


In most European countries, working hours have decreased over the past two decades but work intensity has increased(Reference Parent-Thirion, Vermeylen and van Houten1). Tight deadlines and high work demands have been reported by 60 % and difficulties in combining work and personal life by 18 % of workers in Europe(Reference Parent-Thirion, Vermeylen and van Houten1). At the same time, a study conducted in twenty-three European countries showed that sleep problems were common, with prevalence rates varying from 16·6 % in Denmark and Italy to 31·2 % in Poland(Reference van de Straat and Bracke2). A Finnish population study showed that sleep duration had decreased and sleep complaints increased between 1972 and 2005(Reference Kronholm, Partonen and Härmä3,Reference Kronholm, Partonen and Laatikainen4) and that 21 % of women and 17 % of men reported frequent sleep problems which were associated with sickness absence spells(Reference Rahkonen, Lallukka and Kronholm5). Increased sleep complaints and work stress have been shown to associate with a higher need for recovery (NFR) from work(Reference Silva-Costa, Griep and Fischer6,Reference Karhula, Härmä and Sallinen7) .
During the last working hours or after a workday, workers may recognise feelings of overload, irritability, social withdrawal, lack of energy for new effort and reduced performance(Reference van Veldhoven and Broersen8). These feelings refer to workers’ insufficient recuperation from work(Reference van Veldhoven and Broersen8,Reference Van Veldhoven and Meijman9) . In principle, workers recuperate from work-induced fatigue between their work shifts. When recovery from work has been optimal, the worker has no feelings of work-related stress when starting a new workday. Various factors, such as demanding work, age, gender, education, working time and perceived health status, have been identified as factors that affect workers’ ability to recover from work(Reference Jansen, Kant and van den Brandt10,Reference Jansen, Kant and van Amelsvoort11) . High NFR from work has been associated with occupationally induced fatigue, meaning that an increased NFR measures the early symptoms of work related fatigue(Reference van Veldhoven and Broersen8,Reference Sluiter, de Croon and Meijman12) .
Workers’ NFR from work has predicted workers’ health complaints(Reference Sluiter, van der Beek and Frings-Dresen13). Emotional exhaustion and sleep problems were more prevalent when recuperation from work was insufficient(Reference Sluiter, de Croon and Meijman12). Sleep disturbances and long-term incomplete recovery from work were associated with the duration of sickness absence, and incomplete recovery from work was associated with CVD over the course of a few years and with mortality a few decades later(Reference de Croon, Sluiter and Frings-Dresen14–Reference Lallukka, Kaikkonen and Härkänen17).
Insufficient recovery from work and sleep problems may influence workers’ lifestyle habits. In a study of construction workers, workplace stress and fatigue affected workers’ dietary habits, decreasing fruit and vegetable intake(Reference Nagler, Viswanath and Ebbeling18). Recent review articles concluded that insufficient sleep increases food consumption, the risk for poor dietary habits, total energy intake, total fat intake and snacking. Some studies have suggested that insufficient sleep relates to lower fruit intake and to otherwise lower-quality diets(Reference Dashti, Scheer and Jacques19–Reference Golem, Martin-Biggers and Koenings21). Studies on sleep and nutrition have mostly focused on sleep duration, but there is some evidence that among female workers, poor sleep quality may be associated with unhealthy food choices such as low intake of vegetables(Reference Katagiri, Asakura and Kobayashi22).
Studies have shown that insufficient recovery from work and sleep problems predispose workers to worse health outcomes. It is possible that workers’ lifestyle habits may mediate the association between recover from work, sleep problems and health. Only a few studies have investigated the association of recuperation from work and sleep problems with dietary habits. Therefore, our aim was to determine the associations of workers’ NFR from work and sleep problems with their dietary habits in a shift-work intensive working place.
