


During the past decades, non-communicable diseases have been the leading cause of mortality and morbidity worldwide. Developing countries emerged as epicenters of diabetes and other non-communicable diseases as a result of urbanization and nutritional transition (Chan et al., Reference Chan, Malik, Jia, Kadowaki, Yajnik, Yoon and Hu2009; Wang et al., Reference Wang, Kong, Wu, Bai and Burton2005; WHO, 1994). Non-communicable diseases account for an estimated 80% of annual deaths (Wang et al., Reference Wang, Kong, Wu, Bai and Burton2005) and 70% of total disability-adjusted life-years in China (‘China's major health challenge’, 2011). Studying the etiology and causes of non-communicable diseases can have significant impacts on disease prevention and treatment.
The Qingdao Twin Registry (QTR), established by Qingdao Centers for Disease Control and Prevention (QDCDC) in 1998, is part of the Chinese National Twin Registry (Li et al., Reference Li, Gao, Lv, Cao, Zhan, Yang and Hu2006). The purpose of the QTR was primarily to recruit twins born in the Qingdao region and to estimate genetic and environmental components in non-communicable diseases (Pang et al., Reference Pang, Ning, Unger, Johnson, Wang, Guo and Lee2006). A total of 10,655 twin pairs across all age groups were recruited until 2005 (Pang et al., Reference Pang, Ning, Unger, Johnson, Wang, Guo and Lee2006). The coverage of QTR has been extended and new cohorts were established during the past 5 years. Meanwhile, cross-culture collaborative studies between China, Denmark, Finland, and US cohorts have been carried out based on the QTR. This paper provides a detailed status update of the QTR.
Twins Recruitment
Since 2000, the QTR recruited twins through medical records, school, and media coverage (Pang et al., Reference Pang, Bo, Wang, Peng, Zhang and Zhai2003, Reference Pang, Ning, Unger, Johnson, Wang, Guo and Lee2006). Newborn twins were identified and recruited to QTR through the Immunization Registry for Newborns, which covers 95% of all newborns in Qingdao each year. Children and adolescent twins are registered and their health and development monitored by school physicians and nurses. The tertiary prevention and health system (village, township, and county level) in Qingdao has provided assistance for the registries with high efficiency, coverage, and accuracy of information (Li et al., Reference Li, Gao, Lv, Cao, Zhan, Yang and Hu2006). The twin registry and health-related surveys have been reviewed and approved by the QDCDC ethics committee and collaborative institutions’ ethics committees.
Anthropometric Measurements
Trained physicians or nurses explained the objectives of the survey and obtained consent from twins and their families. Height and weight were measured with participants wearing light clothes and without shoes. Waist circumference was measured at the midpoint between the rib cage and the iliac crest to the nearest 0.1 cm. Hip circumference was measured over the widest part of the gluteal region to the nearest centimeter. Body mass index (BMI) was defined as an individual's body weight in kilograms divided by the square of his/her height in meters (kg/m2). Blood pressure was taken by a standard procedure using mercurial table stand model sphygmomanometer. Systolic blood pressure was defined as Korotkoff of phase I (appearance of sound), and diastolic blood pressure was defined as Korotkoff phase V (disappearance of sound) (Ren et al., Reference Ren, Wu, Hu, Cao, Zhan, Lv and Li2003). After undergoing the anthropometric measurements, adult twins, adolescent twins, and their parents were requested to fill in the health-related questionnaires, which included questions on substance use, mental health status of the twins, as well as socio-economic characteristics of the families.
Laboratory Tests
After an overnight fast of 10–12 hours, twins were invited to the health screening centers of the local Center of Disease Control. Blood samples of approximately 10 mL were collected from the antecubital vein into a vacuum tube containing sodium fluoride. Centrifugation and separation of serum and plasma from blood cells were performed at the local centers within 30 minutes of collection. Fasting plasma glucose was determined using the glucose oxidase method. Total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and other biomedical parameters were measured using the Analyser Medical System (Olympus-AU 640 Automatic analyzers, Olympus Optical, Tokyo, Japan).
