


Introduction
In 1703, the Académie royale des sciences in Paris reported the case of a 23-year-old man from Chartres. He had been deaf and mute his entire life, until 1 day – to the surprise of the entire city – he suddenly started to talk. The French surgeon Claude-Nicolas Le Cat (1700–68) recalled this remarkable story in his 1742 treatise on the senses, noting that the man ‘gave out, that 4 or 5 months before, he had heard the sound of bells and was exceedingly surprised at this new sensation. After this a kind of water gushed from his left ear, and he heard perfectly well with both’.Footnote 1 In the months following that occurrence, the man continued his normal routines, including attending church, but privately he practiced uttering words until he ultimately broke the silence. Remarkably, this story was not reported as a case of miraculous healing, which had not been uncommon in medieval and early modern Europe.Footnote 2 Rather, in Le Cat’s retelling the man’s transition from deaf to hearing had coincided with the secretion of excess fluid stuck in his ears. Scottish writer Martin Martin (d. 1718) reported a similar incidence about Daniel Fraser from Straharig near Inverness, who was congenitally deaf. At seventeen, after having recovered from a violent fever, he ‘perceived a motion in his brain, which was very uneasie [sic] to him, and afterwards he began to hear’.Footnote 3 These case studies raised the question about the role of the fluids in deafness and hearing.
This article discusses how physicians across Europe became increasingly interested in differences between how well people could hear from the late seventeenth century onwards. They conducted numerous studies on the ear and hearing to better understand deafness and hardness of hearing – two terms often used interchangeably. Medical men recognised that hearing difference came in numerous shapes and guises, and that it could be caused by various circumstances, including disease, accident or old age. Yet, in medical treatises, all these diverse forms of hearing difference fell under the same rubric of ‘deafness’.Footnote 4 This made deafness not necessarily a single and fixed physical state, but rather a flexible condition that could slowly or suddenly manifest itself, and just as easily disappear or remain permanent. This article analyses how early modern physicians explored the crucial role of earwax and other fluids as conducive to hearing and, inversely, as responsible for bringing about deafness. It argues that this new medical understanding of a fluid auditory perception cast hearing and deafness not as dichotomous but rather as part of a broad, continuous spectrum.
It is important to note that by using the term ‘continuous spectrum’, I do not refer to the advent of audiometry in the late nineteenth century, which framed hearing and deafness via the standardised measurement of the range and sensitivity of a person’s sense of hearing.Footnote 5 Rather, I call attention to the early modern recognition that the condition of deafness was flexible. Deafness was not a fixed state or condition, but showed many changes on an individual and societal level. For some people, the impairment of deafness was permanent and profound, as was often the case in the congenitally deaf – although educators realised that their condition did not necessarily imply functional limitation. Within the field of medicine, too, the condition of deafness was considered as a ‘fluid state’.Footnote 6 The movement and consistency of fluids that occur in and across the body was the main explanation for understanding how the body worked. Physicians conceived of physiology and pathology in terms of fluids by combining ancient humoral theory with iatromechanical and iatrochemical thinking. The fluids went across bodily boundaries and included flows through the skin and filtrations from the air. The onset of deafness could imply the viscosity or blockage, and hence medical interventions were aimed at applying the right type of fluid to make solids in the hard of hearing, fluid again. Fluid deafness, in short, applied to the flexibility in hearing difference as well as its conception interpreted in terms of fluids.
The present article begins with a discussion of the historiography of deafness, which tends to discuss deafness in terms of permanence and dichotomies. The three sections that follow demonstrate the notion of fluid deafness in three distinct ways. The first section focuses on the characteristics of earwax and the unstable divide between hearing and deafness. The fluidity of earwax was believed to be conducive to hearing, while its viscosity and obstruction in the ear channel were thought to cause severe hearing difficulties, including tinnitus and partial deafness. The application of the right type of fluid, physicians argued, would liquify solid earwax. The second section explores the notion of subtle fluids of sound and hearing: physicians envisioned the vibrations and movement of sound as fluids, both in the air and in the inner ear and nervous system. The final section examines how new medical interventions, such as injecting the Eustachian tubes, aimed at making deafness temporary rather than permanent. Treatments for hearing difficulties often involved the syringing with liquids to help excrete fixed pus and mucus. Ultimately, the study and treatment of deafness in the early modern world drives home the point that there existed no solid dividing line between deaf and hearing; if anything, the divide was permeable and unstable.
Histories of deafness and medicine
Scholarship on deafness has often described deafness in terms of permanence and in opposition to hearing. Studies on early modern deafness take a social approach and focus almost exclusively on the study and education of congenitally deaf children: they were either born deaf or became deaf at a very young age, and hence did not speak.Footnote 7 Within histories of deaf education, scholars have distinguished two central philosophies, both of which suggested the somatic state of deafness as permanent. One philosophy propagated an oralist approach, aimed at teaching children to speak and speech-read.Footnote 8 The other regarded sign language as the natural language of the deaf and hence promoted a manual approach, teaching deaf children sign language.Footnote 9 Eighteenth and nineteenth century educators therefore perceived profound deafness as something that could be transcended through language and speech training. Historians have fruitfully analysed the extent to which both philosophies succeeded in improving the functional limitations of deafness, not only showing how schools for deaf children fostered the development of a Deaf community and Deaf culture but also how former pupils managed to get along remarkably well in a hearing society.Footnote 10
However, because scholars have generally refrained from questioning the somatic concept of deafness as a historical category, they have unwittingly reinforced the presumed permanent status of ‘deaf’ and the conventional deaf/not deaf assumption.Footnote 11 Instead, this article takes its cue from recent work arguing that the D/deaf distinction is artificial – since 1975 used to denote the difference between those who are culturally deaf and the audiological condition deaf – and does not reflect how deaf individuals may identify, nor how medical professionals leverage this distinction for diagnosis purposes.Footnote 12 Indeed, the early modern medical term ‘deafness’ denoted a wide range of phenomena that are nowadays labelled congenital and prelingual deafness as well as conductive and sensorineural hearing loss. Physicians and surgeons elaborated upon the exact experiences of the case in question, which could include tinnitus, earaches, swellings and a range of other observations. By historicising the medical term of deafness, then, this article takes hearing difference as its object of study.
