


Introduction
Probable mental health disorders in British children aged 5 –16 years have increased from 10.8% to 16.0% over three years (Newlove-Delgado et al., Reference Newlove-Delgado, McManus, Sadler, Thandi, Vizard, Cartwright and Ford2021). Vulnerability and risk factors predispose children to the development of anxiety and depression symptoms (Ho et al., Reference Ho, Zhang, Lai and Dai2021; Nguyen et al., Reference Nguyen, Rawana and Flora2011). The presence of vulnerability factors such as trait anxiety during the transition into early adolescence, which is a sensitive period when critical events, including puberty, might affect brain development, and increase the vulnerability of children to developing anxiety and depression symptoms (Andersen, Reference Andersen2003; McGuire et al., Reference McGuire, McCormick, Koch and Mendle2019).
Attentional control might mediate the association between high trait anxiety and trajectories of depression symptoms. Children with high trait anxiety are more likely to develop depression symptoms (DeJong et al., Reference DeJong, Fox and Stein2019; Knowles & Olatunji, Reference Knowles and Olatunji2020a). According to attentional control theory, trait anxiety leads to a poorer ability to inhibit attention to task-irrelevant stimuli and to flexibly switch attention (Eysenck et al., Reference Eysenck, Derakshan, Santos and Calvo2007). Based on the cognitive theory of emotional symptoms, poor attentional control ability might lead to negative attentional bias and consequently contribute to depression symptoms (K. Mogg & Bradley, Reference Mogg and Bradley2018). Moreover, children with poor attentional control might be more likely to ruminate over negative things, which increases the probability of developing depression symptoms (DeJong et al., Reference DeJong, Fox and Stein2019; Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015). Nevertheless, no studies have investigated whether attentional control might mediate the association between trait anxiety and the trajectories of depression symptoms. These findings contribute to a more comprehensive understanding of the relationship of trait anxiety to the development of depression symptoms and expand attentional control theory to explain depression symptoms in a developmental context during the transition into early adolescence.
Prevalence and impact of depression symptoms
Previous research has revealed that children have heterogeneous trajectories of depression symptoms. For example, a study assessed trajectories of depression symptoms in nonclinical adolescents without diagnosed depression (10–15 years) three times over one year with latent growth curve modeling (McLaughlin & King, Reference McLaughlin and King2015). The study revealed that the level of depression symptoms was stable across the period. Another study investigated the trajectories of irritability, depression, and anxiety symptoms in nonclinical community children from early childhood to early adolescence (3 to 11 years) (Ezpeleta et al., Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020). The study revealed that 67.1% showed stably low trajectories of all variables; 11.2% had trajectories of stably high depression and anxiety; and 21.7% had trajectories of increasing anxiety and stable mean-level depression (Ezpeleta et al., Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020). Overall, from childhood to adolescence, the majority of nonclinical children showed adaptive trajectories of depression symptoms, which is defined by stably low or decreasing depression symptoms. The minority of children had a maladaptive trajectory of depression symptoms, which is defined by a stably high or increasing level of depression symptoms. Previous evidence showed that girls had higher depression symptoms than boys (Fernández et al., Reference Fernández, Crivelli, Magrath, Allegri, Picco and Pedreira2022). Gender differences were also reported in the trajectories of depression symptoms in early adolescents. Four trajectories of depressive symptoms were found in girls, but three trajectories were revealed in boys (Fernandez Castelao & Kröner-Herwig, Reference Fernandez Castelao and Kröner-Herwig2013).
Early-onset anxiety and depression symptoms in childhood predict anxiety and depression disorders in adulthood (Cohen et al., Reference Cohen, Andrews, Davis and Rudolph2018; Ranøyen et al., Reference Ranøyen, Gulliksrud, Indredavik and Stenseng2018). Moreover, anxiety and depression symptoms have a close relationship with life satisfaction. Higher anxiety and depression symptoms predict lower life satisfaction and lower psychological well-being (Lopes & Nihei, Reference Lopes and Nihei2021). Therefore, research on the vulnerability factors of depression symptoms in children is of paramount concern.
Factors associated with depression symptoms
Trait anxiety
Trait anxiety characterizes an individual’s disposition to evaluate various circumstances as threatening and experience disproportionately high anxiety in response to even objectively less stressful circumstances (Spielberger, Reference Spielberger1973). Children high in trait anxiety are more likely to experience high-level anxiety than children with low trait anxiety across different situations. Moreover, gender differences were present in trait anxiety. Previous research has suggested that females have higher trait anxiety than males (Burton & Nkwo, Reference Burton and Nkwo2022).
Trait anxiety is a transdiagnostic factor for depression symptoms. The relationship between trait anxiety and depression symptoms might be explained by the tripartite model (Clark & Watson, Reference Clark and Watson1991). According to tripartite theory, anxiety symptoms and depression symptoms share the same construct of negative affectivity. Trait anxiety was previously shown to represent an overall tendency for negative affectivity (Knowles & Olatunji, Reference Knowles and Olatunji2020). Thus, high trait anxiety might predict depression symptoms because it predicts the level of negative affectivity in children’s transition into adolescence.
Cognitive flexibility is defined by the capability to adjust cognitive processing strategies according to changing or unpredictable situations (Jacques & Zelazo, Reference Jacques, Zelazo, Wilde Astington and Baird2005). A cross-sectional study assessed trait anxiety and depression by self-reported inventories and revealed that the higher risk of people with high trait anxiety for developing high depression was buffered by high cognitive flexibility (Wang et al., Reference Wang, Li, Xu, Liu, Wu, Lu, Xie, Peng and Wang2019b). Although people with high trait anxiety are likely to experience high anxiety symptoms in situations, if they can adapt their cognitive strategies to stress, for example, using a more adaptive appraisal of stressful situations, they are less likely to develop high depression symptoms. This finding further supported the relationship of trait anxiety to depression symptoms, providing some rationale for examining the relationship between trait anxiety and the trajectories of depression symptoms. A study recruited young people aged 15 to 25 years who received randomized controlled treatment for moderate to severe major depressive symptoms. The study found that higher trait anxiety predicted higher suicidal ideation (Moller et al., Reference Moller, Badcock, Hetrick, Rice, Berk, Witt, Chanen, Dean, Gao, Cotton and Davey2023). The findings showed that high trait anxiety might precede and prospectively affect the development of depression symptoms, thus providing some evidence for the predictive values of trait anxiety for the developmental trajectories of depression symptoms.
In early adolescence, a longitudinal study recruited children aged 8–14 years who were diagnosed with generalized anxiety disorder. The study showed that high trait anxiety at pretreatment was associated with high depression symptoms at posttreatment (Chambers et al., Reference Chambers, Power and Durham2004). For children between the ages of 12–18 years, high trait anxiety explained why more irritable children were prone to developing depressive symptoms (Malhi et al., Reference Malhi, Das, Outhred, Bell, Gessler and Mannie2021a). These two studies showed that the relationship of trait anxiety and depression symptoms can be replicated in children and adolescents, providing the foundation for future studies to investigate the predictive value of trait anxiety for the developmental trajectories of depression symptoms for children and adolescents. However, little longitudinal research has been conducted to understand how trait anxiety predicts the developmental trajectories of depressive symptoms, especially during early adolescence, which hinders a developmental perspective on the relationship of trait anxiety to depression.
