Many mental health, neurodevelopmental and health disorders of adulthood have their roots in childhood (Betts et al., Reference Betts, Williams, Najman and Alati2016; Copeland et al., Reference Copeland, Shanahan, Costello and Angold2009; Shonkoff et al., Reference Shonkoff, Boyce and McEwen2009; Sonuga-Barke et al., Reference Sonuga-Barke, Kennedy, Kumsta, Knights, Golm, Rutter and Kreppner2017). According to recent national surveys, the number of children affected by neurodevelopmental disorders is high, and these disorders are associated with real economic and emotional costs (Finkelstein et al., Reference Finkelstein, daCosta DiBonaventura, Burgess and Hale2010; Lynch & Clarke, Reference Lynch and Clarke2006; Robb et al., Reference Robb, Sibley, Pelham, Foster, Molina, Gnagy and Kuriyan2011). Recent meta-analyses and studies of nationally representative children show that 13% of children worldwide have at least one current psychiatric disorder (Merikangas et al., Reference Merikangas, He, Brody, Fisher, Bourdon and Koretz2010; Polanczyk et al., Reference Polanczyk, Salum, Sugaya, Caye and Rohde2015). The lifetime rates of each of these disorders at any time from childhood through adolescence substantially exceed this rate (Perou et al., Reference Perou, Bitsko, Blumberg, Pastor, Ghandour and Gfroerer2013). Similarly, prevalence rates of childhood obesity present a major public health concern, affecting more than 13.7 million children in the USA (Centers for Disease Control and Prevention, 2018). Based on the public health consequences of mental and physical health problems in childhood and adolescence, the focus of the Early Growth and Development Study (EGDS) has been to better understand their etiology through the use of a prospective ‘dual-family’ adoption study that includes linked adoptive and birth parents and children in both homes.
There is no question that environmental and genetic influences on development operate jointly to impact child development, and that there are complex interactions and correlations between these two important influences (e.g., Reiss et al., Reference Reiss, Leve and Neiderhiser2013). For example, family context and parenting processes may be moderated by genetic influences or, conversely, may moderate genetic influences. Twin, adoption and molecular genetic studies have found evidence of genotype × environment (G × E) interaction for a range of child and adolescent behavioral, mental health, cognitive and health outcomes (e.g., Brody et al., Reference Brody, Yu, Chen, Kogan, Evans, Windle and Philibert2013; Dick, Reference Dick2011; Leve et al., Reference Leve, Harold, Ge, Neiderhiser, Shaw, Scaramella and Reiss2009; Reiss et al., Reference Reiss, Plomin, Hetherington and Neiderhiser1995; Tucker-Drob et al., Reference Tucker-Drob, Rhemtulla, Harden, Turkheimer and Fask2011). In addition, there is evidence that heritable qualities in children influence their social environmental exposures through evocative and self-selection effects (Forget-Dubois et al., Reference Forget-Dubois, Boivin, Dionne, Pierce, Tremblay and Pérusse2007; Klahr et al., Reference Klahr, Thomas, Hopwood, Klump and Burt2013; McGue et al., Reference McGue, Elkins, Walden and Iacono2005; Scarr & McCartney, Reference Scarr and McCartney1983). Adoption studies have found that heritable child characteristics (e.g., behavioral impulsivity, negative emotionality) influence the parenting that children receive from toddlerhood through late adolescence (Ge et al., Reference Ge, Conger, Cadoret, Neiderhiser, Yates, Troughton and Stewart1996; Hajal et al., Reference Hajal, Neiderhiser, Moore, Leve, Shaw, Harold and Reiss2015; Harold, Leve, Barrett et al., Reference Harold, Leve, Barrett, Elam, Neiderhiser, Natsuaki and Thapar2013; O’Connor et al., Reference O’Connor, Deater-Deckard, Fulker, Rutter and Plomin1998). However, adoption studies prospectively examining social environmental processes from early childhood to adolescence are rare, with this study and the Colorado Adoption Project (Plomin & DeFries, Reference Plomin and DeFries1985) being the only such studies to date. In the adoption design, similarities between birth parents and the adopted child suggest genetic influences (attributed to shared genes and a lack of shared rearing environments) or prenatal influences (occurring in utero). Associations between adoptive parents’ and adopted children’s characteristics suggest postnatal environmental processes (based on shared rearing environments and the lack of shared genes), although evocative gene–environment correlation (rGE) effects may also cause adoptive parent–child associations.