A standard 75 g oral glucose tolerance test was carried out in the adult twins. Participants with a history of diabetes or a fasting plasma glucose ≥7.0 mmol/L or a 2-hour plasma glucose ≥11.1 mmol/L, were classified as diabetic according to the World Health Organization criteria 1999 (Alberti & Zimmet, Reference Alberti and Zimmet1998). Another 5 mL venous blood sample was collected and stored for the DNA test.
Zygosity Determination
For zygosity determination, first we identified potential monozygotic (MZ) and dizygotic (DZ) twins through sex and ABO blood types. Twins with opposite sex and/or different blood types were classified to DZ twins. Zygosity determination of twin pairs with same sex and blood types was classified by DNA testing using 16 short tandem repeat markers (Becker et al., Reference Becker, Busjahn, Faulhaber, Bahring, Robertson, Schuster and Luft1997; Jackson et al., Reference Jackson, Snieder, Davis and Treiber2001). Zygosity tests were conducted in the central laboratory of the Qingdao Blood Station.
Development of the Adolescent Twin Cohort and the Research Focus
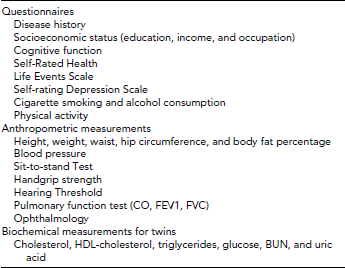
Six young twin cohorts (born 1990–1996) including a total of 600 pairs were established in 2006. The first phase of the young twin study was completed when these twins were 10–16 years old in 2006. The two follow-up surveys took place in 2007–2008 and in 2009 when twins were 11–18 and 13–19 years old, respectively. Follow-up rates were 98% in 2007–2008 and 95% in 2009. The questionnaires and anthropometric measurements were described in details as below (see Table 1).
TABLE 1 Phenotypes of Twin Pairs for the Adolescents’ Cohort

CO, carbon monoxide; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; BUN, blood urea nitrogen.
Abnormal lipid metabolism contributes to atherosclerosis, cardiovascular diseases (Zhang et al., Reference Zhang, Qiao, Tuomilehto, Hammar, Ruotolo and Stehouwer2009), and diabetes (Mooradian, Reference Mooradian2009) and lipid metabolism in adolescence is predictive for these conditions. Data from the QTR, including 314 same-sex twin pairs (MZ = 243, DZ = 71) aged 5–18 years, indicated that lipid levels were significantly different before and after puberty (Chen et al., Reference Chen, Ji and Hu2009). Moderate and strong heritability estimates were observed for lipid phenotypes, such as TC, HDL-C, and low-density lipoprotein cholesterol (LDL-C), whereas TG was influenced mainly by shared and non-shared environmental factors. Total phenotypic variances decreased after puberty, mainly as a result of decrease of genetic variance, even though the common environmental variance increased. Shared environmental factors had an important effect on lipids during puberty, suggesting family-based lifestyle intervention might be recommended in reducing cardiovascular risk factors. To what extent the variances change might be caused by sex and growth hormones or genetic-environmental interactions during puberty (Frindik, Reference Frindik, Kemp and Sy1999; Rogol, Reference Rogol, Roemmich and Clark2002), needs to be investigated in a longitudinal study.
Hyperuricemia, defined as a serum uric acid concentration in excess of urate solubility (Fang & Alderman, Reference Fang and Alderman2000), increases the risk for diabetes and cardiovascular disease in adults. Accumulated evidence has demonstrated that hyperuricemia is associated with metabolic syndrome in child and adolescent Caucasians (Ford et al., Reference Ford, Li, Cook and Choi2007; Invitti et al., Reference Invitti, Maffeis, Gilardini, Pontiggia, Mazzilli, Girola and Viberti2006; Lee et al., Reference Lee, Wahlqvist, Yu and Pan2007; Pacifico et al., Reference Pacifico, Cantisani, Anania, Bonaiuto, Martino, Pascone and Chiesa2009; Tang et al., Reference Tang, Kubota, Nagai, Mamemoto and Tokuda2010), but not in their Chinese counterparts. Our data, including 521 twin pairs from the 2006 baseline survey (MZ = 274, DZ = 247), demonstrated that genetic factors play a vital role in uric acid metabolism. A sex-limitation model showed that additive genetic factors accounted for 75% of total variance, while non-shared environmental factors explained 22.5% (Duan et al., Reference Duan, Pang, Zhang, Wang, Zhai and Zhang2010). The combined effects of pubertal development, sex hormones, and obesity on uric acid levels need to be further investigated.