Attentional control
Attention consisted of a goal-directed top-down attentional system and a stimulus-driven bottom-up attentional system (Corbetta & Shulman, Reference Corbetta and Shulman2002). The goal-directed attentional system involves effortfully shifting attention to pursue goals. Attentional control derived from the goal-directed attentional system is the ability to shift and focus attention (Mogg & Bradley, Reference Mogg and Bradley2016). Moreover, attentional control might be an element of effortful control that represents a personality trait to shift and focus attention (Derryberry & Rothbart, Reference Derryberry and Rothbart1997; Olatunji et al., Reference Olatunji, Knowles and Cole2021). Evidence has suggested that gender differences in attentional control are significant (Riley et al., Reference Riley, Okabe, Germine, Wilmer, Esterman and DeGutis2016), showing that females have worse attentional control than males.
Attentional control is an important correlate for depression symptoms. A study assessed attentional control by a self-report inventory in adults seeking treatment for anxiety and depression symptoms. The study found that difficulty in attentional control might be related to more rumination, which led to more depressive symptoms (DeJong et al., Reference DeJong, Fox and Stein2019; Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015). Thus, one of the mechanisms linking self-reported attentional control and depression symptoms might be rumination. Children with poor self-reported attentional control might have difficulty focusing on ongoing tasks and tend to ruminate over negative things (DeJong et al., Reference DeJong, Fox and Stein2019; Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015). A strong tendency to ruminate over negative information contributes to depressive feelings (DeJong et al., Reference DeJong, Fox and Stein2019; Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015).
Moreover, based on the integrative cognitive model of anxiety symptoms (Mogg & Bradley, Reference Mogg and Bradley2018), top-down attentional control regulates bottom-up threat detection. Poorer attentional control contributes to an enhanced bottom-up threat detection system, leading to higher attention toward threats. Attention to negative stimuli more than neutral or positive stimuli is a vulnerability factor, contributing to anxiety and depression symptoms (Mogg & Bradley, Reference Mogg and Bradley2018). A study found that people with low self-reported attentional control were more likely to attend to mild negative stimuli, as was measured by the dot-probe paradigm, suggesting that attentional control can modify negative attentional biases (Dana van et al., Reference van Son, Angelidis, Hagenaars, van der Does and Putman2018 Reference van Son, Angelidis, Hagenaars, van der Does and Putman). Another study provided electrophysiological evidence for the causal effect of poor attentional control on the development of negative attentional bias in socially anxious individuals (Yuan et al., Reference Yuan, Mao, Chen, Zhang and Cui2019). Thus, negative attentional bias is another mechanism for the relationship between depression symptoms and attentional control. Attentional control also played a significant moderating role in the relationship between trait anxiety and negative attentional bias. In children, a study by Susa et al. (Reference Susa, Pitică, Benga and Miclea2012) found that higher negative and lower positive attentional biases were related to higher anxiety only for children with low attentional control; the associations were insignificant for children with high attentional control.
For children, a study that recruited nonclinical children showed that poorer self-reported attentional control was related to more psychopathological symptoms, which might be mediated by children’s self-efficacy (Muris et al., Reference Muris, Mayer, van Lint and Hofman2008). Therefore, poor ability to control attention might be negatively related to children’s self-efficacy, which was another mechanism underlying the association between attentional control and depression symptoms. Children with poor attentional control might not believe that they can successfully complete tasks. This might increase the likelihood of feelings of helplessness and depression. Empirical findings have supported the important role of attentional control in the development of depression symptoms. An intervention study assessed the relationship between self-reported attentional control to respond to treatment for depression and depression relapse in depressive patients. The study found that lower self-reported attentional control predicted higher depression symptoms and relapse of depressive symptoms after treatment (Buckman, Saunders, Fearon, Leibowitz, & Pilling, Reference Buckman, Saunders, Fearon, Leibowitz and Pilling2019).
Although these studies established the relationship between poor self-reported attentional control and high depression symptoms, insufficient studies have adopted a longitudinal design to assess the effect of self-reported attentional control on the development of depressive symptoms, especially in children. Whether self-reported attentional control predicts heterogeneous developmental patterns in children remains unknown. This knowledge would help predict the developmental patterns of depression symptoms in at-risk children with poor attentional control, especially during the critical period of transition into early adolescence, when vulnerability factors might predispose children to develop more severe emotional disorders.
Attentional control theory
An attentional control system regulates the bottom-up stimulus-driven attentional systems and is responsible for shifting attention toward threatening or rewarding stimuli. According to attentional control theory, trait anxiety impairs information processing efficiency as well as the efficiency of the executive system (Eysenck et al., Reference Eysenck, Derakshan, Santos and Calvo2007). These factors lead to a poorer ability to inhibit attention to task-irrelevant stimuli and to flexibly switch attention (Eysenck et al., Reference Eysenck, Derakshan, Santos and Calvo2007). Thus, trait anxiety impairs attentional control, leading to poor efficacy and effectiveness of cognitive performance. Due to the impairment of attentional control, people with high trait anxiety need to exert additional mental effort to sustain cognitive performance (Eysenck & Derakshan, Reference Eysenck and Derakshan2011). Recently, attentional control theory was supported with neuroimaging evidence revealing the relevant cognitive processes and associated neural network underlying the association between anxiety and attentional control (Eysenck et al., Reference Eysenck, Moser, Derakshan, Hepsomali and Allen2023).
Previous empirical studies have suggested that high trait anxiety is associated with poor self-reported attentional control. A study has shown that high trait anxiety is related to lower self-reported attentional control in adults (Takil & Sari, Reference Takil and Sari2021). Moreover, another study showed that participants who had high trait anxiety had poor neuropsychological performance that indicated low attentional control (Rezaei et al., Reference Rezaei, Hosseini Ramaghani and Fazio2017). The study lent support to the relationship of trait anxiety and attentional control. However, these two studies were cross-sectional and could not suggest whether high trait anxiety impaired attentional control. A longitudinal study with 120 adolescents aged 18 years or younger revealed that high trait anxiety prospectively predicted low self-reported attentional control, supporting that higher trait anxiety might weaken self-reported attentional control (Ho et al., Reference Ho, Yeung and Mak2017b).
Because high trait anxiety and poor attentional control have been shown to predict depression symptoms, high trait anxiety might predict depression symptoms through the mediating pathway of attentional control. Previous studies have shown that high trait anxiety predicts high depression symptoms. For instance, in 178 depressive patients, higher trait anxiety predicted a worse response to treatment for depression symptoms (Min et al., Reference Min, Lee, Lee, Lee and Chae2012). Based on attentional control theory, children with high trait anxiety are more likely to have low self-reported attentional control. For example, a study suggested that high trait anxiety reduces attentional control, which partially explained the association between trait anxiety and mindfulness (Walsh et al., Reference Walsh, Balint, Smolira Sj, Fredericksen and Madsen2009). Reduced attentional control, in turn, might lead to higher depression symptoms. Empirical evidence suggests that attentional control contributes to depression symptoms via rumination (Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015). Therefore, attentional control might account for the association between trait anxiety and depression symptoms.
Although previous empirical evidence and theory imply that self-reported attentional control might mediate the association between trait anxiety and depression symptoms in children, no research has tested the mediating effect of self-reported attentional control on the relationship between trait anxiety and depression symptoms in children. The evidence would provide empirical support for the mechanism underlying the relationship of trait anxiety to the development of depression symptoms. Additionally, the results might further expand attentional control theory to explain the development of depression during the critical period of transition into early adolescence.