Recent studies on deafness and hearing loss in the modern age have shown that both were increasingly perceived as pathological and in need of a cure, again pitting hearing and deafness as opposites. Analysing medical and scientific developments in the nineteenth and twentieth centuries, historians have charted the role of medics in making ‘hearing’ the normative category. While the aim of medics and oralists was to have deaf people assimilate in the hearing society, this simultaneously legitimised the need for medical intervention. In the course of the nineteenth century, doctors increasingly supplanted teachers at schools for the deaf, and aural surgery emerged as a new specialisation.Footnote 13 At the turn of the twentieth century, otologists shifted their objective from curing deafness to assisting hard of hearing adults with communication barriers. Yet in doing so, hearing loss became defined as an impairment in audiometry and hearing tests, which only served to solidify the perception of deafness as a pathological problem.Footnote 14
While the measurement of auditory acuity significantly impacted how hearing loss came to be defined, the study of deafness in science and medicine should not be limited to the modern period. This article contends that early modern medicine provides an important insight into notions and attitudes of deafness, as it presents an alternative approach to deafness, before the strict divide between hearing and deafness took shape. Exploring a wide variety of medical sources, including philosophical and medical treatises, dissertations, textbooks and encyclopaedia entries, this article shows that, in contrast to the modern notion of deafness as a biological reality, early modern physicians understood deafness as a fluid concept, and as the result of an interaction between neo-humoral bodies and their atmospheric environment. To be sure, as in other ages, some early modern physicians expressed unmistakably ableist and audist views concerning the so-called ‘deaf and dumb’. Overall, however, the eighteenth century presented a medical perception of deafness that considered hearing and deafness to have natural and fluid boundaries. By historicising the medical term of deaf in the eighteenth century, this article reveals a much more fluid and permeable understanding of the condition, which extended beyond a diversity in deafness and included hearing as well.
While numerous people in early modern Europe experienced some form of hearing difference – either from birth, by accident, disease, or old age – most scholarship on this period has focused on the conceptions of the body and the senses. Medical historians have written about such topics as anatomy, the physiology of the nerves, and the role of music in well-being, but deafness has largely been neglected.Footnote 15 This article therefore contributes to the current historiography by demonstrating the growing interest in deafness by physicians and surgeons. The isolation of the elementary substances and chemical properties of bodily fluids, which was dominant at the time, also initiated new ideas about sound, hearing and deafness.Footnote 16 Medical studies therefore included ear anatomy, hearing physiology, defects of the ear, earwax varieties, the design and effectiveness of hearing aids, speech therapy and gesture communication. By analysing deafness in an early modern medical context, this article offers a new perspective on both medical discourses of deafness and the concerns and abilities of physicians in this period.
Earwax viscosity
The case of earwax is a clear example of the unstable divide between hearing and deafness in early modern medicine. Earwax, known to physicians by the medical term cerumen (from the Latin cera, meaning ‘wax’), was not simply a waxy substance secreted in human ear canals. Across Europe, medical writings referred to transparent and yellow, oily and bitter, smooth, viscid and dry earwax, in excessive or diminutive quantities. Physicians agreed that the quantity and quality of earwax resonated with both healthy and bad hearing. From the late seventeenth century onwards, therefore, earwax became one of the most important explanations for the occurrence of hearing difference, because its many different manifestations allowed physicians to dissolve the boundaries between hearing and deafness.
One of the first to elaborately describe the particulars of earwax was the French physician and anatomist Guichard Joseph du Verney (1648–1730), a member of the Académie royale in Paris who gave regular anatomical demonstrations.Footnote 17 In 1683, he published the Traité de l’organe de l’ouie (translated in 1737 as A Treatise of the Organ of Hearing), which discusses the anatomical structure of the ear, the physiology of hearing and ear diseases.Footnote 18 He was not the first to publish on the anatomy of the ear though: almost two centuries earlier (in 1543), Andreas Vesalius (1514–64) had already depicted two of the three small bones from the middle ear in his revolutionary De humani corporis fabrica (‘The Fabric of the Human Body’).Footnote 19 Vesalius’s work prompted a productive series of anatomical investigations into the ear in Renaissance Italy. Many of Vesalius’s pupils contributed to the accurate descriptions of the minute and delicate parts of the ear. Yet, anatomy did not offer a clear explanation for how hearing worked – or deafness, for that matter. Moving beyond the solid parts of anatomy, Du Verney therefore began to analyse the fluid parts in the ear to understand the physiological process of hearing and the causes of deafness. His approach would be adopted by eighteenth-century medical professors like Antonio Maria Valsalva (1666–1723), Albrecht von Haller (1708–77) and Giovanni Battista Morgagni (1682–1771).
