohort II females (y = − 1·11x+76·7; P < 0·01). LOA, limit of agreement.
Discussion
Here, we evaluated the validity of an FFQ using DR as a reference method. Levels of intake were underestimated by the FFQ, and its validity for ranking individuals varied from low to moderate.
Although associations between the intake of specific amino acids and diseases have been examined in several studies, the validity of FFQ in estimating dietary intake has not been evaluated(Reference Harnack, Jacobs, Nicodemus, Lazovich, Anderson and Folsom6, Reference Giovannucci, Stampfer, Colditz, Rimm, Trichopoulos, Rosner, Speizer and Willett9). Because the collection of information on the amino acid components of all foods is both expensive and time-consuming, obtaining intake data from a DR, which requires the composition data of a variety of foods, is not trivial. Here, we used a composition table for amino acids developed by substitution methods. To our knowledge, the present study is the first to comprehensively evaluate the validity of an FFQ in the estimation of dietary amino acid intake.
Underestimation was observed with amino acid intake, particularly among men. In analyses among our validation study subjects, energy intake estimated using the FFQ was closely similar to that using DR among men, and somewhat overestimated among women. Among macronutrients, total fat intake was overestimated by the FFQ among men and women, whereas protein was underestimated, as indicated in the present study(Reference Ishihara, Sobue and Yamamoto14, Reference Tsugane, Kobayashi and Sasaki20), most likely because of missing food items or inadequate portion size estimation by the FFQ. In fact, the results from our previous study showed that fish, meat and eggs, which contribute to protein intake, were more strongly underestimated in the external population (cohort II)(Reference Ishihara, Sobue and Yamamoto14). We cannot deny the possibility that the reference method (DR) underestimated the true intake of individuals such that the underestimation by the FFQ was exacerbated, since we did not use a more objective method such as doubly labelled water(Reference Kroke, Klipstein-Grobusch, Voss, Moseneder, Thielecke, Noack and Boeing21, Reference Livingstone22). However, we assume that the underestimation was not particularly severe since energy intake seemed appropriate for the sex and age of those participants of normal weight. In addition, protein intake was higher than the intake level in Japanese populations of the same age as the participants. According to the 2004 National Health and Nutrition Survey, the average protein intake for men and women aged 50–59 years is 82·0 and 70·5 g, respectively(23).
The validity of our FFQ for ranking individuals by amino acid intake was lower than that by the general level of other nutrients in similar studies, particularly among women. Results from previous validation studies of a number of FFQ among Japanese(Reference Date, Fukui and Yamamoto24–Reference Egami, Wakai and Kato26), including ours(Reference Tsugane, Kobayashi and Sasaki20, Reference Sasaki, Kobayashi and Tsugane27), tend to show lower validity than those from Western populations, possibly because of the complexity of the Japanese diet, for example, in the variety of mixed dishes, seasonal variation, and others. It is also possible that relatively poor agreement between the FFQ and the DR might be due to the heavy burden of 28 d weighed dietary recording. Lower validity due to instrument measurement error would of course attenuate the association between intake and disease, in turn indicating the need for awareness of the difficulty in distinguishing between a true null v. an attenuated association.
Correlation coefficients for amino acids were similar to that for protein within the same group. Although protein consists of amino acids, the amino acid content of individual foods and individual intake varies. Nevertheless, the present results suggest the possibility of surrogating the validity of protein determination for that of amino acids. Protein is one of the few nutrients whose intake is directly reflected by an available recovery biomarker, i.e. 24 h urine N(Reference Bingham28). The fact that the validity of amino acid intake could be surrogated by that of protein may suggest the possibility of using this biomarker to assess amino acid intake, a valuable notion if confirmed, as no single ideal biochemical indicator of dietary intake of amino acids is known(Reference Willett10). One weakness of the present study is that we did not measure urinary N, which would have greatly strengthened the results. If feasible, a future study of this in our frozen 24 h urine samples would be of interest.
A limitation of the present study was that amino acid intake from supplements was not included in the estimations of intake. However, given that very few subjects (less than 2 %) consumed supplements that included amino acids, intake from this source is probably negligible.
Compared with 28 d DR, the FFQ is a valid tool to rank participants according to high and low intakes of amino acids in this population of Japanese men and women. In conclusion, the validity of this FFQ in estimating amino acid intake was low to moderate. However, because the degree of validity in estimating protein and amino acids was similar, the use of protein intake as a surrogate for that of amino acids in investigations of the association between specific amino acids and diseases may be possible.
Acknowledgements
The authors wish to express their appreciation to the local staff in each study area, especially to the local dietitians for their efforts in conducting the dietary survey. J. I. was awarded a research resident fellowship from the Foundation for the Promotion of Cancer and Research (Japan) for the 3rd Term Comprehensive 10-year Strategy for Cancer Control. J. I. performed the data analysis and drafted the manuscript. H. T. developed the database for amino acids. M. I. was in charge of conducting the JPHC Study. S. T. was the principal investigator of the JPHC Study.
The investigators in the validation study of the self-administered FFQ in the JPHC Study (the JPHC FFQ Validation Study Group) and their affiliations at the time of the study were: S. T., S. Sasaki and M. Kobayashi, Epidemiology and Biostatistics Division, National Cancer Center Research Institute East, Kashiwa; T. Sobue, S. Yamamoto and J. I., Cancer Information and Epidemiology Division, National Cancer Center Research Institute, Tokyo; M. Akabane, Y. Iitoi, Y. Iwase and T. Takahashi, Tokyo University of Agriculture, Tokyo; K. Hasegawa and T. Kawabata, Kagawa Nutrition University, Sakado; Y. Tsubono, Tohoku University, Sendai; H. Iso, Tsukuba University, Tsukuba; S. Karita, Teikyo University, Tokyo; the late M. Yamaguchi and Y. Matsumura, National Institute of Health and Nutrition, Tokyo.
We have no conflicts of interest to declare.