Each type of genetically informed design has unique strengths. The adoption design’s primary strengths pertain to its ability to identify genetic influences at the whole genome, aggregate level (not specific to particular alleles), its elimination of passive rGE and its ability to detect evocative rGE. Specifically, because the adoptive parents are genetically unrelated to their adopted children, passive rGE is eliminated and associations between the birth parent(s) and adoptive parent(s) must reflect a heritable effect transmitted from birth parent to the child, which then can evoke a predicted response from the rearing parent. In twin studies and other designs where the rearing parents and child are genetically related, it can be difficult to disentangle the effects of the child’s genes from those of their parents’ when examining associations between parent and child phenotypes, and evocative rGE associations may be confounded by passive rGE effects.
Overview of the EDGS
This article provides an update on the goals, results and plans of the EGDS (see Leve et al., Reference Leve, Neiderhiser, Ge, Scaramella, Conger, Reid, Shaw and Reiss2007; Leve, Neiderhiser et al., Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013, for our initial reports). The EGDS started as a prospective adoption study designed to examine the influence of specific features of families, peers and social contexts on child adjustment, and factors that may mediate the expression of genetic influences or that may be moderated by (or moderate) genetic influences. The EGDS has since expanded to include additional children in both the birth parent and adoptive home (see Figure 1), and additional behavioral and health outcomes, as well as developmentally salient environmental exposures. By focusing on family processes beginning in infancy, the EGDS provides a unique opportunity to detect gene–environment (GE) interplay when first expressed and examine its unfolding over time.

Fig. 1. EGDS ‘dual-family’ adoption study design.
Our theoretical model was derived from research indicating family process predictors of, and continuities within, five life course developmental pathways: internalizing behavior, externalizing behavior, social competence, cognitive skills and healthy weight. The phenotypic patterns of life course development in each of these pathways are well supported by existing genetic and phenotypic data (e.g., Birch & Davison, Reference Birch and Davison2001; Caspi et al., Reference Caspi, Henry, McGee, Moffitt and Silva1995; Eisenberg et al., Reference Eisenberg, Valiente, Morris, Fabes, Cumberland, Reiser and Losoya2003; Gilliom & Shaw, Reference Gilliom and Shaw2004). To select phenotypes and associated measures to test our hypotheses, we relied on three types of studies: adoption studies to identify phenotypes that are known to be linked between birth parent and adopted child, and to also be influenced by the environment (e.g., Ge et al., Reference Ge, Conger, Cadoret, Neiderhiser, Yates, Troughton and Stewart1996); twin and sibling studies to identify phenotypes that have known genetic and environmental influences (e.g., Petrill et al., Reference Petrill, Deater-Deckard, Thompson, DeThorne and Schatschneider2006); and life course studies to identify how a phenotype might change or evolve across development (e.g., Caspi & Roberts, Reference Caspi and Roberts2001).
Although these approaches have led to substantial scientific advances in understanding the etiology of child behavioral and health outcomes, this body of research also has limitations that our study can address. For example, most sibling studies include family members who are genetically related, and most twin studies include twins reared together. Both methods can confound putative genetic and environmental effects on development. Adoption studies can address some of these concerns. In addition, most twin and sibling studies do not often permit a comparison of phenotypes across generations, and life course studies without a genetically sensitive component cannot detect whether phenotypic stability or change is based on environmental versus genetic or prenatal influences.
Considered together, however, existing adoption, twin, sibling and life course research have facilitated the formulation of data-based hypotheses about probable birth parent-adopted child phenotypic similarities and likely environmental influences on these genetically influenced phenotypes. In addition, selection of constructs and measures for some of our ongoing assessments was guided by a National Institutes of Health cooperative grant, Environmental Influences on Child Health Outcomes (ECHO; Gillman & Blaisdell, Reference Gillman and Blaisdell2018). ECHO was designed to capitalize on existing studies of children and parents and study five child outcomes: pre, peri and postnatal outcomes; obesity; airways health; neurodevelopment; and positive health.