Based on his anatomical research, Du Verney explained the origins of earwax and its function in healthy hearing. In the first part of his treatise, Du Verney described and depicted the structure of the outer ear, the ear passage (meatus auditorius) and its outer layer of skin, which housed numerous round follicles (see Figure 1).Footnote 20 By short ducts, these glands steadily secreted an oily substance, which moisturised the skin and slowly became thicker, bitter and inflammable.Footnote 21 By way of simple experiment, his later colleague Von Haller, professor of anatomy, botany and medicine at the newly founded Hanoverian University of Göttingen, concurred that earwax was continuously being discharged. By taking a piece of black velvet and rubbing his ears a hundred times in an hour, Von Haller found that the cloth kept on wiping off traces of wax.Footnote 22 According to Du Verney, the function of the continuous secretion of earwax was twofold: first, its oily character lubricated the tympanic membrane (eardrum), preventing it from drying out and losing its tension. Second, the bitter property prevented dirt, insects and other extraneous bodies from entering and hurting the eardrum. In Du Verney’s words, ‘the wax […] stops any filth and insects which else might enter into the ear, and which would be a sure cause of impairing the membrana tympani’.Footnote 23 In the later eighteenth century, the chemist Antoine François de Fourcroy (1755–1809) added a third function, namely to soften the sonorous vibrations of the air and moderate loud noise.Footnote 24
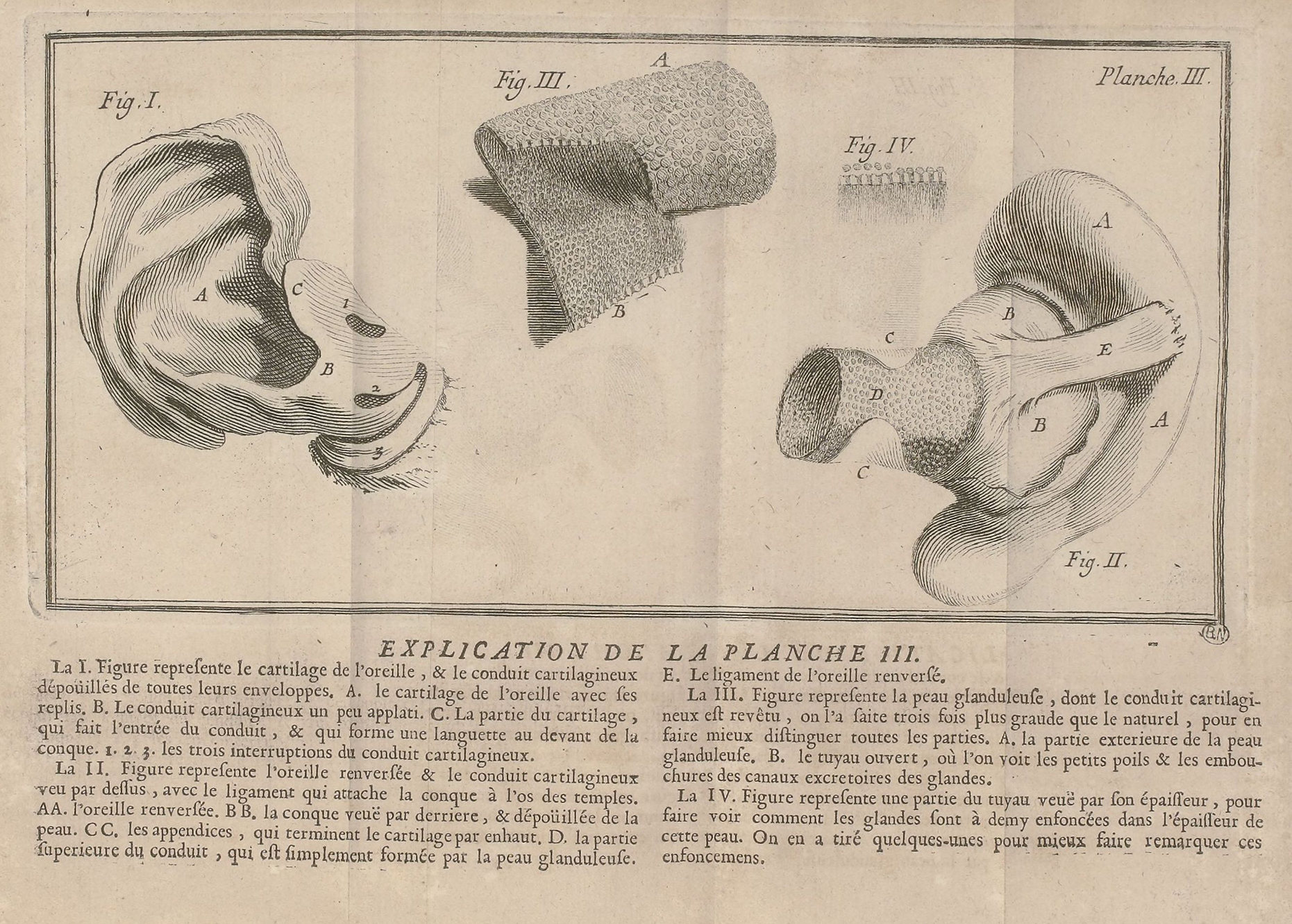
Figure 1 The glandular skin in the ear canal, in G.J. du Verney, Traité de l ’ organe de l’ ouie (Paris, 1683), Planche III. Source: Bibliothèque nationale de France.
Earwax also had its downsides, however, owing to its potential viscosity. Du Verney described how earwax could be too thick or secreted in too large quantities, thus damaging the ear and one’s hearing. Dried up earwax and dirt could block the ear passage, even causing severe deafness. Du Verney noted that
It is not long since, that searching out the cause of deafness in a person, who had been afflicted with it many years before his death, I found in the auditory passage, about two lines from the membrana tympani [eardrum], a small pellet, which was soft and pretty thick with a considerable quantity of filth indurated, collected before it, and I don’t doubt but that this sort of deafness is very common.Footnote 25
Earwax-related deafness was indeed fairly common. In the 1670s, Robert Hooke (1635–1703), an eminent member of the Royal Society, recorded in his diary his own experiences of impaired hearing. He particularly complained about tinnitus, a ringing or buzzing in the ears. Hoping to unblock his ears, in December 1672 he filled his ear with warm honey, wool and the oil of bitter almonds. But on New Year’s Day 1673, Hooke still woke up with a ‘strange noyse in right ear […] like a horne or bell’, which continued to plague him for months.Footnote 26 Finally, on Monday 11 August, Dr. Carew syringed Hooke’s ears, which helped to ‘fetch out a core’ of earwax; he had no complaints about noise in his head for the next 8 months.Footnote 27 Hooke was far from the only one who experienced earwax viscosity. In the eighteenth century, numerous physicians commented on the hardness of hearing caused by the formation of stones or the collection of cerumen in the ears.Footnote 28
Du Verney hypothesised that the cause of earwax viscosity was the cold, which thickened the wax. After all, the external ear was open to the elements. In addition, people of a phlegmatic temperament were generally believed to be colder and therefore prone to earwax accumulation, bringing about swellings, ear pain, feelings of heaviness and hardness of hearing. As a remedy, Du Verney suggested the application of heat: stopping the ear with thick wool or cotton perfumed with musk, in order to open the pores and stimulate the flow of earwax. Injections also became a popular treatment, for which surgeons and doctors commonly used milk, water with thistle or other decoctions, including linseed oil mixed with drops of spirits of wine, oil of bitter almonds or mineral water. For instance, the French physician and botanist François Boissier de Sauvages de la Croix (1706–67) relayed that he had pulled out some thick, hardened wax by injecting the ear with mineral water for several consecutive days. Soap, honey or another solvent was dissolved in the heated water before it was injected.Footnote 29 The chemist De Fourcroy performed in vitro experiments with earwax in the chemical laboratory to see the effect of these treatments. His colleague Jean-Noël Hallé (1754–1822) had been struck with excessive earwax secretion to such an extent that he furnished De Fourcroy with sufficient quantities of cerumen to enable chemical analyses. The earwax hardened over time and grew dry and bristle in air, but melted with heat and could dissolve as emulsive in water. Further chemical experiments sought to identify the components of earwax, but these first results already supported the most prevalent treatments.Footnote 30
If none of the above remedies worked, physicians suggested instruments to physically remove the earwax. Du Verney, for instance, recommended the use of ear spoons or ear scoops made of ivory or silver, followed by a series of injections if necessary.Footnote 31 These earwax removal treatments gained significant traction in the eighteenth century. Surgeons and healers, such as Margaret Searl in London, advertised deafness cures in newspapers and broadsheets.Footnote 32 In 1741, Archibald Cleland (c. 1700–71), surgeon to general Wade’s Regiment of Horse, presented an optical instrument made of convex glass and a candle to gain a better view of the hardened wax. If forceps were unable to remove all excess earwax, he suggested steaming the ears to dissolve the viscous substance.Footnote 33 Finally, Lorenz Heister (1683–1758), a professor of anatomy and surgery at Helmstedt and author of the authoritative and much reprinted manual on surgery, suggested probes, pliers and scissors to remove earwax and other foreign bodies that had entered the ear.Footnote 34
In short, the viscosity of earwax prompted physicians to perceive deafness as fluid rather than fixed and permanent. People could acquire deafness or hardness of hearing once, or indeed several times, during their life. Although today we may recognise the build-up of earwax as a simple case of conductive hearing loss, around 1700 earwax was not confined to this type of deafness. As a fluid it showed great variability.Footnote 35 Earwax flowed in and between various hearing categories, from unobstructed hearing to tinnitus and deafness. This transformed the meaning of deafness among medical practitioners, too: not as something static and permanent, but as something potentially episodic and brought about by weather conditions.