The current study
Based on the above literature review, the research questions for the current study include (1) how trait anxiety predicted developmental trajectories of depression symptoms, (2) how attentional control predicted developmental trajectories of depression symptoms, and (3) whether attentional control was the mediator for the relationship of trait anxiety to the trajectory membership of depression symptoms during transition into early adolescence. To address the research questions, the current study adopted a longitudinal design to assess depression four times across 18 months in children during the transition into early adolescence. It aimed to reveal (1) the predictive value of trait anxiety and attentional control for the trajectories of depression symptoms and (2) the mediating effect of attentional control on the relationship of trait anxiety to the trajectory membership of depression symptoms during the transition into early adolescence.
According to previous studies, it was hypothesized that (1) high trait anxiety and low attentional control might predict a higher likelihood of showing the developmental trajectory of high depression symptoms during early adolescence. Moreover, it was hypothesized that (2) attentional control might have a mediating effect on the association between high trait anxiety and the developmental trajectories of depression symptoms. (3) It was also hypothesized that girls might have higher trait anxiety and poorer attentional control than boys. Moreover, girls might be more likely to show a trajectory of high depression symptoms than boys.
The current study adopted latent class growth modeling (LCGM) to reveal the trajectory of depression symptoms. LCGM is different from growth curve modeling in its ability to reveal multiple distinct trajectories rather than a single general changing pattern (Bollen & Curran, Reference Bollen and Curran2006; Mathiesen et al., Reference Mathiesen, Sanson, Stoolmiller and Karevold2009). LCGM can categorize children into homogeneous groups based on their trajectories across a period, which is particularly suitable for revealing low and high trajectories of symptoms (Xu et al., Reference Xu, Huebner and Tian2021). Thus, latent class growth analysis was used in the current study.
Method
Participants
Primary schools in Hong Kong and mainland China were approached for permission to conduct this study as part of a larger research project. Children from Grade three of the primary school in Shenzhen were selected because these students were 9 to 10 years old and were in transition into early adolescence. The exclusion criteria were (1) not being able to fluently speak or understand simplified Chinese and (2) having any psychological disorders. The second criterion was added for two reasons: first, the study expected that the findings could provide implications for the nonclinical population to help prevent the development of anxiety symptoms. Second, (2) because the sample was from a nonclinical population where the majority of the participants would not have physiological and psychological disorders, very few of the participants who have physiological or psychological disorders are very likely to give responses to the questionnaire that would be excluded from the dataset as outliers (e.g., extremely high anxiety or depression level).
Children who failed to fill out one of the questionnaires or dropped out of the study were excluded. The final dataset comprised 264 students with an average age of 9.56 years (SD = .50) (138 girls and 124 boys; 2 did not indicate their gender). Eight percent were born in Hong Kong, and 92% were born in mainland China. A total of 321 students who agreed to participate in the study completed the first assessments. Seventeen children from the first assessment did not attend the second assessment. Eight children from the second assessment did not finish the third assessment. Ten children who completed the third assessment did not complete the fourth assessment.
Measurement
Trait anxiety
The Chinese version of Spielberger’s State-Trait Anxiety Inventory—Trait Anxiety Scale (STAI-T; Cao & Liu, Reference Cao and Liu2015) was used to measure children’s tendency to experience high anxiety in response to stressful situations. The scale includes 20 items (e.g., “I worry too much”) rated on a Likert scale from 1 (Not at all) to 4 (Always). Scores from each item were summed to calculate the total trait anxiety scores. High scores suggested higher trait anxiety. The scale had good internal reliabilities with Cronbach’s alpha = .842 in the current study.
Depression symptoms
The Chinese version of the Major Depression Disorder (MDD) subscale from the Revised Child Anxiety and Depression Scale (RCADS; Piqueras et al., Reference Piqueras, Martín-Vivar, Sandin, San Luis and Pineda2017) was used to measure depression symptoms in children. The MDD subscale had 10 items rated on a 4-point Likert scale (0–3). The scale showed high internal consistency in the four assessments (MDD scale: Cronbach’s Alpha = .878 at Time 1; Cronbach’s Alpha = .865 at Time 2; Cronbach’s Alpha = .877 at Time 3; Cronbach’s Alpha = .876 at Time 4). Total depression scores were calculated by summing the scores for each item. Higher depression scores indicated higher depression symptoms.
Attentional control
The Chinese version of the Attentional Control Scale (ACS) (Derryberry & Reed, Reference Derryberry and Reed2002) was administered to children to measure attentional control. Items were rated on a 4-point Likert scale, ranging from 1 to 4 (1 = “almost never” and 4 = “always”). An example item includes “Hard for me to concentrate on a difficult task when there is noise around.” To assess the structural validity of the 20-item scale to measure attentional control in children, confirmatory factor analysis (CFA) was performed on the original structure of the full scale (20 items) from Ólafsson et al. (Reference Ólafsson, Smári, Guðmundsdóttir, Ólafsdóttir, Harðardóttir and Einarsson2011). CFA was performed because the factor structure of the ACS was previously validated with EFA (Ólafsson et al., Reference Ólafsson, Smári, Guðmundsdóttir, Ólafsdóttir, Harðardóttir and Einarsson2011). As a result, 11 items from the scale were shown to have good structural validity (refer to Supplementary Information for CFA). Consequently, these 11 items were used to measure attentional control in the current study (refer to S. Table 1 for the factor loading of the 11-item ACS). The 11 items from the scale had good internal consistency (Cronbach’s α = .837) at Time 1. Total attentional control scores were calculated by summing scores from the 11 items. Higher attentional control scores indicated higher attentional control difficulty.
Table 1. Mean (standard deviation) of psychological variables

Note. *p < .05. **p < .01.
Procedure
Ethics approval was obtained from the Human Subjects Ethics Sub-Committee of the university. Students and their parents were informed of the purpose and the procedure of the study from the information sheet. If children and their parents agreed to participate in the study, they signed the assent form and submitted the assent form together with the signed parents’ informed consent form to teachers and researchers. Children who submitted these forms could participate in the study.
At time 1, participants completed the first assessment, including the STAI, the MDD subscale, and the ACS, in the classrooms. After six months, students completed the MDD subscale in three follow-up assessment sessions from Time 2 to Time 4 with an interval of six months. Students’ questions were answered by a researcher and a teacher, who also collected the questionnaires and ensured the safety of students. The assessment session was 40 minutes. The whole study lasted for 18 months.
Statistical analyses
Demographic statistics were first presented. The effect of gender on psychological variables was tested by independent t tests. Using SPSS version 22, a repeated ANOVA was conducted to examine the effect of gender and time as well as the interaction between gender and time on depression symptoms. The gender difference in trait anxiety, as well as attentional control at Time 1, was also assessed. Next, the association among these psychological variables was assessed by Pearson’s partial correlation, controlling for gender.
To identify the trajectories of depression symptoms, latent class growth modeling (LCGM) was performed with Mplus 7.11 (Muthén & Muthén, 2012). First, the unconditional LCGM was performed to establish the trajectories of depression symptoms. Next, trait anxiety and attentional control were input as predictors of the LCGM model, and the conditional model of LCGM was performed.
Models for the developmental trajectories of depression symptoms were tested from the two-class model until the test showed that the k model was not better than the k-1 class model. The best-fitting model was evaluated and compared based on the following criteria. Lower Bayesian Information Criterion (BIC) and lower Akaike Information Criteria (AIC) indicate better model fit (Kline, Reference Kline2005). Significant p values of the Lo-Mendell-Rubin likelihood ratio test (LMR–LRT), the Vuong–Lo–Mendell–Rubin likelihood ratio test (VLMR), and the adjusted Lo–Mendell–Rubin likelihood ratio test (Adj. LMR) suggested that the k model was better than the k-1 class model (Kline, Reference Kline2005). Additionally, a better model fit would be demonstrated by a value of entropy (range 0 ∼ 1) closer to 1 (Kline, Reference Kline2005). Additionally, only the model that had at least 1% of participants in each class was selected (Jung & Wickrama, Reference Jung and Wickrama2008). Whether there was a gender difference in the trajectory membership of depression was assessed by the chi-square test.