Methods
Study design and participants
The occupational health care provider for a Finnish airline company implemented a screening and prevention programme for chronic diseases in 2006(Reference Viitasalo, Lindström and Hemiö23). Of 4169 invited employees, 2312 participated in the health check-up, which consisted of diabetes risk screening, laboratory tests, physical measurements and a questionnaire on lifestyle, work and sleeping habits. At an average of 2·5 years later, the participants were invited to a follow-up health check-up which was similar to the baseline except that participants were asked to fill in a sixteen-item food intake questionnaire(Reference Hemiö, Pölönen and Ahonen24) and a measure of NFR score(Reference van Veldhoven and Broersen8). The participants’ responses to the web questionnaire were saved on the research institute database server, and only the researchers had access to the data. People with known diabetes were excluded from the study at baseline and were not invited to the follow-up study. For the present analyses, we used cross-sectional data collected at this follow-up visit. Altogether 1523 employees participated in the follow-up study and completed the questionnaires. We excluded 172 employees who had retired or stopped working for the company, six employees who had reported unreliable amounts of food, one employee with an incomplete food intake questionnaire and two employees with incomplete NFR questionnaires. The final study sample consisted of 1342 employees.
Need for recovery
We measured participants’ ability to recover from work with the validated NFR Scale(Reference van Veldhoven and Broersen8) which was earlier translated from English into Finnish and then back translated into English for wording confirmation(Reference Kinnunen, Feldt and Siltaloppi25). The scale measures the short-term adverse effect of work-day stressors and workers’ ability to recuperate from work during their free time. The NFR Scale consists of eleven items, for example, ‘I find it difficult to relax at the end of a working day’. Participants rated the items on four-point scales (1 = never, 2 = sometimes, 3 = often, 4 = always), and like in the original study(Reference van Veldhoven and Broersen8), scores were transformed into a score ranging from 0 to 100 to allow comparison with other studies. A higher NFR score indicates worse recovery from work.
Sleep
Sleep problems were identified using six questions from the Basic Nordic Sleep Questionnaire(Reference Partinen and Gislason26). The participants were advised to think of the past 3 months when answering sleep questions. The questions were as follows: 1) Have you had difficulties falling asleep? 2) How often have you awakened at night? 3) Do you feel excessively sleepy during the daytime? 4) Have you suffered from an irresistible tendency to fall asleep while at work? 5) How often have you awakened during the night without being able to fall asleep again? Subjective sleep quality was queried with a modified version of the original Basic Nordic Sleep Questionnaire question as follows: How often have you felt that your sleep is not restorative during the past 3 months? The questions were rated on a five-point scale: 1 = never or less than once per month, 2 = less than once per week, 3 = on 1–2 d/week, 4 = on 3–5 d/week and 5 = daily or almost daily. The sum of points for the six questions, ranging from 6 to 30, was used as a sleep problem score, with a higher score indicating more sleep problems. Sleep length was assessed with the question ‘How many hours a day do you usually sleep, including naps?’ Sleep apnoea was assessed with a question ‘Has a physician diagnosed that you have sleep apnoea?’ Answer options were ‘yes’ or ‘no’.
Dietary habits
We estimated participants’ dietary habits using a validated sixteen-item questionnaire(Reference Hemiö, Pölönen and Ahonen24). Validity of the food intake questionnaire has been tested earlier against 7-d food records filled by seventy-seven participants. The questionnaire asks the respondents to estimate, in daily or weekly portions, their usual consumption of sixteen different food groups (each question containing examples of portion sizes) and total number of meals and snacks per day (with examples of snacks: fruit, chocolate bar, bun, juice and beer). Of the answers of these food groups, we chose those which, based on earlier research(Reference Chaput20,Reference Torres and Nowson27) , are known to be relevant for sleep and recovery and only results for those food groups are presented here. The number of meals and snacks were categorised as follows: 1 to 2/d, 3 to 4/d, 5–6/d and 7 or more meals and snacks per day. The consumption of vegetables, fruit, desserts (e.g. sweet bakery items, ice cream, puddings and chocolate) and sweets (e.g. added sugar, honey and sweets) was rated on a five-point scale as follows: less than a portion per week or none, 1–3 portions per week, 4–6 portions per week, 1 portion per day and at least 2 portions per day. Fast food consumption was assessed using a five-point scale as follows: <1 portion per month or none, 1–3 portions per month, 1–3 portions per week, 4–6 portions per week and 1 portion per day or more. Consumption of bread and breakfast cereals and consumption of beverages were assessed with open-ended questions. The amounts of fibre-rich bread and breakfast cereals reported were changed into portions which were summed and named as grain products. We categorised grain product consumption into three categories: <2 portions per day, 2–3 portions per day and more than 3 portions per day. Of beverages, we combined sugar-sweetened juices, soft drinks and fruit juices into a group ‘sugary drinks’. We categorised sugary drinks consumption into three categories: none, 1–14 dl and more than 14 dl/week. Use of alcoholic drinks was categorised into three groups: 2 drinks/week or less, 3–7 drinks/week and more than 7 drinks/week. One drink contained 12 g of alcohol.