The fluid of sound
That hearing and deafness were construed as essentially fluid is also evident from the way physicians and natural philosophers envisioned sound. The notion that sound moved in the form of acoustic waves is centuries old; even today, sounds are explained in terms of oscillations in a medium. Many natural philosophers viewed the propagation of sound as akin to the dropping of a pebble on a smooth surface of water, its waves consequently spreading out evenly in all directions.Footnote 36 According to Von Haller, ‘sonorous waves of the air flow […] much after the same manner as we see water, without air, transfer any impulse that is given to it’.Footnote 37 This wave-like depiction of sound helped explain concepts of volume. ‘If you throw two stones at once into a lake’, the French surgeon Claude-Nicolas Le Cat explained, ‘the undulations they will form in the water, will either be confounded in the one alone, or be mutually destroyed. For the same liquid is not susceptible of two or more different vibrations at once’.Footnote 38 At first glance, the understanding of sound in terms of waves in the water simply appears to be a useful metaphor. On closer inspection, however, medical men actually saw the propagation of sound as fluid in a literal sense. Le Cat went so far as to argue that
It is necessary then that the air, which generates sound, be composed of several species of fluid, more or less subtle, each of them imbued with a property of producing the vibrations, or the different tones, of Ut, Re, Mi, &c much after the manner as light is formed of several kinds of rays adapted to the production of red, yellow, green, blue, &c.Footnote 39
In other words, Le Cat claimed that not the air, but various ‘species of fluid’ in the air transmitted sound by their vibrational motion. Le Cat’s understanding of hearing in terms of subtle fluids effectively reconfigured hearing as a ‘soundscape’ of fluids and waves. Furthermore, Le Cat’s theory was far from idiosyncratic: it perfectly fit the eighteenth century conception of air as fluid, as well as the broader notion that numerous subtle fluids exist.
Thinkers in the eighteenth century were particularly attuned to the notion that the air behaved like a fluid. Natural philosophers, academics and gentlemen amateurs – some of whom were member of medico-meteorological societies like the Natuur- en Geneeskundige Correspondentie Societeit (‘Nature and Medical Correspondence Society’) in The Hague – increasingly owned measuring instruments to keep track of the fluid characteristics of the air and to speculate about its effects on human health.Footnote 40 Weathervanes on top of churches and other tall buildings showed the direction of the wind as a current of air flowing from one place to the other, quicksilver thermometers indicated the hotness of air in summer and the coldness of air in winter, hygrometers measured the humidity of the air and barometers demonstrated changes in the weight of air from high to low pressure and vice versa.Footnote 41
Eighteenth-century textbooks also identified the air as a fluid. A case in point was the lecture series given by Hieronymus Gaubius (1705–80), a professor of medicine and chemistry at Leiden University. He referred to ‘that fluid the air’ (fluidum aërium), which would have a direct impact on health. In his pathology lectures, Gaubius systematically discussed all ‘noxious powers of the atmosphere’. For example, air could be too hot and too dry, exhausting the body, or it could be too cold and too moist, diminishing the body’s vital motions. The particularities of the air were taken very seriously indeed, because ‘the atmosphere, where it surrounds and penetrates the human body, presses it equally in every point in the manner of fluids’.Footnote 42 This was demonstrated by patients who, when the air pressure dropped – as was evident from the drop in quicksilver in the barometer – suffered from acute rheumatic pains (from rheuma ‘stream’, thought to be caused by the internal flow of ‘watery’ humours).Footnote 43
Physicians argued that certain qualities of the air could also affect the sense of hearing. Damp air in particular was thought to blunt the senses and dilute hearing. When Gaubius’s colleague Johannes de Gorter (1689–1762), a professor of medicine in the Dutch port city of Harderwijk, researched the effects of climate on the body, he noticed the impact of mist on one’s hearing. ‘Moist air dampens the sound, like in mist’, he noted, ‘partly because our bodies are weaker, and hence can vibrate less’.Footnote 44 Indeed, Boissier de Sauvages explained how excessive humidity, in combination with a hot, southern wind, could cause the eardrum to relax too much. Humid weather obstructed normal perspiration, causing an overabundance of serous fluid in the body. Conversely, for Boissier de Sauvages, deafness was principally the result of a cold, northern wind that made the eardrum too dry and rigid. If the cold affected the internal ear, the communication of sound would become confused, leading to a so-called loud hearing: ‘The reason for this dissonance between the internal & external sound is that the hammer & stirrup muscles, stiffened, thickened & clogged up by the humor that causes the cold, can neither position nor stretch the membrane or the oval window to a point that matches the tone of voice of the speaker’.Footnote 45 Boissier de Sauvages went on to distinguish over twenty ‘species’ of deafness, but it is clear from his examples that it was often extreme weather conditions that eroded one’s capacity to hear.Footnote 46
Yet the ways in which wind and air impacted on hearing did not explain how sound itself flowed through the air. It was Le Cat who first presented a comprehensive theory of sound in terms of subtle fluids moving in the air. When in the 1750s, the Académie des Sciences, Inscriptions et Belles-Lettres in Toulouse launched an essay competition on the subject of hearing, Le Cat seized this opportunity to expand on his concept of subtle fluids.Footnote 47 In 1757, he was awarded the golden medal worth 1,500 francs, but his essay La théorie de l’ouie (‘The Theory of Hearing’) was not published until 1768, in the third volume of his Oeuvres physiologiques. The book was adorned with an impressive allegorical frontispiece, showing Minerva sitting on a large sphere holding a beadle and harp, surrounded by numerous putti – all signifying objects and themes in the theory of hearing (see Figure 2). At the bottom, two putti appear to symbolise the ear’s anatomy: one plays with the small bones of the middle ear another with a model of the inner ear. Two putti in the middle hold up hearing instruments, one to enhance the sound through a trumpet and the other listening with a hearing aid. On top, an orchestra of putti play the organ and various other musical instruments. Le Cat himself is depicted observing and making notes on the scene. Befittingly, these three subjects visually represent the progression of Le Cat’s book, in which he first discussed ear anatomy, followed by sound, and ending with effects of sound and music on the hearing organ.

Figure 2 Frontispiece by Dumarest in Claude-Nicolas Le Cat, La théorie de l’ ouie (Paris, 1768). Source: Wellcome Collection, Public Domain Mark 1.0.