Skeletal age is usually employed to evaluate endocrine, genetic, and renal disorders and to monitor growth in childhood and adolescence (Poznanski, Reference Poznanski1984; Tanner et al., Reference Tanner, Whitehouse and Marshall1975). The skeletal or bone age determination evaluates left hand and wrist from subjects at different stages of skeletal maturation using radiologic examinations (Greulich, Reference Greulich and Pyle1959). Inconsistency between skeletal age and chronological age suggest metabolic disorders on the endocrinology and anthropology vary across the ethnic groups (Mora et al., Reference Mora, Boechat, Pietka, Huang and Gilsanz2001). During 2012–2013, a total of 190 pairs of adolescent twins from the QTR will have hand and wrist radiographs taken by experienced pediatric radiologists. The Standards of Skeletal Maturity of Hand and Wrist questionnaire (Version 2005) using measurements derived from Chinese children will be employed to determine maturation and subsequent evaluation of growth during puberty. The heritability of skeletal age and corresponding risk factors will be estimated in a sex limitation model. Whether the difference between skeletal age and chronological age is explained by genetic or environmental effects, such as sex hormone and lifestyle, will be assessed and compared with other ethnic groups.
Chinese–US Adolescents Twin Study of Substance Use
Cigarette smoking has been identified as the second leading risk factor for death from any cause worldwide (Gu et al., Reference Gu, Kelly, Wu, Chen, Samet, Huang and He2009). China is the world's largest producer and consumer of tobacco and bears a large proportion of deaths attributable to smoking worldwide. In 2010, a cross-sectional survey indicated that 28.1% of adults were current smokers, accounting for 301 million people in China (Li et al., Reference Li, Hsia and Yang2011). Odds ratio (OR) for past 30-day smoking is significantly higher in adolescents in the United States than Chinese counterparts in a multivariable adjusted model, with an OR of 0.80 (0.71–0.90; Unger et al., Reference Unger, Yan, Shakib, Rohrbach, Chen, Qian and Anderson Johnson2002). The association between access to cigarette and respondents’ smoking were significantly greater in US adolescents. Family and peer influence play an important role on adolescent substance use (Trinidad et al., Reference Trinidad, Chou, Unger, Johnson and Li2003; Unger et al., Reference Unger, Yan, Shakib, Rohrbach, Chen, Qian and Anderson Johnson2002; Zhu et al., Reference Zhu, Liu, Wang, He, Chen, Shi and Shang1992). Most psychological and genetic studies of adolescent substance use have been conducted within a single cultural context; however, it is not known whether the complex interactions among genetic risk/protective factors and social-environmental risk/protective factors differ across cultural contexts. Cross-cultural study could add to our knowledge about the socio-cultural conditions that increase or decrease the effects of risk and protective factors.
For this purpose, we initiated a cross-cultural study between China and the US adolescent twins based on 600 twin pairs (born between 1990 and 1996) in China and 600 twin pairs of the same age range selected from the twin study of University of Southern California in the United States. We collected psychosocial data to distinguish environmental risk and protective factors from heritable factors in order to identify the specific aspects of the shared and non-shared environments that are associated with substance use, and to investigate interactions and mediated pathways among these influences. Furthermore, the impact of parents and peers attitudes and behaviors on adolescents substance use will be investigated in this study.