For the daily number of meals and snacks and for the number of portions of fast food, the two highest categories were combined because only a few responses were in those categories. In the data for women respondents, we combined the two lowest consumption categories for vegetable intake due to the low number of workers who had chosen those alternatives.
Classifications
BMI was calculated by dividing weight (kg) by height (m) squared. Education was categorised into three groups: low (comprehensive school), intermediate (secondary education) or high (polytechnic or university). Marital status was categorised into two groups: living alone and living with partner. Participants were categorised into two working time groups. Working hours between 06.00 and 18.00 hours were categorised as day work and shift work was assessed as other than day work. Occupations were categorised based on the main characteristics of the work into maintenance, customer service, in-flight work, office work and management.
Statistical methods
We used χ 2 test to analyse gender differences between categorical variables and t test between continuous variables. Pearson or Spearman correlation coefficients were assessed between NFR and sleep problems score and shift work. We used ANOVA to analyse differences between NFR (non-transformed) or sleep problem score and gender, age or working time groups and to assess differences. Ordered logistic regression, which is an extension of the logistic regression model allowing for more than two ordered response categories, was performed to examine the relationship between NFR or sleep problems and dietary habits; OR denoting the odds for falling into higher consumption category by one-point increase in the NFR/sleep problem scale. Food groups or number of meals and snacks were the dependent variables, and they were used as categorical variables in the analyses (some categories were combined, see Dietary Habits). NFR and sleep problems were the independent variables. Analyses were done separately for men and women. We adjusted analyses for the following potential confounders: age (continuous variable), education (three groups), marital status, work schedule (day work v. shift work), full v. part time work and occupational category (five groups). We chose the confounders based on the nutrition studies about which background variables typically influence dietary habits(Reference James, Nelson and Ralph28,Reference Valsta, Kaartinen and Tapanainen29) . In addition to age, education level correlates with dietary habits, where higher education predicts healthier food choices. Working time and part time work may also influence dietary habits. Occupation was chosen as a confounder based on the results of our previous analysis of the same cohort(Reference Hemiö, Puttonen and Viitasalo30). The significance level was set at α = 0·05. The analyses were performed using the statistics package Stata version 16·0 (StataCorp).
Results
The participants’ characteristics are shown in Table 1. Of participants, 737 (55 %) were men. The mean age was 47 years, and the mean BMI (kg/m2) was 26·9 in men and 25·1 in women. Men mainly worked in aircraft maintenance (51 %), office work (27 %) and management (13 %). Women did in-flight work (39 %), office work (34 %) and customer service (14 %). Among men, 57 % had a shift work schedule; among women, it was 62 %.
Table 1 Characteristics of study participants, n 1342

* <4 h weekly of leisure time low impact physical exercise.
† Working time other than between 06.00 and 18.00 hours.
‡ Sum of six sleep questions, scale range 6–30. Higher score indicates more sleep problems.
§ Sixty participants’ BMI measurements were missing.
‖ Scale range 0–100. Higher score indicates higher need for recovery from work.