Overall Study Hypotheses
The conceptual model for the EGDS is based on the following general hypotheses: (1) parenting behaviors, marital dynamics and peer behaviors have main effects on child adjustment (clarifying that data from prior studies of genetically related family members can be interpreted as environmental effects); (2) heritable characteristics of children evoke specific reactions and interactions from their social environment (e.g., parenting, marital relations, peer behaviors; evocative rGE); (3) environmental main effects are moderated by and moderate genetic influences (G × E), at times offsetting genetically influenced susceptibility and at times enhancing genetically influenced strengths; (4) child and parental behaviors show both change and continuity across development, with child behavioral continuity associated with both environmental and genetic influences and the continuity of parenting behavior partially influenced by children’s heritable characteristics; and (5) the environmental context enhances the effects that genetically influenced child behaviors have on parenting practices (e.g., genetically influenced effects of child characteristics on parenting may only appear in certain contexts; moderation of evocative rGE). In this model, we hypothesize specific mediating and moderating mechanisms on adjustment along five developmental pathways: externalizing behavior, internalizing behavior, social competence, academic and school performance and weight trajectories.
Figure 2 illustrates the interrelation of the studies and the developmental periods covered. EGDS-Toddlers (n = 361) focused on infancy and toddlerhood and is considered Cohort I of EGDS. EGDS-Prenatal is considered Cohort II of EGDS; it expanded EGDS-Toddlers by adding 200 new cases, adding buccal cell collection for candidate gene analyses and focusing specifically on the role of prenatal influences. EGDS-School was designed to continue assessments of the EGDS-Toddlers participants through the school entry period, with additional data collection on school readiness, academic achievement and stress reactivity (measured by salivary cortisol collection). EGDS-NIMH focused specifically on child and adoptive parent mental health symptoms and diagnoses and included Cohort I and II children. EGDS-Health examined pathways to healthy weight and obesity through the assessment of children’s and parents’ health-promotive behaviors (e.g., diet, physical activity, sleep) within Cohort