Preliminary outcomes from the QTR cohort indicated that the estimates heritability for alcohol consumption is greater than for cigarette smoking (0.68 vs. 0.28), whereas environmental factors account for major components of total variances of psychological traits (depression, aggression, and hostility) among adolescents. Bivariate analysis showed that substance use and psychological measures were attributed to the combined effects of genetic and environmental factors (Unger et al., Reference Unger, Lessov-Schlaggar, Pang, Guo, Ning, Gallaher and Anderson Johnson2011). Family environment and peer behaviors were further investigated to explore the risk and protective factors for substance use in QTR. Family cohesion, family adaptability, parental monitoring, and academic score were associated with decreased risk for smoking, whereas negative events (e.g., family-related, school-related, and peer smoking) increased the odds for cigarette smoking in adolescents (Arpawong et al., Reference Arpawong, Sun, Chang, Gallaher, Pang, Guo and Unger2010). Whether the association between risk and protective factors is culture specific warrants further investigations.
The Development of Adult Twin Survey and the Research Focus
A total of 695 pairs of adult twins (MZ = 405, DZ = 290) with a mean age of 37 years were recruited in this study. Anthropometric measurements of metabolic phenotypes were collected from these twins in 2001, and were followed up in 2004 and 2008. Genetic factors play vital roles in the sub-phenotypes of metabolic syndrome; however, no common genetic mechanism interacts among the phenotypes based on the bivariate analyses (Duan et al., Reference Duan, Pang, Zhang, Li, Kruse, Kyvik and Tan2011). Multivariate analysis of lipid parameters explored the common genetic architecture in the development of these phenotypes. The findings revealed common genetic and environmental backgrounds for lipid phenotypes, that is, TC, HDL-C, and LDL-C. Modeling showed that physiologically distinct endophenotypes may follow different genetic regulations (Pang et al., Reference Pang, Zhang, Li, Duan, Hjelmborg, Kruse and Tan2010). To determine which loci affect lipid phenotypes in Chinese populations, genome-wide association analysis is warranted.
To our knowledge, we were the first to perform a genome-wide linkage scan on BMI using twins in the Chinese population. The strong linkage identified in Chinese subjects comparable with European studies suggests the existence of evolutionarily conserved genetic mechanisms for BMI, whereas the multiple suggestive loci could represent a genetic effect from gene-environment interaction as a result of population-specific environmental adaptation (Zhang et al., Reference Zhang, Pang, Li, Jiang, Wang, Thomassen and Tan2012a). Our genome-wide association analysis in DZ twins detected a suggestive association on chromosome 4 (rs17031508, p < 8, 34E-08) located within a wide region of suggestive linkage. Our results provide some evidence for genetic linkage and associations with pulse pressure in the Chinese population. Further investigation is warranted to replicate the findings and to explore the susceptibility loci or genes for pulse pressure (Zhang et al., Reference Zhang, Pang, Li, Thomassen, Wang, Jiang and Tan2012b). Considering the limited sample size, validity of these loci requires additional replication studies to be conducted, particularly in the Chinese and other Asian populations. Moreover, the long-term effects of genetic and environmental risk factors for cardiovascular diseases will also be evaluated in a follow-up study.
The Development of Chinese–Finland Adolescents Twin Cohort Study and the Research Focus
It is generally believed that genetic predisposition is important in the risk of disease, whereas lifestyle and environmental factors are assumed to trigger or modify the expression. It has been hypothesized that ethnic differences may result in varying susceptibility to diseases. For example, the risk of type 2 diabetes is 13.5 times greater in Asian children than in White children (Drake et al., Reference Drake, Smith, Betts, Crowne and Shield2002), while the incidence of type 1 diabetes is about 30 times higher in Finland than in China (LaPorte et al., Reference LaPorte, Tajima, Akerblom, Berlin, Brosseau, Christy and Neil1985; Yang et al., Reference Yang, Wang, Li, Sun, Li, Chang and LaPorte1998). Asthma is one of the most common atopic diseases in developed countries; however, the rates of asthma and allergy are relatively lower in Chinese children (Warner, Reference Warner1999; Williams et al., Reference Williams, Robertson, Stewart, Ait-Khaled, Anabwani, Anderson and Weiland1999; Beasley, Reference Beasley1998). Genetic and environmental diversity, diet, substance use, and psychology might explain the regional variations. To what extent the differences in culture and lifestyle have contributed to the variations between Chinese and Finnish adolescents are less known. Twin studies should provide unique insights into how genetic and environmental factors influence obesity and other metabolic disorders during urbanization and lifestyle transition in Chinese adolescents, and how comparable are the variance component estimates to those in Finnish counterparts.