Correlation coefficient was 0·57 (P ≤ 0·001) between NFR and sleep score, 0·18 (P ≤ 0·001) between NFR and shift work and 0·15 (P < 0·001) between sleep score and shift work.
The mean NFR score was higher among women than among men, 31·1 (sd 15·7) v. 27·8 (sd 15·1), P < 0·001). There was no difference in the mean NFR score by age groups (under 40, from 40 to 49, over 49 years) or by education group for either gender. For men, the mean NFR score was 25·9 (sd 15·7) for those doing day work and 29·3 (sd 14·4) for those on shift work (P = 0·002); for women, the mean score was 26·9 (sd 15·1) for those doing day work and 33·7 (sd 15·6) for those on shift work (P < 0·001).
Sleep problems differed by working time groups. Among men, the mean sleep problem score was 12·5 (sd 4·4) for those doing day work and 13·4 (sd 4·0) for those on shift work (P = 0·007). Among women, the mean score was 11·8 (sd 3·8) for those doing day work and 13·1 (sd 3·9) for those on shift work (P < 0·001).
Based on the adjusted model (age, education, marital status, day v. shift work, working full or part time and occupation), for one-point increase in the NFR scale, the OR for falling into higher category was 1·03 (95 % CI 1·00, 1·06) for eating frequency category, 0·96 (95 % CI 0·93, 0·98) for vegetable, 0·96 (95 % CI 0·93, 0·98) for fruit, 1·05 (95 % CI 1·02, 1·08) for fast food and 1·05 (95 % CI 1·02, 1·08) for sweets among men (Table 2).
Table 2 Association between need for recovery from work and dietary habits in men (n 737) and women (n 605)

* Dietary habit categories used in the analyses were as follows: number of meals and snacks: 1–2/d, 3–4/d, 5 or more per d; vegetables, fruits, desserts and sweets: <1 portion/week, 1–3 portions/week, 4–6 portions/week, 1 portion/d, at least 2 portions/d; fast food: <1 portion/month, 1–3 portions/month, 1–3 portions/week, at least 4 portions/week; grain products: <2 portions/d, 2–3 portions/d, at least 4 portions/d; sugary drinks: none, 1–14 dl/week, more than 14 dl/week; alcohol drinks: <3 drinks/week, 3–7 drinks/week, at least 8 drinks/week. OR denotes the odds for falling into higher consumption category by one-point increase in the NFR scale.
† Bold P values are statistically significant.
‡ One drink contains 12 g of alcohol.
Model 1, no adjustments.
Model 2, adjusted for education, age, marital status, day work v. shift work, full or part time job and occupation.
Among women, for one-point increase in the NFR scale, the OR was 1·06 (95 % CI 1·02, 1·09) for fast food and 1·04 (95 % CI 1·00, 1·07) for dessert consumption category based on the adjusted model (Table 2).
Among men, for one-point increase in sleep problems, the OR for falling into higher category was 1·04 (95 % CI 1·00, 1·07) for eating frequency, 0·96 (95 % CI 0·93, 0·99) for fruit and berries, 1·07 (95 % CI 1·04, 1·11) for fast food, 1·05 (95 % CI 1·01, 1·08) for sweets, 0·97 (95 % CI 0·93, 1·00) for grain products and 1·05 (95 % CI 1·01, 1·08) for alcohol consumption categories. Among women, for one-point increase in sleep problems, the OR was 1·06 (95 % CI 1·02, 1·11) for eating frequency, 1·06 (95 % CI 1·02, 1·10) for fast food and 1·04 (95 % CI 1·00, 1·08) for sweets consumption categories based on the adjusted model (Table 3).