The trajectories of depression symptoms from the conditional LCGM model were used in the logistic regression analysis as the outcome variable to assess whether trait anxiety and attentional control were predictors of the trajectories of depression symptoms in children. Finally, mediational analysis with attentional control as the mediator for the relationship of trait anxiety to the trajectory of depression was performed by the PROCESS macro v3.5 for SPSS (Hayes, Reference Hayes2013). The PROCESS macro can conduct mediation analysis for categorical outcome variables if the variable is dichotomous (Hayes, Reference Hayes2013).
Results
Preliminary analyses
The demographic statistics were first presented. Refer to Table 1. Gender had a significant effect on trait anxiety, t (260) = 2.836, p < .001; girls had higher trait anxiety than boys. Gender did not have a significant effect on attentional control, t (255) = .667, p = .505. Then, a repeated ANOVA was conducted to examine the main effect of gender and time, as well as the interaction effect of gender and time, on depression symptoms. Depression showed a significant increasing trend across the four assessment times, F (3, 258) = 69.026, p < .001. Further paired t tests showed that depression symptoms at Time 1 were significantly higher than depression symptoms at Time 2, t (263) = 10.33, p < .001. Depression symptoms at Time 3 were significantly higher than depression symptoms at Time 2, t (263) = -12.07, p < .001. Depression symptoms at Time 4 were significantly higher than depression symptoms at Time 1, t (263) = -2.16, p = .032. Depression symptoms at Time 4 were significantly higher than depression symptoms at Time 2, t (263) = 12.08, p < .001. Gender had an insignificant effect on depression, F (1, 260) = 2.597, p = .108. The interaction effect of gender and time on depression symptoms was not significant, F (3, 258) = 1.279, p = .282.
Pearson’s correlation suggested that trait anxiety was significantly and positively associated with depression symptoms from Time one to Time two, r = .442 ∼ .683, p < .001. Higher trait anxiety was significantly related to poorer attentional control, as indicated by higher total attentional control scores, r = .548, p < .001. Total attentional control scores were significantly and positively associated with depression symptoms from Time 1 to Time 4, r = .360 ∼ .631, p < .001. Refer to Table 2 for the correlation coefficients
Table 2. Correlation among psychological variables
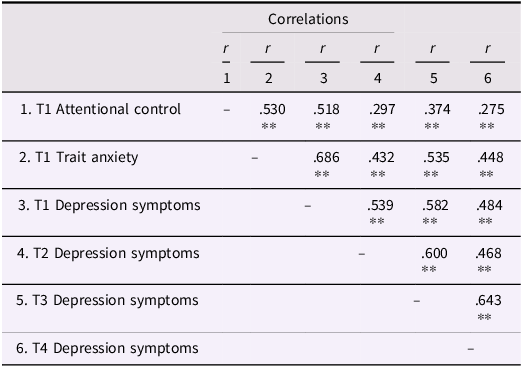
Note. T1 = Time one; T2 = Time two; T3 = Time three; T4 = Time four; **p < 0.001;
Correlations remain unchanged when controlling for gender.
Trajectories of depression symptoms
Unconditional model
Starting from the 2-class models, an increasing number of classes were tested until the VLMR, Adj. LMR, or BLRT showed that the k class model was not significantly better than the k-1 class model. Linear models were compared to nonlinear models. According to the fit indices for each model (refer to Table 3), the 4-class linear model had the lowest BIC and AIC values. VLMR, Adj. LMR, or BLRT were significant, showing that the 4-class model was significantly better than the 3-class model. Thus, the 4-class model was selected. The nonlinear model had better-fit indices than the linear model. Therefore, the 4-class nonlinear model was selected. Refer to S. Table 2 for growth parameters for each class of trajectories of depression symptoms (unconditional model).
Table 3. Fit statistics for latent class growth models representing two to four trajectory membership of depression symptoms (unconditional model)
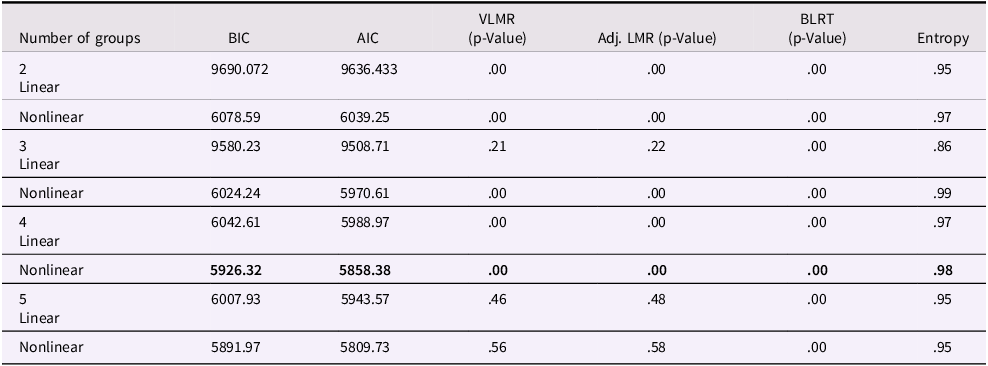
Note. The bolded four-group model showed the best model fit.
According to Figure 1, groups 1 to 3 exhibited a decrease from T1 to T2, which was followed by an increase in depression symptoms from T2 to T3. Group one was the “low depression” group, where depression symptoms remained relatively lower than the other group across the period (79.2%), Mean T1 depression = 3.52, Mean T2 depression = .48, Mean T3 depression = 3.72, Mean T4 depression = 4.57. The group showed a decrease from T1 to T2 and then gradually increased from T2 to T4 (mean intercept = 2.885, mean slope = -3.870, mean quadratic slope = 1.556). Group two was depicted as the “moderate depression” group, where the depression level was higher than that of the “low depression” group across the period (10.4%), with mean T1 depression = 9.27, mean T2 depression = 4.81, mean T3 depression = 9.77, and mean T4 depression = 9.19. The group showed a trajectory that increased from T1 to T2, decreased from T2 to T3, and gradually leveled off from T3 to T4 (mean intercept = 7.902, mean slope = −4.937, mean quadratic slope = 1.952). Group three was the “high depression group”, which showed a higher level of depression symptoms than the “low depression” and “moderate depression” groups. The level of depression symptoms decreased from T1 to T2, increased from T2 to T3, and decreased from T3 to T4 (mean intercept = 15.209, mean slope = 5.202, mean quadratic slope = −1.766), mean T1 depression = 12.63, mean T2 depression = 10.54, mean T3 depression = 12.83, mean T4 depression = 11.54. Group four was the “very high depression group”, which had the highest level of depression symptoms. Group four displayed a trajectory that increased from T1 to T2, decreased from T2 to T3 and leveled off from T3 to T4 (mean intercept = 12.114, mean slope = −2.179, mean quadratic slope = 0.742), mean T1 depression = 14.50, mean T2 depression = 18.75, mean T3 depression = 16.00, mean T4 depression = 15.75. Refer to S. Table 2 for the parameters in the supplementary information. The chi-square test showed that the trajectory membership of depression symptoms did not differ in terms of gender, χ2 (3) = 3.465, p = .325.