We will collect data from 600 Chinese adolescent twins in a cohort established in 2006 when the pairs were 10–16 years old, and the data will be compared with 1,000 adolescent Finnish twin pairs at the same age. The specific aims of this study are: (1) to study interactions between genetic factors, social environment (e.g., parental and peer influences, stressful life events), and lifestyle (e.g., physical activity, cigarette smoking, and alcohol drinking) in the prediction of adolescent obesity and metabolic disorders in Chinese and Finnish adolescents; and (2) to assess mediated pathways by which heritable factors influence adolescents’ selection of social environments, thereby influencing their exposure to social-environmental risk factors for obesity and metabolic disorders, making adolescents more susceptible or resilient to health consequences under different cultural contexts.
Development of Elderly Twin Cohort and the Research Focus
Cross-sectional and longitudinal studies have shown that aging-related decline in physical performance and increasing functional impairment is associated with detrimental outcomes in the elderly, such as disability, decline in quality of life, and mortality. People over 60 years old account for 13.3% of the population in China. A collaborative study including 2,476 adults aged 50–74 years from the Qingdao China Ageing Study (Wu et al., Reference Wu, Pang, Zhang, Jiang, Wang, Li and Tan2012a, Reference Wu, Zhang, Pang, Oksuzyan, Jiang, Wang and Tan2012b) and 5,278 twins aged 50–74 years from the Study of Middle-Aged Danish Twins and the Longitudinal Study of Aging Danish Twins, demonstrated significant gender and population differences in physical, cognitive performance and mental assessment (Wu et al. Reference Wu, Pang, Zhang, Jiang, Wang, Li and Tan2012a, Reference Wu, Zhang, Pang, Oksuzyan, Jiang, Wang and Tan2012b). Age-related decline in general health was observed in both ethnic groups. However, genetic and environmental factors cannot be evaluated in the general population using the Chinese cohort.
To provide valuable information for decomposition of the genetic and environmental determinants in the observed differences in the two ethnic groups, we launched an elderly twin cohort in Qingdao. The protocol of elderly twin study is consistent with the Qingdao China Ageing Study (Wu et al. Reference Wu, Pang, Zhang, Jiang, Wang, Li and Tan2012a, Reference Wu, Zhang, Pang, Oksuzyan, Jiang, Wang and Tan2012b). As shown in Table 2, physical performance, such as sit-to-stand test (lower limb strength measurement), handgrip strength, cognitive performance, and depression were evaluated in these elderly twins. The scale of the Mini-mental Cognitive state (Folstein et al., Reference Folstein, Folstein and McHugh1975) and the Zung Self-Rating Depression employed in the current study have been validated widely (Zung, Reference Zung1965).
TABLE 2 Phenotypes of Twin Pairs for the Elder Cohort
We plan to collect 300 pairs of twin aged 40 years and over to evaluate the genetic and environmental risk factors for aging-related diseases. The aims of the elderly twin study are: (1) to estimate the heritability of aging-related phenotypes, and promote the well-being through environmental modifications; and (2) to explore the aging susceptible genes with the extensive genome-wide association studies.
Furthermore, we plan to conduct a longitudinal study in the adult and elderly twin cohorts. Meanwhile, together with the Qingdao Death Registry and Qingdao Health Record Registry, we monitor the incidence of diabetes, cancer, and other non-communicable diseases and lifestyle changes in Qingdao twins. An investigation of the joint effect of genetic and environmental risk factors on the increasing trends of metabolic disorders, mortality, and morbidity will be conducted in further investigations.
Acknowledgments
The authors wish to thank the QDCDC twin project staff for assistance in data collection, and the twins and their families for their participation in this research. The QTR was supported by the China Medical Board, New York (CMB01-746). Additional support for expanding the twin registry was provided by the National Institutes of Health (P50 CA84735-01), Novo Nordisk Foundation Grant for Medical Research (2006), European Foundation for the Study of Diabetes (2007), and National Natural Science Foundation of China (30872170). FN also received financial support from European Foundation for the Study of Diabetes/Chinese Diabetes Society/Lilly Research Fellowships (2009).