To support his theory of subtle fluids of sound, Le Cat structured the second part of his book in propositions, supported by arguments and experiments. He first set out to prove that air – in particular a subtle part of the air – was the medium that transmitted sound. Le Cat had a bell ring inside a vacuum pump and clearly perceived that the sound was significantly weaker once the air had been sucked out.Footnote 48 Another experiment made use of the effects of the wind on sound. Three men were positioned at appropriate distances from each other, along the direction of the wind. When the middle man produced a sound, the man upwind had more trouble hearing this sound than the man downwind. As Le Cat observed, ‘it is a constant fact that the wind is a current of air; therefore, the air is the medium that carries sound and noise’.Footnote 49 Even so, Le Cat argued that ‘crude’ air had to be distinguished from ‘subtle’ air, which he also verified by experiment:
If you place your ear next to a large ringing bell, this organ will be vividly moved; but put a candle in the place of your ear, give a great hammer blow on the bell, and you will not notice the slightest movement in the flame of this candle; yet the slightest draught will move it, & the wind that will be strong enough to extinguish it will not make the slightest impression on your hearing.Footnote 50
In other words, while wind and sound occupied the same space, were intimately connected, and moved reciprocally, a crude air that made up the wind had to be distinguished from a more subtle air that carried the sound. The subtle part of air was identified as the essential medium of sound, and, because of its characteristics, this subtle air was envisioned as fluid.
But although Le Cat may made the existence of subtle parts in air a plausible hypothesis, substantiating his claim that sound was composed of ‘several species’ of fluid proved more difficult, because he could not provide empirical proof of the existence of these fluids. Instead, he resorted to analogy. He argued that just as a string on a harp could not make numerous vibrations at the same time, a single subtle fluid of air could not receive and preserve various movements at the same time. Once again, Le Cat made use of the analogy of water waves:
A single stone thrown into a given area of water produces undulations that spread from the centre of impact to the circumference; yet several stones thrown into the same water produce only confused movements. As such, the regularity & the difference with which several sounds are heard at the same time are convincing proof that the fluid carrying them is composed of as many different matters as there are different tones.Footnote 51
In Le Cat’s theory, therefore, each tone had its own unique vibration, for which there existed one corresponding subtle fluid. The ‘sound fluid’ (fluide sonore) was accordingly not just one fluid, but instead composed of as many species as there were different sounds. According to Le Cat, this was a feature that could also apply to the other senses. He conjectured that species of fluids of other configuration, density and subtlety were the object of odours, flavours and sights. This was proven, for example, by the transpiration of plants exuding aromatic fluids in spring and summer, or the invisible perspiration of animals and humans, who give off their bodily odours to the air – invisible to the eye, but clearly discernible to the nose.Footnote 52
Given that physicians understood the natural world and the human body as essentially composed of fluids,Footnote 53 it is not surprising that the auditory perception – the mechanism of this sensation in the body – was increasingly understood in terms of subtle fluids, too. According to physiologists like Boerhaave and Von Haller, sound waves were collected by the outer ear and strengthened by reflection against the bone and cartilage in the auditory passage. Reaching the tympanic membrane (eardrum), the sound affected a chain of ossicles in the middle ear, reaching the oval window of the inner ear. The last ossicle, the stirrup, compressed the nervous pulp of the vestibule. Somehow the sensation was transferred from the labyrinth and semi-circular canals to the auditory nerves, but how exactly remained a mystery. A number of physicians, including Antonio Valsalva, Raymond Vieussens (c. 1635–1715) and Johann Friedrich Cassebohm (1698–1743), hypothesised the presence of a subtle fluid.Footnote 54 In 1742, Theodor Pyl claimed that the entire cochlea were filled with an ‘elastic fluid’.Footnote 55 It was in 1761 that the Italian anatomist and physician Domenico Cotugno (1736–1822) undeniably demonstrated the presence of a serous fluid in the labyrinth of the inner ear. He argued that this ‘exhalation from the blood vessels’ was ‘to protect the nerves’ and played a part in the transmission of sound.Footnote 56 Dissectors had previously cut the head from the neck, thereby losing these fluids. But, as a skilled dissector, Cotugno also proved the existence of the fluids in the brain and spine. As Le Cat summarised:
All the inner chambers of the organ of hearing, as well as all the cavities of the skull, are thus filled from their creation onwards with a fluid, a subtle air, extracted from a person’s bodily fluids; & even in adults, all the voids in the labyrinth can only be filled with vapours of this matter, emanating from the fluids contained in the vessels that moisturise the nervous tissue of this organ.Footnote 57
Le Cat deftly used the words ‘fluid’ and ‘air’ interchangeably, because prior theories of hearing were built on the Aristotelian concept of ‘internal air’ (aer insitus or aer internus). This internal air, so he believed, corresponded with the air in those parts of the brain responsible for auditory perception. Rooted in Aristotelian thought, this concept had become a cornerstone of European medicine, which made it difficult to discredit or even refute its existence. Yet, Le Cat’s theory had circumvented this problem by transforming air itself into a fluid – hence the ancient term could still be used. Sound and vibrations of the internal air had simply evolved into one of the subtle fluids in the air.
The final step in the mechanism of auditory perception was the notion of nervous fluids that communicated sounds to the brain. In the course of the eighteenth century, theories on the nature of the nerves shifted from a model based on ‘animal spirits’ to one of ‘nervous juices’. While notions of resonating and vibrating nerves remained popular, this was increasingly explained in terms of the flow of ‘nervous juices’, as is evident in the works of physicians such as Du Verney, William Cullen, De Gorter and Von Haller.Footnote 58 These nervous juices were thought to be affected by the sound waves, and, when flowing to the brain, to bring about auditory sensations. In the words of Le Cat: ‘The fibres of this nerve are filled with the fluid that flows in this kind of vessel, & the soul is united with this nervous fluid’.Footnote 59 Based on new theories of hearing and supported by the discovery of fluids in the labyrinths and nerves, the propagation of sound and the physiology of hearing were firmly rooted in fluids.