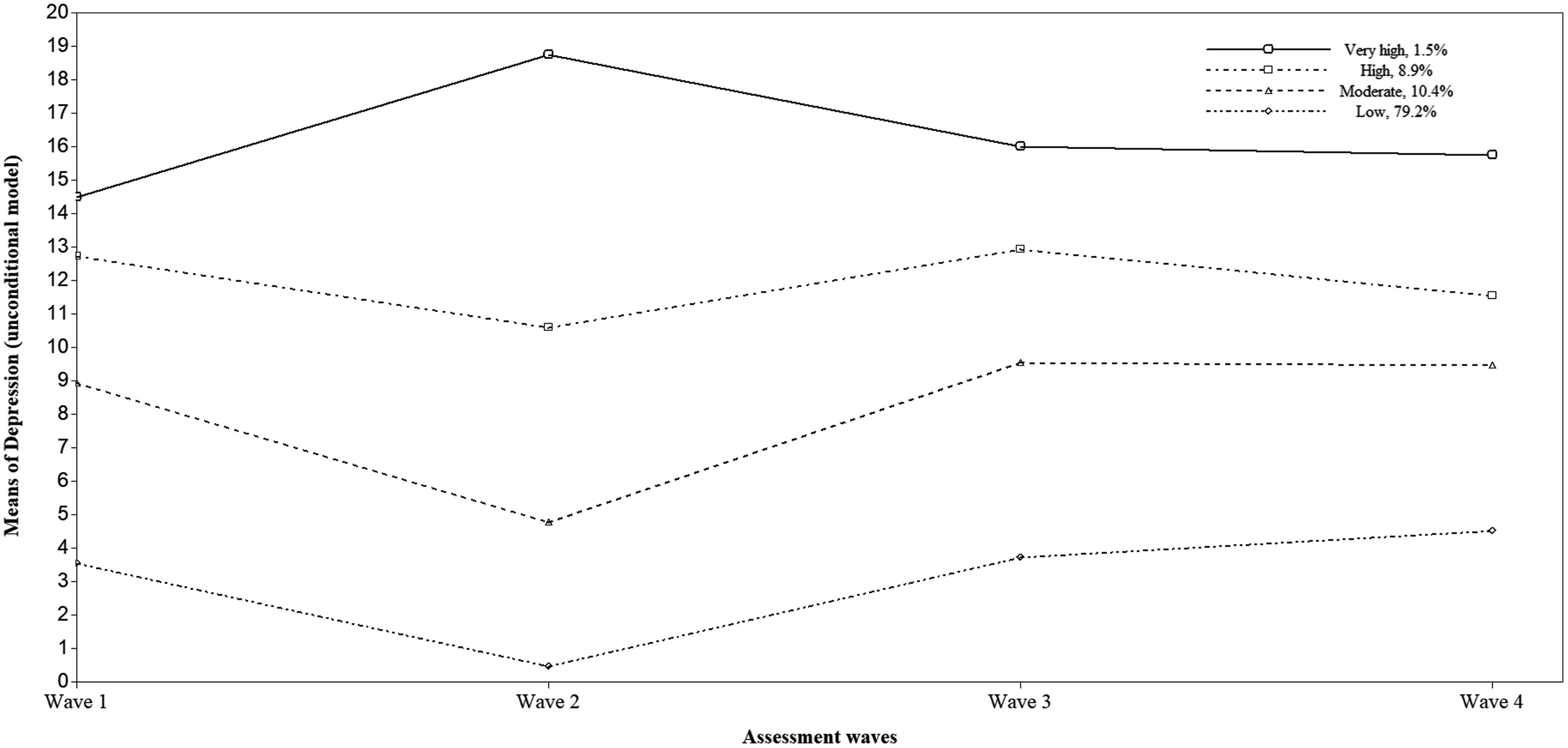
Figure 1. Unconditional model: heterogeneous trajectories of depression symptoms (Means). Note: Depression at T1: Variance = 29.842, Standard Deviation = 5.463; Depression at T2: Variance = 14.44, Standard Deviation = 3.801; Depression at T3: Variance = 28.850, Standard Deviation = 5.371; Depression at T4: Variance = 30.136, Standard Deviation = 5.490.
Conditional model
After including attentional control and trait anxiety into the model, LCGA revealed that the 2-class model showed the best model fit (refer to Table 4). Compared to the 3-class model, the 2-class model had the lowest BIC and AIC values. The 2-class model also had significant p values for VLMR, Adj. LMR, and BLRT tests indicated that the 2-class model was significantly better than the 1-class model. However, the 3-class model had insignificant p values for VLMR, Adj. LMR, and BLRT, suggesting that the 3-class model was not significantly better than the 2-class model. Compared to the linear model, the nonlinear model had better fit indices. Thus, the 2-class nonlinear model was selected. Refer to S. Table 3 for growth parameters for each class of trajectories of depression symptoms (conditional model).
Table 4. Fit statistics for latent class growth models representing two to four trajectory membership of depression symptoms (conditional model)
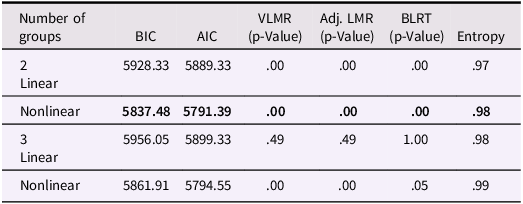
Note. The bolded two-group model showed the best model fit.
Refer to Figure 2. Class one was the “low depression” trajectory group (85.6%), which was characterized by a lower level of depression symptoms. The level of depression symptoms decreased from T1 (Mean depression = 3.67) to T2 (Mean depression = .80) and increased from T2 to T3. From T3 (mean depression = 3.94) to T4 (mean depression = 4.69), the level of depression symptoms slightly decreased (mean intercept = 3.109, mean slope =−3.260; mean quadratic slope = 1.350). Group two was defined as the “high depression” trajectory group, which consisted of 14.4% of the participants. The trajectory group had a high level of depression symptoms across the period. The level of depression symptoms in this group decreased from T1 (mean depression = 13.47) to T2 (mean depression = 9.84) and gradually increased from T2 (mean depression = 13.58) to T4 (mean depression = 12.61) (mean intercept = 12.371, mean slope = −3.136; mean quadratic slope = 1.180). Refer to S. Table 3 for the parameters in the supplementary information.