I and II families. EGDS-Middle School (MSCH) continued assessment of the original Cohort I children as they entered middle school. Early Parenting of Children (EPoCh) began as a separate study designed to assess the original birth families who were parenting a 7-year-old sibling of the original Cohort I or II adoptee. Finally, EGDS-ECHO1 was designed to collect data on all original EGDS and EPoCh children, and on all additional siblings aged 0–20 years who were living in either the adoptive or birth home. It served as the precursor to ECHO2, which is now underway and is further described in the Future Plans section of this article. The Future Plans section also describes a second ongoing study with the Cohort I and II adoptees that is focused on pubertal development and hormonal influences on child outcomes (EGDS-ADOL). With the exception of ECHO2 and EGDS-ADOL, assessment activities for the studies shown in Figure 2 are complete.
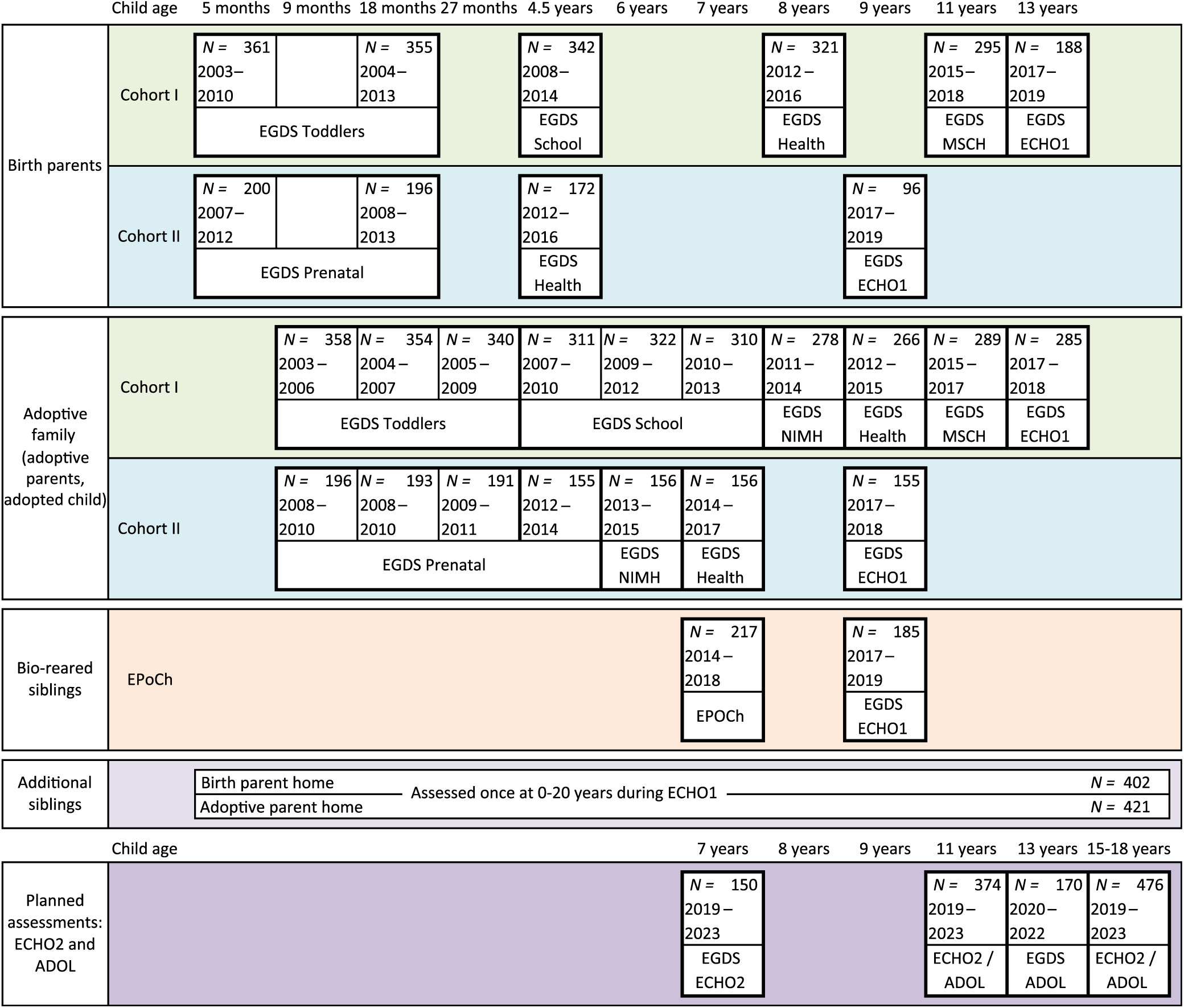
Fig. 2. Timeline for the EGDS studies and assessments.
Sample Description
The EGDS sample includes 561 linked sets of participants: 561 adopted children, their birth mothers (n = 554), their birth fathers (n = 210) and their adoptive parents (562 adoptive fathers and 569 adoptive mothers; numbers do not sum to 561 mothers/fathers because the sample includes 41 same-sex parent families, and 11 additional adoptive fathers and 3 additional adoptive mothers who entered the family after the original couple adopted the child, recruited in 2 cohorts. More than half of the children are male (57.2%), and 55.3% of the children are Caucasian, 19.6% are multiracial, 13.2% are Black or African American, 10.9% are Hispanic or Latinx, <1% are Asian, <1% are Native Hawaiian or Pacific Islander, <1% are American Indian and <1% are of unknown ethnicity/not reported. The median child age at adoption placement was 2 days (M = 5.58, SD = 11.32; range = 0–91 days). When the study expanded as part of EPoCh and ECHO, siblings living in the original birth and adoptive homes were recruited. Of the siblings recruited into the study, 13% (n = 135) were a full sibling to the adoptee, 43% (n = 435) were a half sibling to the adoptee and 43% (n = 430) were unrelated to the adoptee. Cohort I and II adopted children’s birth dates ranged from January 2003 to May 2009, EPoCh children’s birth dates ranged from December 2005 to May 2012 and the ECHO additional siblings’ birth dates ranged from August 1996 to December 2018.