What impact did this theory have on explaining the ‘hard of hearing’ (l’ouie dure)? In essence, hardness of hearing could be compensated with increased sound. In order to gather more subtle fluids of sound in the ear, Le Cat designed his own hearing aids, which he presented at the end of his book (see Figure 3). His first set of acoustic devices were modelled after a conch shell: thanks to their large opening they were able to gather a larger volume of sound than the external ear, while their domed shape reflected and amplified the sounds further inwards. The devices were placed on the ear and could be covered up with a wig.Footnote 60 For the more severely deaf, Le Cat invented an elaborate ear trumpet, the design of which was based on the anatomy of the ear itself, including an artificial eardrum. The numerous convolutions would multiply and enliven the sound vibrations before entering the auditory canal of a deaf person. Although this device was fairly large, according to Le Cat it proved very effective, surpassing the performance of all other ear trumpets.Footnote 61
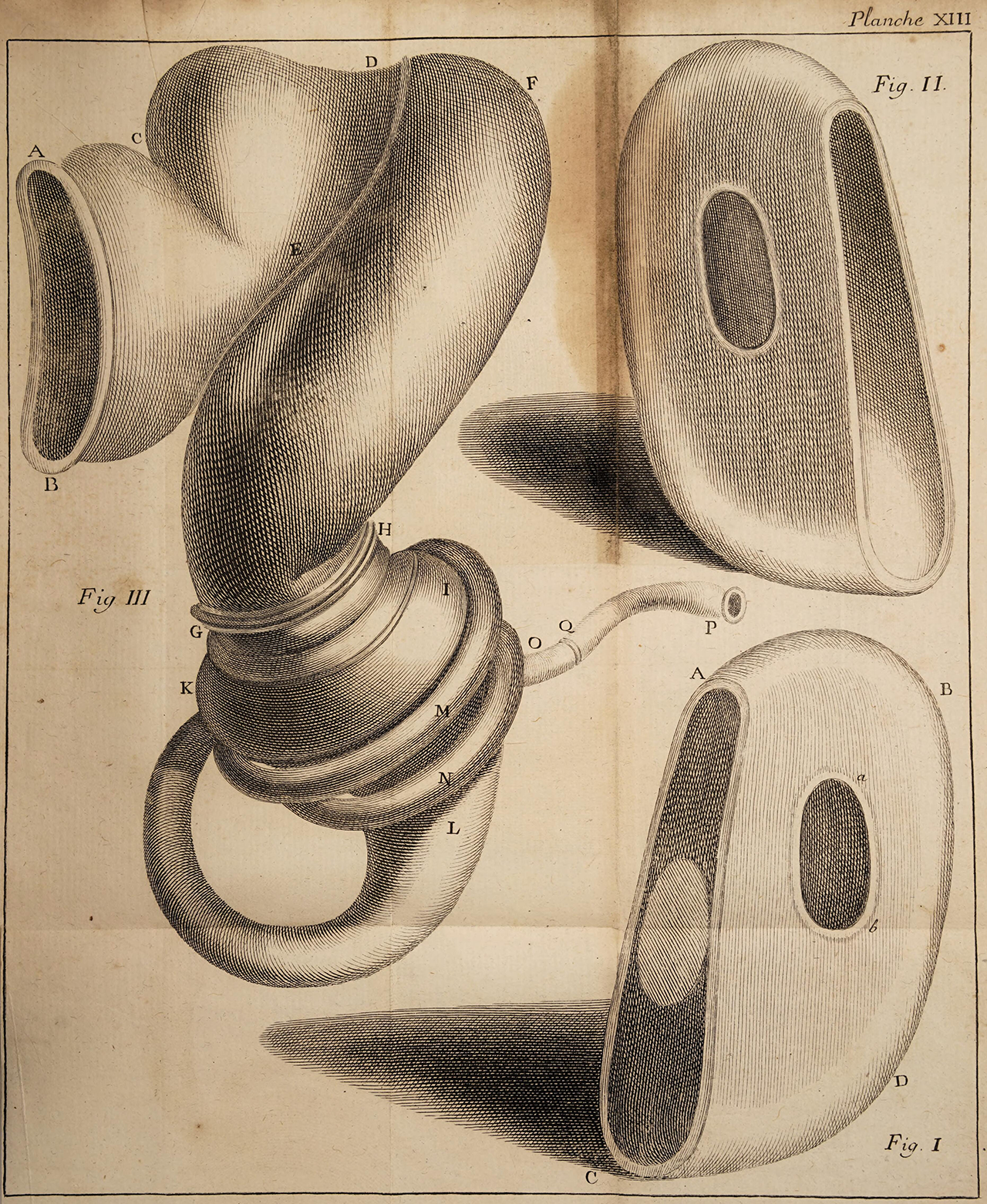
Figure 3 Two ear shells (right) and ear trumpet (left) in Le Cat, La théorie de l’ ouie (Paris, 1768), Planche XIII.Source: Wellcome Collection, Public Domain Mark 1.0.
In sum, early modern medical treatises clearly suggest that sound and hearing as fluids and waves were not just metaphors: they were envisioned in a literal sense. Within this neo-humoral physiology of nervous juices and fluids of the labyrinths, physicians understood the entire concept of hearing in terms of fluids as well. They effectively reconfigured hearing as a soundscape of subtle fluids and waves. At the same time, new acoustic devices underlined the fluidity between hearing and deafness, because hardness of hearing was ameliorated by increasing the volume of fluid sound.
Draining pus and mucus
The final example of fluidity concerns the understanding of deafness as the result of morbid fluids congested in the middle ear – a deafness that could potentially be overcome by their forced excretion. Observing cases of disease and infection, eighteenth-century surgeons discovered new ways to improve the experience of hearing difficulties by means of the technological innovation of catheters. Their treatments involved the syringing with liquids to help excrete fixed pus and mucus stuck in the middle ear. The relative success of these new instruments contributed to the notion that certain types of hearing difficulties were the result of disease, rather than necessarily fixed conditions. While the actual number of treatments were few and far between, the publication of favourable results nevertheless instilled confidence among medical men that certain hearing difficulties previously thought to be permanent could in fact be made episodic.
Early modern physicians were well aware that morbid obstructions in the middle ear could lead to serious hearing difficulties. Under ordinary circumstances, the Eustachian tube leading from the pharynx behind the nose and mouth to the cavity of the middle ear was supposed to be slightly moist.Footnote 62 This narrow passage was seen as ‘a kind of aqueduct capable of carrying the vapours and even liquors, either natural or diseased, into the cavity of the gullet’.Footnote 63 But in the case of a throat infection, swellings or mucus accumulated and ultimately blocked it. The blockage would cause a build-up of excess airs and fluids in the inner ear and thereby interrupt the communication of vibrations from the external air to the auditory nerves. Besides suffering from difficulties with breathing and heavy earaches, patients could also experience a growing deafness.Footnote 64 Valsalva recalled the case of a nobleman, who had a mucus plug in his nose. The bigger this nasal mucus plug became, stretching all the way to the uvula, the more it squeezed the opening of the Eustachian tube. The man’s hearing diminished daily until he became profoundly deaf.Footnote 65 Other patients experienced deafness due to an infection and the accumulation of pus. Morgagni shared the case history of a 12-year-old boy, who, after having suffered from smallpox, grew a tumour behind his right ear, became ‘quite deaf, [and] discharg’d a purulent matter’. A surgeon made an incision, which released a ‘large quantity of pus’, but in the following days the boy remained delirious, weak and ultimately died. When Morgagni performed a dissection of the boy’s head, he determined the cause of death to be the decay of the temporal bone by the effusion of pus in the middle ear and in between the dura mater, causing the pain and hearing difficulties. Morgagni investigated another young man who died of a similar fistula, but who nevertheless had continued to hear.Footnote 66 These cases show, therefore, that the deafness itself was not recognised as the disease, but the result of one.