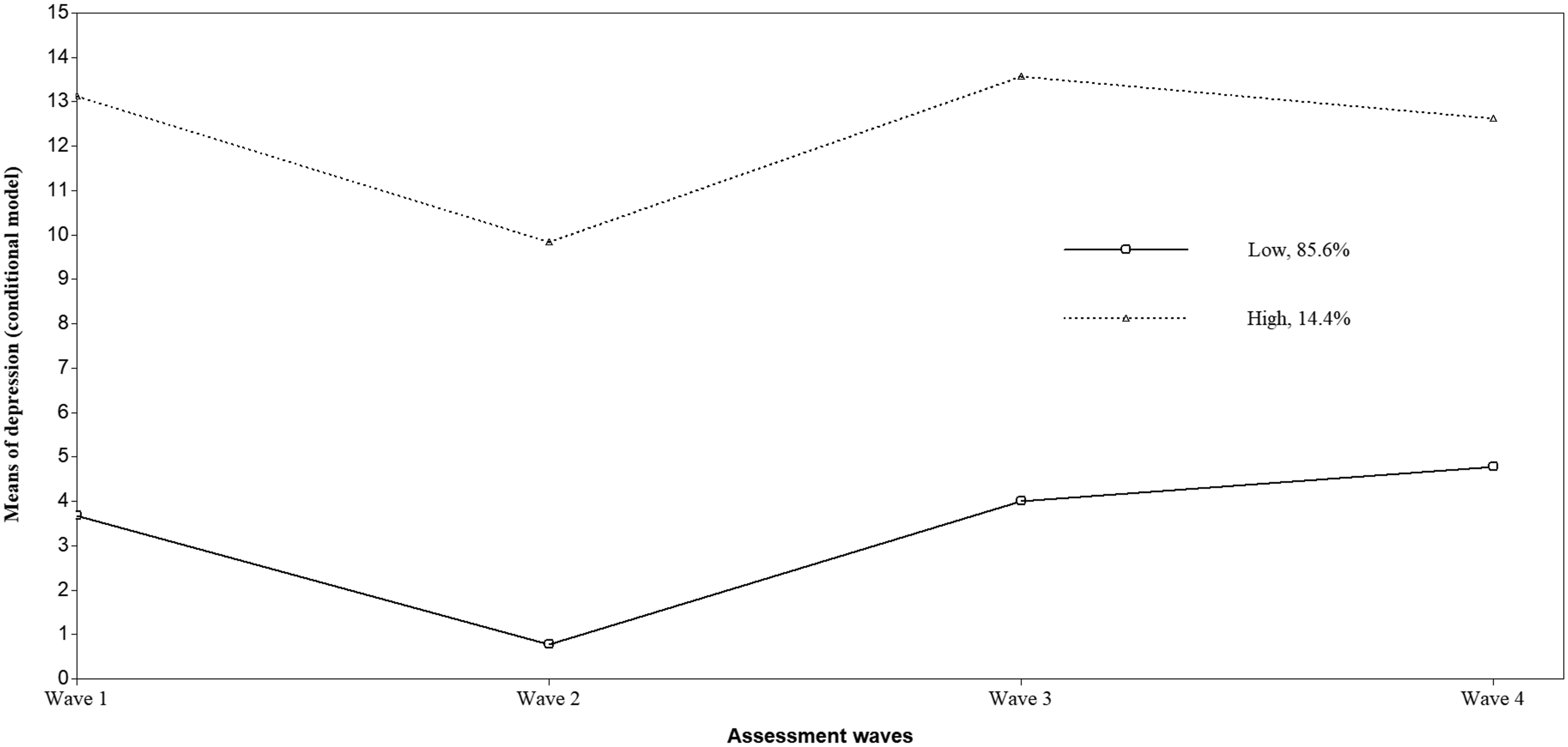
Figure 2. Conditoinal model: heterogeneous trajectories of depression symptoms (Means). Note: Depression at T1: Variance = 29.026, Standard Deviation = 5.388; Depression at T2: Variance = 14.527, Standard Deviation = 3.811; Depression at T3: Variance = 28.721, Standard Deviation = 5.359; Depression at T4: Variance = 29.969, Standard Deviation = 5.474.
Trait anxiety and attentional control as predictors of the trajectory of depression symptoms
Because the conditional model had a better model fit, the outcome of the conditional model was used in the analysis. With the trajectory membership of depression symptoms as the outcome variable, multinomial logistic regression was conducted to assess whether attentional control and trait anxiety at Time 1 were significant predictors of the trajectories of depression symptoms.
The regression model was significant, χ 2 (2) = 72.215, p < .001. Higher trait anxiety significantly predicted a higher probability of being in the “high depression” trajectory compared to the “low depression” trajectory (B = .140, SE = .030, p < .001, OR = 1.150, 95% confidence interval [CI: 1.085, 1.219]). Weaker attentional control, as indicated by higher total attentional control scores, significantly predicted a higher probability of being in the “high depression” trajectory than in the “low depression” trajectory (B = .102, SE = .036, p < .01, OR = 1.108, 95% confidence interval [CI: 1.032, 1.189]). Thus, consistent with the hypothesis, higher trait anxiety, and lower attentional control significantly predicted a higher likelihood of showing the high trajectory of high depression.
Mediation analysis
Multinomial logistic regression showed that the total effect of trait anxiety on the trajectory membership of depression symptoms, without considering the effect of attentional control, was significant (B = .174, SE = .028, p < .001, OR = 1.190, 95% confidence interval [CI: 1.128, 1.256]). Mediation analysis conducted with PROCESS v3.5 in SPSS showed that attentional control significantly and partially mediated the relationship of trait anxiety to the trajectory membership of depression symptoms. Refer to Figure. 3 for the mediational model. Higher trait anxiety significantly predicted higher total attentional control scores, t = 10.386, p < .001. Both trait anxiety, z = 4.689, p < .001, and attentional control, z = 2.827, p < .005, were significant predictors of the trajectory membership of depression symptoms; higher trait anxiety and higher total attentional control scores predicted a higher probability of showing the trajectory membership of high depression symptoms relative to the trajectory membership of low depression. Higher attentional control scores indicate poorer attentional control. The direct path from trait anxiety to the trajectory membership of depression symptoms was significant after accounting for the effect of attentional control (direct effect = 0.140, SE = 0.030, 95% CI = [0.081, 0.198], p < .001). The indirect effect of trait anxiety on the trajectory membership of depression via the partial mediator of attentional control was also significant (indirect effect = 0.038, SE = 0.014, 95% CI = [0.014, 0.071]). Thus, attentional control was a significant partial mediator of the relationship between trait anxiety and depression symptoms.
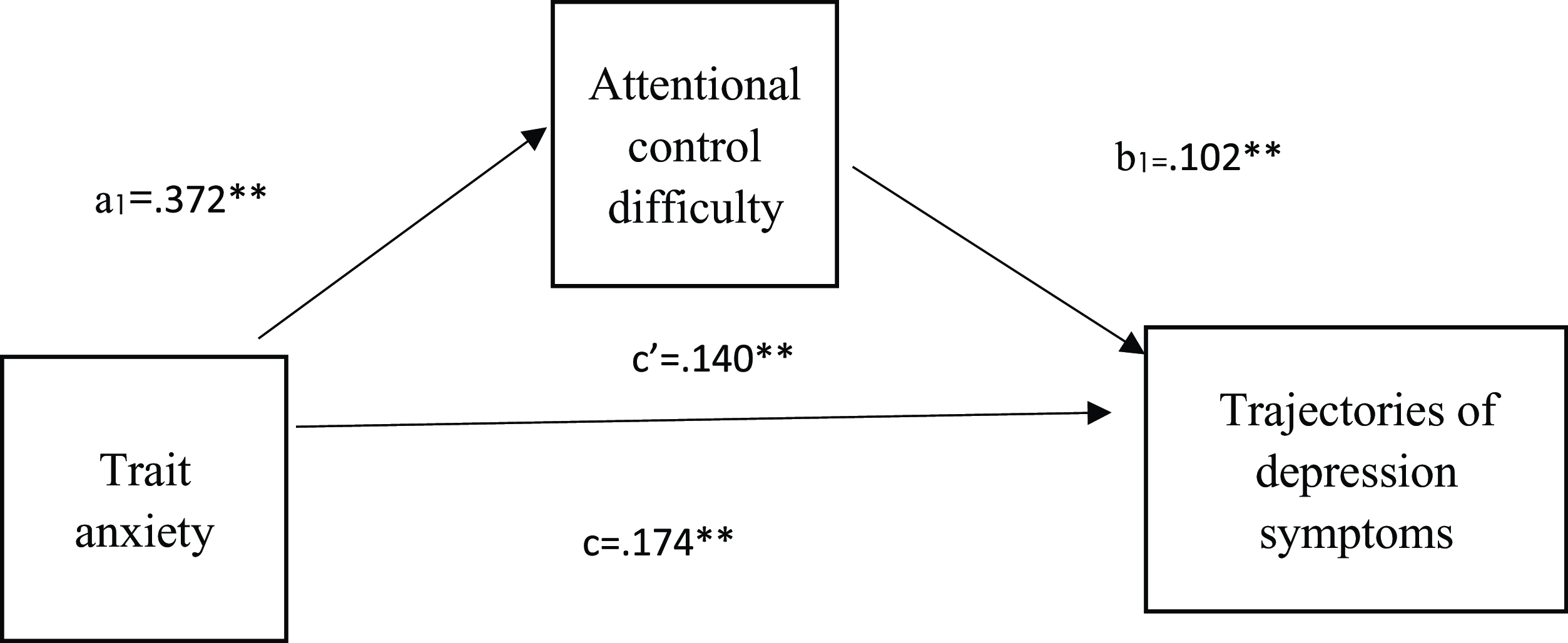
Figure 3. Mediation model with unstandardized coefficients: a1 = direct effect of trait anxiety on attentional control difficulty, b1 = direct effect of attentional control difficulty on trajectories of depression symptoms in children, c = total effect of trait anxiety on trajectories of depression symptoms in children, without accounting for the mediators. c' = direct effect of trait anxeity on trajectories of depression symptoms once mediators have been included in the model. **p < .001.