Demographic information regarding parent age, race, ethnicity, education, marital status and income is provided in Table 1. Cohort differences were examined for all demographic variables, and negligible differences were identified. As is indicated by these demographic statistics and was noted in our prior publication (Leve, Neiderhiser et al., Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013), EGDS shows the typical pattern of differences in sociodemographic characteristics often found between birth and adoptive parents, with adoptive parents having substantially more advantaged socioeconomic backgrounds than birth parents (DeFries et al., Reference DeFries, Plomin and Fulker1994). In addition, it is notable that birth parents’ highest education level completed and household income levels have continued to rise since the start of the study, as would be expected based on their younger age at the time of recruitment into the original study.
Table 1. Sample demographics

a Includes Asian, Native Hawaiian/Pacific Islander, American Indian/Alaskan Native and unknown.
b Mean education level calculated with a 7-point scale ranging from 1 (<high school degree), 2 (GED), 3 (high school degree), 4 (trade school), 5 (2 year’s college), 6 (4 year’s college), to 7 (graduate program).
c Includes marriage, remarriage and living together in a committed marriage-like relationship.
d Statistically significant difference between cohorts at p < .01.
Sample Recruitment and Design Assumptions
Staff at four recruitment sites recruited families in the Mid-Atlantic, the West/Southwest, the Mid-West and the Pacific Northwest regions of this USA into the study. Recruitment of Cohort I and II birth and adoptive families occurred between March 2003 and January 2010, beginning with the recruitment of adoption agencies into the study (N = 45 agencies in 15 states). EGDS participants currently reside in 46 states, the District of Columbia in the USA, and in 12 other countries. The project employs separate birth parent and adoptive family recruiters to ensure that project staff do not transfer information between members of the adoption triad. We maintain this separation through all stages of the study, including assessment. In collaboration with the study, each adoption agency appointed a liaison from their organization to perform the initial stages of recruitment into the study.
Agency liaisons identified participants who completed an adoption plan through their agency and met the study’s eligibility criteria: (a) the adoption placement was domestic, (b) placement occurred within 3 months postpartum, (c) the infant was placed with an adoptive family that was not biologically related to the child, (d) there were no known major medical conditions such as extreme prematurity or extensive medical surgeries and (e) the birth and adoptive parents were able to understand English at the eighth-grade level. All types of adoptive families were eligible for study enrollment (e.g., same-sex parents, single parents and hearing-impaired parents). Once eligibility criteria were met, 2 to 4 weeks postplacement, the agency liaison mailed a letter describing the study to each eligible adoptive family. Adoptive families were given the opportunity to opt out of future study contact by returning a self-addressed, stamped postcard. Two weeks after the mailing, liaisons called the birth mothers linked to the adoptive families that had not opted out of the study to describe the study and ask for permission to have a recruiter from the study to contact them directly. If birth mothers provided permission for EGDS to contact them, the EGDS birth parent recruiter contacted the birth mother. Next, the EGDS adoptive family recruiter attempted to recruit the adoptive family using the contact information provided by the agency. Finally, after the birth mother and adoptive parents were recruited, project staff attempted to recruit the birth father. See Leve, Neiderhiser et al. (Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013) for recruitment details and a flowchart of the recruitment procedures for Cohort I and II families.
For EPoCh, the eligibility criteria included: (a) birth mother enrolled in EGDS between 2003 and 2009 following the birth of the EGDS adoptee, (b) birth mother was parenting a biological sibling of an EGDS Cohort I or II adoptee and (c) this biological sibling was born between 2005 and 2012. The EPoCh participants were recruited at biological sibling age 7 from an eligible pool of n = 287 children. Of the eligible participants who were not enrolled into EPoCh; 8% were unable to be located; 5% declined participation; 3% were not recruited because the parent was incarcerated, deceased or the child was removed from the home; 5% verbally agreed to participate but never completed the assessment; and 4% were not recruited because the study ended. Birth parents participating in EPoCh had similar demographic characteristics (race, ethnicity, income and education) as the full sample of EGDS birth parents, with the exception that they were significantly younger, t(398) = 4.385, p < .001, than the full sample, likely due to the study inclusion criteria (parenting a 7-year-old child at the time of recruitment).