Physicians had a series of treatments at their disposal to attend to their patients and possibly relieve them of their predicament. If the Eustachian tube was blocked by a swelling of pus, breaking it was usually sufficient to restore hearing, and, when the throat infection disappeared, hearing was often restored as well. If patients failed to recover, physicians ordinarily prescribed gargle fluid (gargarismata), sneeze powder (sternutatories), chewing tobacco (apophlegmatisms) or purgatives (cathartics) to free the tubes and nostrils of any extant phlegm, mucus or slime.Footnote 67 Mrs. Tillotson, the wife of John Tillotson and a friend of Robert Hooke, appears to have accidentally performed this treatment when she took beet juice to clear her nose, but also recovered the hearing in her ear.Footnote 68 When faced with more serious diseases, such as violent fevers and the infection of the mastoid process, physicians resorted to well-known therapies such as bloodletting, purging, lactating, leeches, plasters, roasted onions, or other forms of heat.Footnote 69 These treatments, however, would not do much for the patient.
The discharge of pus and mucus by applying syringes and catheters proved to be a real breakthrough in restoring the hearing of some patients. In the 1720s, the postmaster of Versailles, Edme-Gilles Guyot (1706–86) claimed to have relieved his own deafness by syringing with water. When he experienced deafness and found no relief, he invented a syringe that was a tube of tin, bent at an angle and connected with a leather bag.Footnote 70 He introduced this syringe into the mouth and behind the palate, squeezing the bag to spray warm water in a thin stream into the cavity.Footnote 71 Guyot’s incidental yet successful operation signalled the start of further experiments with Eustachian tube catheterisation. In the course of the eighteenth century, a number of medical men in England and France experimented with various types of catheters. The English surgeon Archibald Cleland fitted a flexible silver tube to a syringe, ‘whereby warm water may be injected or air blown into the Eustachian tube so as to dilate it sufficiently for the discharge of the excrementitious matter that may be lodged there’.Footnote 72 The French physician Antoine Petit (1722–94), however, questioned whether spraying liquids via the mouth would do anything more than wash the entrance of the Eustachian tube. This could be useful in itself, he admitted, but it certainly did not mean actually injecting the tube. Instead, he suggested introducing the catheter via the nostril, and, in doing so, he more conveniently and successfully injected fluids into the Eustachian tube (see Figure 4).Footnote 73 Likewise, the Scottish anatomist John Douglas (d. 1759) is said to have proposed Eustachian catheterisation via the nose.Footnote 74 What had started as an accidental success had therefore quickly caught the attention of surgeons across Europe.
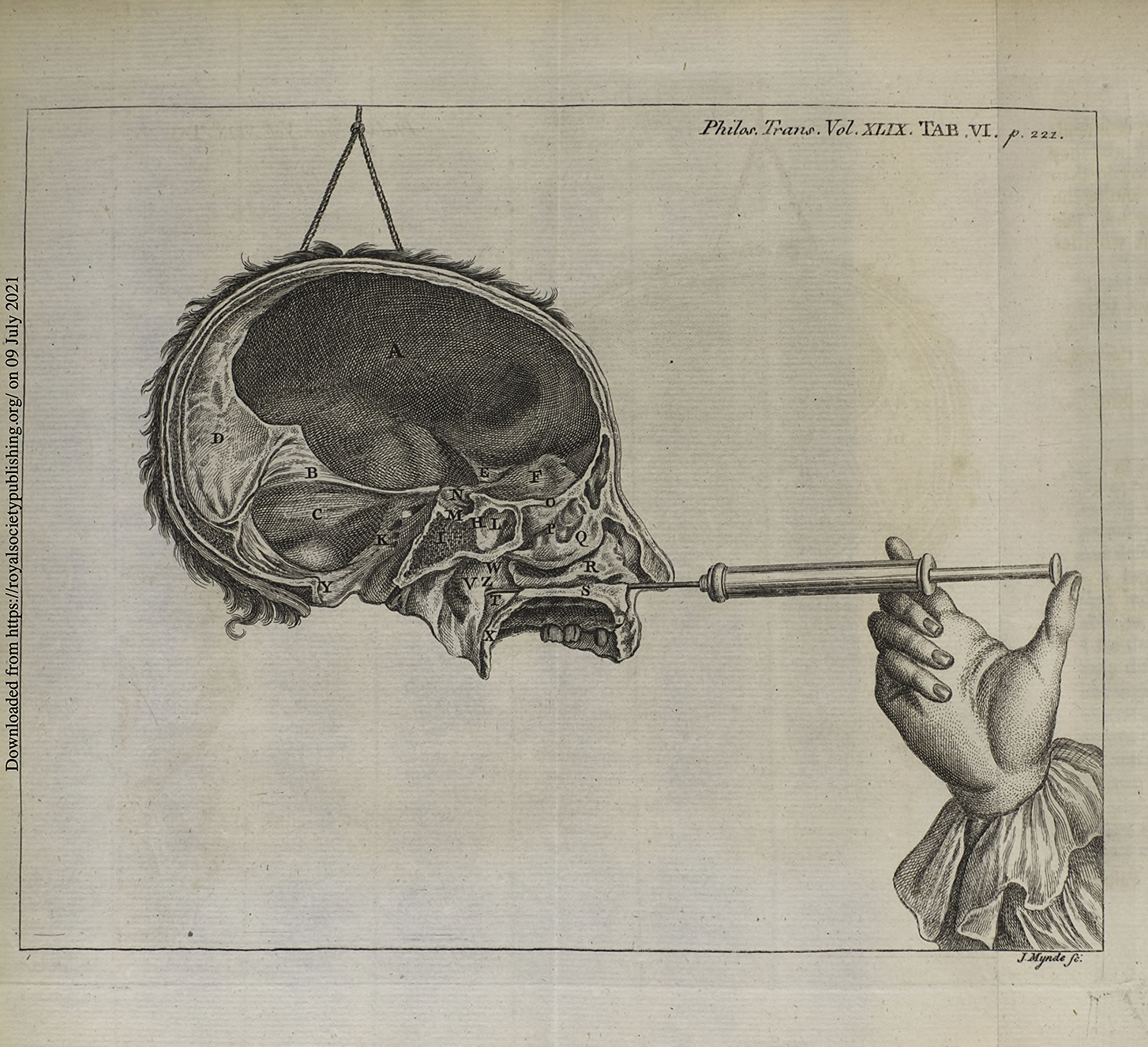
Figure 4 Engraving showing mode of use of Eustachian catheter via the nose, by J. Mynde, in Jonathan Wathen, Philosophical Transactions 49 (1755). Source: Royal Society, Public Domain.