Table 3 Association between sleep problems and dietary habits in men (n 734) and women (n 602)
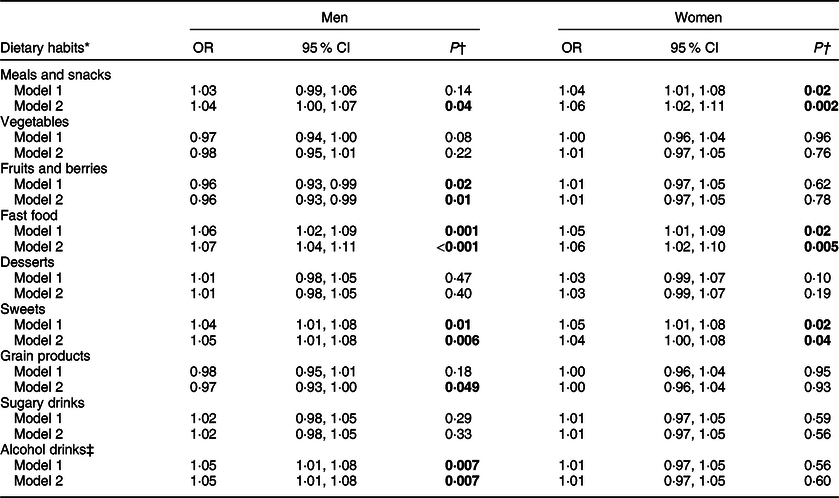
* Dietary habit categories used in the analyses were as follows: number of meals and snacks: 1–2/d, 3–4/d, 5 or more per d; vegetables, fruits, desserts and sweets: <1 portion/week, 1–3 portions/week, 4–6 portions/week, 1 portion/d, at least 2 portions/d; fast food: <1 portion/month, 1–3 portions/month, 1–3 portions/week, at least 4 portions/week; grain products: <2 portions/d, 2–3 portions/d, at least 4 portions/d; sugary drinks: none, 1–14 dl/week, more than 14 dl/week; alcohol drinks: <3 drinks/week, 3–7 drinks/week, at least 8 drinks/week. OR denotes the odds for falling into higher consumption category by one-point increase in sleep score.
† Bold P values are statistically significant.
‡ One drink contains 12 g of alcohol.
Model 1, no adjustments.
Model 2, adjusted for education, age, marital status, day work v. shift work, full or part time job and occupation.
Discussion
We studied how airline company workers’ ability to recover from work and their sleep problems were associated with dietary habits in a cross-sectional study design. The results showed that those workers, especially men, with poorer recovery from stressors of work more often chose unhealthy foods than did workers whose recovery from work was better. Similarly, sleep problems were associated with some unhealthy dietary habits.
Among men, poorer recovery from work was associated with lower consumption of vegetables and fruits and with higher consumption of fast food and sweets. In women, only the association between poorer recovery from work and higher consumption of fast food and desserts was observed. Women’s generally poorer recovery from work was not associated with their dietary behaviours as strongly as for men. We have not found any studies concerning the associations between NFR from work and dietary habits. Instead, other research has found that high work-to-family spill over, white race, being male and working in the evening predicted decreased vegetable and fruit consumption among construction workers(Reference Devine, Stoddard and Barbeau31). That study included only a few women, and finding of a gender difference in fruit and vegetable consumption can be questionable. Long working hours and poor sleep quality or inadequate sleep were associated with unfavourable food choices(Reference Mota, Waterhouse and De-Souza32,Reference Buxton, Quintiliani and Yang33) . In addition, one of these studies found that changes in sleeping patterns were associated with changes in biological markers related to central food control(Reference Mota, Waterhouse and De-Souza32). These findings provide support for our results which indicate that work-related factors might influence workers’ dietary habits, and it seems that they affect men more than women.
In the present study, correlation between NFR scale and sleep problem score was 0·57. NFR score has been shown to correlate with fatigue (r = 0·66 and r = 0·71), with emotional exhaustion (r = 0·84 and r = 0·75), with stress (r = 0·63), with physical job demands (r = 0·36), with psychological job demands (r = 0·54) and inversely with job control (r = –0·32), and NFR scale has been associated with subsequent sickness absence as well(Reference van Veldhoven and Broersen8,Reference de Croon, Sluiter and Frings-Dresen14) . In our current study, workers’ mean NRF score, 29·3, was in the same range as that in a large cohort of workers from another study (NFR = 26·7)(Reference van Veldhoven and Broersen8), but differed from the average score found in a study of day workers (NFR = 36·0)(Reference Mohren, Jansen and Kant34), and from the score found in a study of day and shift workers (NFR = 37·7)(Reference Gommans, Jansen and Stynen35). The rather low NFR in the present study may be due to the workers’ adaptation to work because of long working experience.