Discussion
The current study aimed to investigate the predictive value of attentional control and trait anxiety for the developmental trajectories of depression symptoms in children transitioning into adolescence. Additionally, the study aimed to examine the partial mediating effect of attentional control on the relationship of trait anxiety to the trajectory membership of depression symptoms. The study found that high attentional control predicted the trajectory of high depression symptoms. High trait anxiety predicted the trajectory of high depression symptoms. High attentional control significantly and partially mediated the relationship of trait anxiety to the trajectory membership of depression symptoms in children transitioning into adolescence.
Trajectories of depression symptoms
According to the RCADS User Guide, the raw scores were converted to t scores. T scores from 65 to 70 indicate borderline clinical levels of depression. For the trajectory of low depression symptoms, t scores ranged from approximately 30 to 41, indicating a low level of depression. For the trajectory of high depression symptoms for girls or boys from the 4th to 6th grades, the t scores ranged from approximately 51 to 69, indicating a borderline clinical level of depression. Thus, the majority (85.6%) of children demonstrated low depression levels during the transition into early adolescence. However, the minority (14.4%) of children had borderline clinical levels of depression.
Similarity with previous findings
Consistent with previous findings by Ezpeleta et al. (Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020) and Olivier et al. (Reference Olivier, Morin, Leo and Salmela-Aro2022), which revealed a low trajectory and a high trajectory of depression symptoms, the present study also identified two trajectories of depression symptoms during the transition into early adolescence, which comprised the trajectory of low depression symptoms (85.6%) and the trajectory of high depression symptoms (14.4%). Although the trajectories were not stable (decreased from T1 to T2 and increased from T2 to T3) across the transition into early adolescence, the general level of depression symptoms (low and high) remained constant across the period, which was consistent with previous studies (Ezpeleta et al., Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020; Olivier et al., Reference Olivier, Morin, Leo and Salmela-Aro2022).
Difference with previous findings
Contradictory to previous studies (Ezpeleta et al., Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020; Olivier et al., Reference Olivier, Morin, Leo and Salmela-Aro2022), the current study failed to reveal any increasing or moderate trajectory of depression symptoms after considering the effect of trait anxiety and attentional control. The sample only included children of 9 to 10 years, and the study lasted for 18 months, which might represent a critical but shorter assessment period. The assessment period in previous studies was longer; for example, the study by Ezpeleta et al. (Reference Ezpeleta, Penelo, Navarro, de la Osa and Trepat2020) had an assessment period of 5 years, and the study by Olivier et al. (Reference Olivier, Morin, Leo and Salmela-Aro2022) had an assessment period of 8 years. This might explain why fewer classes of depression trajectories were revealed in the current study than in previous studies.
Trait anxiety as the predictor for the trajectories of depression symptoms
Similarity with previous literature
Consistent with the hypothesis, trait anxiety was a significant predictor of the trajectory of depression symptoms during the transition into early adolescence. Previous studies have supported the transdiagnostic risk factor for trait anxiety for the development of depression symptoms (Carmela et al., Reference Carmela, Clara, Maria Rosaria Anna, Ivan, Clemente, Gianluca, Antonio and Antonio2022; Malhi et al., Reference Malhi, Das, Outhred, Bell, Gessler and Mannie2021 b; Moller et al., Reference Moller, Badcock, Hetrick, Rice, Berk, Witt, Chanen, Dean, Gao, Cotton and Davey2023; Wang et al., Reference Wang, Li, Xu, Liu, Wu, Lu, Xie, Peng and Wang2019 a). For example, a study with 178 depressive patients revealed that higher trait anxiety was associated with slower recovery from depression after treatment (Min et al., Reference Min, Lee, Lee, Lee and Chae2012). Consistent with previous studies, the current study added a developmental approach to the relationship of trait anxiety to the trajectory membership of depression and provided the first evidence that high trait anxiety predicted the trajectories of high depression symptoms during the transition into early adolescence. Transition into early adolescence is a period when children might encounter critical events such as puberty. The results showed that children with high trait anxiety were at greater risk of developing depression symptoms when they experienced negative events during the transition into early adolescence.
Theoretical explanation for the association between trait anxiety and depression
Symptoms trajectories
The relationship between trait anxiety and the trajectories of depression symptoms might be explained by the tripartite theory (Clark & Watson, Reference Clark and Watson1991). Based on the theory, depression and anxiety share the same component of general distress, which might account for the predictive value of trait anxiety for the trajectory of depression symptoms. Moreover, trait anxiety was related to a stronger tendency to allocate attention to negative information (Williams, Reference Williams1997). According to the cognitive theory proposed by Mogg and Bradley (Reference Mogg and Bradley2018), attentional bias contributes to the development of both anxiety and depression symptoms (Dong et al., Reference Dong, De Beuckelaer, Yu and Zhou2017; Dudeney et al., Reference Dudeney, Sharpe and Hunt2015). Cognitive theories explain why trait anxiety is related to the developmental trajectories of depression symptoms.
Attentional control predicting the trajectories of depression symptoms
During the transition into early adolescence, children were shown to have increased emotional arousal (Steinberg, Reference Steinberg2005). Children with poorer attentional control might have greater difficulty regulating their emotions, which increases their risk of developing emotional symptoms, including depression symptoms.
Similarity with previous literature
Consistent with the hypothesis, high attentional control deficits predicted trajectories of high depression symptoms. Consistent with previous research, poorer self-reported attentional control predicted higher depression symptoms during the transition into adolescence (Ólafsson et al., Reference Ólafsson, Smári, Guðmundsdóttir, Ólafsdóttir, Harðardóttir and Einarsson2011; Buckman et al., Reference Buckman, Saunders, Fearon, Leibowitz and Pilling2019; Sportel et al., Reference Sportel, Nauta, de Hullu and de Jong2013). Previous research has shown that poor attentional control is related to negative rumination over negative information and reduced self-efficacy, which are related to more depression symptoms in children (DeJong et al., Reference DeJong, Fox and Stein2019; Muris et al., Reference Muris, de Jong and Engelen2004). Findings from the present studies provided further evidence for the association between poor attentional control and depression symptoms.