Even a few cases of mastoiditis were successfully treated by syringing and discharging the accumulated pus. In 1776, the Prussian surgeon J.L. Jasser successfully performed a mastoidectomy on a German soldier named Hittberg, who had been suffering from painful earaches for many years. Hittberg had not only turned deaf in both ears, from his right ear also continually flowed purulent matter. While still working in the army, Hittberg was placed among the Polish recruits who, not understanding the German language, were also regarded as deaf. Jasser was forced to intervene when Hittberg suffered from extreme pain, violent fever and the formation of a large abscess behind the ear. He made an incision into the mastoid of about a thumb long, which already released some yellowish, thin yet sharp pus. Injecting tea into the opening had a surprising effect, as the soldier exclaimed feeling the flow in his head and the water and pus started flowing out his right nostril. In the days that followed, Jasser continued to irrigate the area with warm water to drain the large amount of purulent matter away. Hittberg happily felt the pain slowly disappear and his hearing increase.Footnote 75
The extent to which syringing the Eustachian tube and mastoid was commonly applied beyond these case studies is difficult to ascertain. Jaipreet Virdi is doubtful whether any practitioners routinely offered Eustachian tube catheterisation.Footnote 76 Mastoidectomy and draining away pus indeed remained a rather rare intervention in the eighteenth century.Footnote 77 Periodical mentions indicate, however, that the practice of Eustachian catheterisation was adopted in a few places across Europe. In 1780 at the Rotterdam hospital, Gerard ten Haaff (1720–91) syringed warm water into the Eustachian tubes of Jan Gardenier, relieving him from a ‘heavy deafness’ and ‘fierce ringing’ or tinnitus.Footnote 78 Boissier de Sauvages, when discussing these categories of deafness and the syphon as proposed by Cleland, claimed that ‘the surgeons of Montpellier use the catheter’.Footnote 79 The most extensive and systematic application of Eustachian tube catheterisation was executed by the London surgeon Jonathan Wathen (c. 1728–1808). In the 1750s, Wathen tried his hands at Eustachian catheterisation via the nostrils, reporting the successful treatment of six people to the Royal Society the following year. His first case history concerned a 40-year-old woman who experienced ‘considerable deafness […] but as soon as the internal meatus was injected, she instantly affirmed, that she heard much better’.Footnote 80 His second test subject was a 50-year-old man who had deafness in both ears after having had a cold. Wathen ‘injected the tube on one side and washed away a very considerable quantity of congealed mucus, in little clots of a blackish colour and putrid smell’.Footnote 81 When the patient regurgitated, he immediately heard what was said. Wathen reported similar results in another four cases, though with varying degrees of success: the third patient had a plug of earwax removed and his tubes syringed, resulting in his being able to hear his watch; case four, who had turned deaf after having had a cold, regained some of her hearing, enabling her to wait tables and work; examinee five received relief in one ear; and the sixth and final test subject, who was ‘deaf to the greatest degree’ for eighteen years, heard his own voice after being syringed. However, the subject of the sixth case experienced hearing as ‘a very painful tintillation [sic], or (as he himself termed it), a scratching in his ear’.Footnote 82 With a relative success rate of five out of six, Wathen was cautiously optimistic about this treatment, writing that his method could give ‘a probable change to the unhappy sufferer’.Footnote 83
Despite Wathen’s positive outlook towards catheterisation, physicians were well aware that irrigating the inner ear cavities was no panacea for all hearing ills. Authoritative medical professors such as Gerard van Swieten (1700–72) and Morgagni warned that if the swellings and slime were caused by venereal disease – which was not uncommon at the time – the ‘foul ichor’ or slime of the infection could eat away parts of the tube and inner ear. Even if the disease had dissipated, the resulting scar tissue could bring about a concretion of the tube, resulting in a permanent deafness.Footnote 84
Nevertheless, the medical understanding and treatment of infected mastoids and congested Eustachian tubes was clearly one of fluid deafness. Morbid matter like mucus and pus was recognised as being literally responsible for the onset of hardness of hearing. Technological innovations with syringes enabled the excretion of these slimy fluids, and in few cases, an amelioration of the pain and hearing difficulties. While mastoidectomy and Eustachian tube catheterisation appear to have been applied on a modest scale, they nonetheless added to the medical understanding of deafness as a fluid state, in a few cases having the potential to render deafness episodic rather than permanent.
Conclusion
This article has sought to demonstrate that analysing early modern medical perceptions is a useful perspective for the study of deafness and hearing difference. First of all, analysing the phenomenon of deafness and hardness of hearing in the works of physicians and surgeons deepens our understanding of deafness in early modern medical knowledge, challenging the historiographical notion that deafness and hearing were diametrically opposed. Hearing and deafness were in fact positioned along a spectrum of auditory disability, with numerous stages in between; there was thus a much more fluid and continuous notion of hearing and deafness than is often assumed. Second, exploring the category of deafness and hardness of hearing demonstrates that such hearing differences were interpreted as resulting from a close interplay between the physical body and the environment, both in theories about the propagation of sound and in the way extreme temperatures, winds and damps could affect the body. Whereas today atmospheric conditions are scarcely a medical issue, in early modern times the weather directly impacted people’s lived experiences.
Furthermore, it is significant that deafness was not a neglected topic in early modern medical research. On the contrary, it could be argued that deafness – and hearing differences more broadly – affected key topics in medicine and natural philosophy, including the nature of sound, the physiology of the nerves and senses, and notions of disease and debility.Footnote 85 Bodily fluids functioned as the defining aspect linking all these seemingly diverse topics. Indeed, the medical study of deafness – with its focus on earwax viscosity, on mucus and pus in the Eustachian tubes and mastoid bone, and on the subtle fluids in airs and nerves – showcased the prevalence of fluids in explanatory models for a wide variety of ear conditions. In 1763, François Boissier de Sauvages recalled once again the man from Chartres, who, though having been deaf his entire life, miraculously started to hear ‘by a flow of water through his ears’.Footnote 86 He connected this story to other instances in which deafness and hardness of hearing were instigated by cephalalgy (headache), dropsy, or middle ear effusions, and he hypothesised that those born deaf had probably formed an abscess in their ears. Fluids, in other words, gave early modern physicians the opportunity to reasonably explain the occurrence of hearing difference. It also invited speculation about possible treatments for the loss of hearing, such as earwax removal and Eustachian tube catheterisation. As such, the historical study of deafness reveals much about the importance of fluids and the nature of seventeenth and eighteenth century medicine.
Acknowledgements
Previous drafts have been presented at the Leeds Centre for History and Philosophy of Science in 2020 and the Northern Network for Medical Humanities Research Congress 2021. I am grateful for the helpful comments and suggestions by Jane Macnaughton, Justin Begley, Tom Hamilton and the two anonymous reviewers.
Funding
Research for this paper was funded by a Dutch Research Council Rubicon award for the project ‘Deafness in Transition: Disability and Hearing Difference in Enlightenment Europe’ (2019–2022).





 Open access
Open access