In the present study, proportions of those who ate fruit (men 42 %, women 69 %) and vegetables (men 57 %, women 80 %) daily were much higher than in a contemporary Finnish population-based survey where similar question about fruit (men 18 % and women 36 %) and vegetables (men 29 %, women 46 %) consumption has been used(Reference Prättälä, Paalanen and Grinberga36). Instead, in a Finnish national survey, consumption of fruits and vegetables was reported higher than in the present study, but the results were based on a consumption at least in one day of the 2-day recalls, and therefore, the results are not directly comparable with the results of daily consumption in the present study(Reference Paturi, Tapanainen and Reinivuo37). Overall, consumption of fruit and vegetables might suggest that the present study population is more health conscious than Finnish general population. The above-mentioned studies also reported similar gender differences seen in the present study, showing that women’s dietary habits are healthier than men’s.
Women’s recovery from work was inferior to that of men. This is in accordance with results from some previous studies but contradicting results have also been reported(Reference Jansen, Kant and van den Brandt10,Reference Gommans, Jansen and Stynen35,Reference Kiss, De Meester and Braeckman38) . One explanation for our finding of a higher NFR score for women could be the high proportion of women who worked shifts in our study population. Overall, our results suggest that shift workers do not recuperate from work as well as day workers do. Jansen et al. also reported that shift workers’ NFR from work was higher than that of day workers(Reference Jansen, Kant and van Amelsvoort11). Shift workers often suffer from sleep problems(Reference Flo, Pallesen and Åkerstedt39), and this presumably increases difficulties in recuperating from work. Unlike in some earlier studies, we did not observe age-related differences in mean NFR scores(Reference Mohren, Jansen and Kant34,Reference Kiss, De Meester and Braeckman38) . In our study population, the proportion of shift workers was lower in the oldest age category than in the youngest, which might explain the discrepancy with earlier findings.
We found an association between sleep problems and increased frequency of meals and snacks, increased fast food consumption and increased sweets consumption for both genders. In a Japanese study, poor sleep quality was associated with a low intake of vegetables and fish, high intake of confectionary and noodles, and unhealthy dietary habits such as irregular eating in women(Reference Katagiri, Asakura and Kobayashi22). A cross-sectional study identified an association between short sleep duration and lower fruit and vegetable consumption(Reference Stamatakis and Brownson40). Severely sleep-restricted shift workers were found to increase their snack consumption and to choose unhealthy sweet snacks more often(Reference Heath, Roach and Dorrian41). There is thus rather strong evidence that sleep-related problems increase adults’ unfavourable food choices. A possible mechanism for the association between sleep problems and unhealthy dietary habits could be hormonal. Sleep loss increases levels of the appetite-stimulating hormone ghrelin, as well as food intake and energy consumption(Reference Broussard, Kilkus and Delebecque42). Reduced sleep quality may affect the timing of insulin secretion and decrease the concentration of insulin secretion inducing glucagon-like peptide, resulting in an increased desire to eat(Reference Gonnissen, Hursel and Rutters43). The influence of sleep restriction on the hormonal regulation of food intake may also differ by gender(Reference St-Onge, O’Keeffe and Roberts44).
In the present study, we administered six questions that measured different aspects of sleep problems. NFR and sleep problems correlated highly, as expected. Because of the cross-sectional setting of the study, it was not possible to demonstrate whether poor recovery from work increases sleep problems or the other way around, and therefore we chose to present results of both. The results showed that shift workers had more sleep problems than day workers as has been reported also earlier(Reference Härmä, Tenkanen and Sjöblom45). Both insufficient recovery from work and sleep problems could be seen as indicators of poor adaptation to shift work, but including work schedule as a confounder in the model did not affect the results. We might speculate that experienced shift workers had adapted to the burden of shift work and therefore insufficient recovery or sleep problems did not particularly influence on their dietary habits.