The integrative cognitive model reveals that low attentional control results in enhanced attention toward negative information (Mogg & Bradley, Reference Mogg and Bradley2018). Higher negative attentional bias was related to higher depression symptoms (Hankin et al., Reference Hankin, Gibb, Abela and Flory2010). Therefore, the integrative cognitive model might provide an explanation for the present findings that high attentional control deficits predicted the trajectory of high depression symptoms.
The mediating effect of attentional control
Similarity with previous literature
Consistent with the hypothesis, attentional control had a partial mediating effect on the relationship of trait anxiety to the trajectory membership of depression symptoms. Trait anxiety contributed to the trajectory of depression symptoms via the partial mechanistic pathway of attentional control. The findings were congruent with previous studies that supported the negative association between trait anxiety and attentional control (Rezaei et al., Reference Rezaei, Hosseini Ramaghani and Fazio2017; Takil & Sari, Reference Takil and Sari2021). The findings were also convergent with previous evidence that high trait anxiety was related to poor attentional control, which contributed to reduced mindfulness (Walsh et al., Reference Walsh, Balint, Smolira Sj, Fredericksen and Madsen2009) Attentional control theory suggests that high trait anxiety weakens the ability to shift and inhibit attention, resulting in reduced cognitive effectiveness and efficiency (Eysenck & Derakshan, Reference Eysenck and Derakshan2011). The results of the mediation analysis were consistent with this theory, showing that higher trait anxiety predicted poorer attentional control.
The findings provided the first evidence to partially explain the relationship of trait anxiety to the developmental patterns of depression with attentional control. During the transition into early adolescence, children have higher emotional arousal and a higher likelihood of engaging in risky behavior (Steinberg, Reference Steinberg2005). Based on the results, children with high trait anxiety during this period might be more likely to feel anxiety, which negatively affects their attentional control ability. Congruent with previous findings, poorer attentional control, in turn, might lead to an increased tendency to ruminate over negative information (Hsu et al., Reference Hsu, Beard, Rifkin, Dillon, Pizzagalli and Björgvinsson2015) and stronger attention to negative stimuli (van Son et al., Reference van Son, Angelidis, Hagenaars, van der Does and Putman2018), which was related to a higher risk of developing depression symptoms during the transition into adolescence.
Difference with previous literature
A previous study showed that self-reported attentional control had a moderating effect on the association between trait anxiety and anxiety symptoms in adolescents (Ho et al., Reference Ho, Yeung and Mak2017a). Moreover, the study by Susa et al. (Reference Susa, Pitică, Benga and Miclea2012) showed that self-reported attentional control moderated the association between attentional biases and anxiety symptoms in children. In contradiction, the findings from the current study revealed the partial mediating role of self-reported attentional control in the association between trait anxiety and depression. This suggested that the role of self-reported attentional control was different in the association related to trait anxiety. When the association involves trait anxiety and emotional outcomes such as depression symptoms, self-reported attentional control was more likely to play the role of a partial mediator instead of a moderator.
Implications
The findings contributed to the developmental perspective toward attentional control theory to explain the development of depression symptoms. The developmental model showed that high trait anxiety was associated with poorer self-reported attentional control. Poor attentional control might contribute to and maintain the developmental patterns of high depression symptoms during the transition into early adolescence. The developmental model highlighted that attentional control might be one of the important cognitive mechanisms underlying the development of high depression symptoms in children with high trait anxiety.
Based on the developmental model, children with high trait anxiety were at high risk of developing the trajectory of high depression symptoms during the transition into early adolescence. Thus, early prevention might need to be delivered to children with high trait anxiety. Due to the partial mediating effect of attentional control, prevention that reduces self-reported attentional control might be important in preventing the development of high depression during the transition into early adolescence for at-risk children with high trait anxiety. Mindfulness training might affect attentional control, although its effect on attentional control measured by the Child version Attention Network Task (ANT) was limited (Lim & Qu, Reference Lim and Qu2017). Future studies might need to investigate whether mindfulness training affects self-reported attentional control and helps prevent children with high trait anxiety from developing the developmental trajectory of high depressive symptoms.
Overall, based on the current results, preventions or interventions for children with high trait anxiety should be developed because high trait anxiety predicted the trajectory of high depression during the transition into adolescence. Because of the partial mediating role of attentional control in the association between trait anxiety and the trajectory membership of depression symptoms, cognitive interventions or therapies targeting poor attentional control, such as attentional control training (Pettit et al., Reference Pettit, Rey, Marin, Bechor, Lebowitz, Vasey, Jaccard, Abend, Pine, Bar-Haim and Silverman2023), need to be delivered to children with high trait anxiety to improve attentional control and reduce the risk of developing high depression during the transition into adolescence (Teasdale et al., Reference Teasdale, Segal and Williams1995).
Limitations
The study had limitations that need to be taken into consideration when interpreting the results. Only Chinese children of 9–10 years at T1 transitioning into early adolescence were included in the study. Moreover, the study did not include children with a formal diagnosis of depression symptoms. Future studies need to be conducted in children with clinical levels of depression to investigate whether the results can be replicated. Thus, the generalizability of the findings might be limited. Additionally, the assessment period was 18 months, which might affect the results, especially the trajectories of depression. Therefore, it should be noted that the results might be different if the assessment period was longer and covered different developmental stages from childhood to adolescence. Another limitation lay in the self-report measure of attentional control and depression symptoms. Previous studies showed that experimental measures of attentional control, including the ANT (Van Bockstaele et al., Reference Van Bockstaele, Greenwell-Barnden, Todd, Clarke, MacLeod and Notebaert2023) or antisaccade task (Todd et al., Reference Todd, Notebaert and Clarke2022), had no relationship with self-reported attentional control. Attentional control measured by self-reported inventories might reflect personality traits related to attentional control or belief in attentional control ability (Olatunji et al., Reference Olatunji, Knowles and Cole2021). The antisaccade task or ANT might be more related to attentional control as a cognitive ability (Figueroa et al., Reference Figueroa, DeJong, Mocking, Fox, Rive, Schene, Stein and Ruhé2019; Lim & Qu, Reference Lim and Qu2017). Additionally, parents or other guardians may provide valuable information about children’s depression symptoms in daily life. However, the current study only collected data from children.
Future studies might need to investigate whether the results can be replicated with behavioral tasks. Future studies may involve other informants to measure depression symptoms. Future studies should replicate the findings with a larger sample of children from different age groups. Moreover, the assessment period could be longer to investigate whether trait anxiety and attentional control predicted developmental trajectories of depression over the developmental period from childhood to adolescence. Additionally, because attentional control was a partial mediator for the relationship between trait anxiety and trajectory membership of depression symptoms, future studies might need to investigate other potential mediators, such as attentional bias, for this relationship.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579424000385.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
Thanks to the teacher Ms. Xiao Hong Ling for her help in the research project.
Funding statement
The authors did not receive support from any organization for the submitted work.
Competing interests
The corresponding author states that there is no conflict of interest.
Ethical standard
Ethics approval was obtained from the Human Subjects Ethics Sub-Committee of the City University of Hong Kong (2020-21-CIR2-B1). Students’ parents who agreed their children to participate had signed the informed consent sheets and students had signed the assent sheets to participate.










 Open access
Open access