Although disturbed sleep and insufficient recovery are typical to shift work, it is also possible that the cause-consequence order between sleep and nutrition could be two-way. A varied diet with nutritious foods such as fresh fruits, vegetables, whole grains and certain low-fat protein sources improves sleep(Reference Peuhkuri, Sihvola and Korpela46). A recent short-term clinical study indicated that nutrients may affect sleep quality. In normal-weight adults, diets low in fibre and high in saturated fat lead to less deep sleep and diets with more sugar and less fibre lead to more arousals during sleep(Reference St-Onge, Roberts and Shechter47). This finding may partly explain why in our study those who reported more sleep problems also tended to report consuming more sweets and fast food, food choices that indicate high sugar and high fat intake. This underlines a cycle rather than a linear order of events in the observed association between diet, sleep and NFR from work.
In workplace preventive interventions, both work conditions and lifestyle should be addressed. For example, recuperation from work can be improved by spending leisure time on social and physical activities(Reference Sonnentag and Zijlstra48). However, in a study by Coffeng and colleagues in which the aim was to lower the NFR from work through social and physical workplace environment interventions, none of the interventions was effective(Reference Coffeng, Boot and Duijts49). One suggested that the way of improving workers’ sleep and recuperation from work is to change work schedules so that job strain is minimised or weekly work time is reduced(Reference Härmä, Hakola and Kandolin50,Reference Schiller, Lekander and Rajaleid51) .
The present study has some limitations. The results clearly show that recovery from work, sleep problems and dietary habits are associated, but the cross-sectional study design does not reveal the direction of the effects. Therefore, the direction of the effects between NFR, sleep problems and diet should be investigated using prospective studies. Fatigue that results from insufficient recovery and disturbed sleep due to shift work can affect workers’ means of coping with daily life, which can then influence their food choices. On the other hand, poor nutrition can impair workers’ recovery from work and worsen sleep quality, increasing stress at work the next day. The data we used on NFR and sleep problems were self-reported by workers, so future studies should include objective sleep measures to confirm our results. It is possible that subjective opinion and objective data on these dimensions could show somewhat diverging associations with NFR and sleep problems. In addition, the results may not be generalisable to the working population as the airline company workers’ stressors can differ from stressors of working population without working in shifts. However, adjusting for the shift work did not affect the associations. Also, selection bias of study participants must be taken into consideration when the results are interpreted. Although the follow-up participants did not differ from non-participants in several measurements and lifestyle habits, some selection bias may have occurred.
To conclude, the present study suggests that workers’ poor recovery from work and sleep problems can negatively associate with dietary habits and therefore possibly be detrimental to health in the long term, especially among men. Therefore, in workplace interventions, dietary counselling should be included together with counselling that target better recuperation from the work day. Healthier dietary habits may also promote better sleep quality and better recuperation.
Acknowledgements
Acknowledgements: We would like to thank Esko Levälahti for valuable advice on statistical analyses. Financial support: This work was supported by the Funding Tekes – the Finnish Funding Agency for Technology and Innovation (grant 1104/10); Yrjö Jahnsson Foundation (K.H., grant 6342); Academy of Finland SALVE consortium, (grant 129518); Juho Vainio Foundation (K.H.) and Finnish Work Environment Fund (grant 108320, K.H., 180147). Any of the above-mentioned funders had no role in the design, analysis or writing this article. Conflict of interest: None. Authorship: All the authors participated in planning the study design. K.H. carried the main responsibility for data analyses and preparation of the manuscript. K.V., K.H. and S.P. participated in data collection. All the authors have revised and approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Ethics Committee of the Hospital District of Helsinki and Uusimaa. Written informed consent was obtained from all subjects.