For ECHO1, eligibility criteria included: (a) birth and adoptive parents enrolled in EGDS between 2003 and 2009 following the birth of the EGDS adoptee, (b) family had not previously withdrawn from the study (n = 32 adoptive families and 13 birth families), (c) parents were not deceased (n = 16 birth families) and (d) the original Cohort I adoptee, Cohort II adoptee, EPoCh sibling or additional children aged 0–20 years were living in the home. Recruitment resulted in a sample of n = 283 Cohort I adoptees, n = 154 Cohort II adoptees, n = 190 EPoCh siblings, n = 421 additional children in the adoptive family home and n = 402 additional children in the birth family home.
To assess sampling bias in the recruitment of the original sample of birth and adoptive families, we compared the demographic information between triads who participated in the EGDS (N = 561 triads) with those of the eligible nonparticipants (N = 2391 triads available for analysis) using data available from the participating agencies. We found minimal systematic sampling biases, suggesting that the EGDS sample is generally representative of the population from which it was drawn (see Leve, Neiderhiser et al., Reference Leve, Neiderhiser, Shaw, Ganiban, Natsuaki and Reiss2013, for details).
The adoption design rests on several assumptions about the separate influences of genetic and environmental influences on child development. For example, once intrauterine factors such as prenatal alcohol and drug consumption, maternal depression and stress, and exposure to environmental toxins have been considered, similarities between the birth parent and the adopted child are inferred to result from genetic factors. Trends in adoption practices such as openness (contact and knowledge between birth and adoptive families) and selective placement (agency matching of birth and adoptive parent characteristics) can pose a threat to these assumptions and can bias model estimates. For example, adopted children may be more likely to resemble their birth parents (inflating genetic estimates) when birth parents are in direct contact with the child. Thus, we examined the variation in two aspects of the adoption process — openness and selective placement — with our sample of 561 linked EGDS families.
The level of openness was measured by asking birth parents and adoptive parents to report on the amount of contact and knowledge between them. Responses were categorized into seven discrete categories: very closed (no information about the adoptive parents or birth parents), closed (only general information that the agency provided), mediated (written communication only, conducted through an agency), semiopen (exchange of letters and emails, cards and pictures, but no face-to-face contact), open (visits one to three times per year and communication semiregularly by telephone, mail or email), quite open (visits about every other month and frequent communication by telephone, mail or email) and very open (visits at least once monthly and communication several times a month by telephone, mail or email). The prevalence of birth and adoptive parents’ ratings for each level of openness during infancy and at their most recent assessment is shown in Table 2. Results show that there are a range of openness levels and indicate that the level of openness has generally declined as the children age. In addition, birth mothers, adoptive mothers and adoptive fathers are generally in strong agreement about the level of openness (r = .71–.84; Ge et al., Reference Ge, Natsuaki, Martin, Leve, Neiderhiser, Shaw and Reiss2008). We include a composite measure of openness in EGDS papers in order to account for this potential confound, although in the majority of papers to date, it has not been significantly associated with most study predictors or outcome variables.
Table 2. Self-reported level of openness in the adoption at the start of the study (before slash) and last report (after slash)

Note: AP = adoptive parent, BM = birth mother, BF = birth father.
To test for selective placement, we correlated birth parent characteristics with adoptive family characteristics that were unlikely to be influenced by evocative effects (e.g., scales of personality, self-worth, executive function, temperament, intelligence and financial needs). Of 132 comparisons, only 3 were statistically significant at p < .05. Thus, systematic selective placement biases typically have not been detected in the EGDS sample.
Data Collection
Measurement for the EGDS has been guided by five principles: adherence to a theoretical model guiding the domains of assessment between parents and children, utilization of a multimethod multiagent assessment strategy, use of identical or developmentally comparable measures across assessments to facilitate the examination of change over time, the meticulous separation of research staff collecting data from birth families from those collecting data from adoptive families and repeated assessment of birth parents to attempt to fully capture genetic influences on development through the reduction of measurement error in the birth parent assessments.
Overview of Assessment
The completed EGDS assessments included questionnaires, in-person interviews, and standardized testing for birth parents, adoptive parents and children; diagnostic interviews with adoptive parents (about themselves and about the adopted child), with birth parents about themselves and with EPoCh birth parents about their child; observational interactions (mother–father, mother–child, father–child and mother–father–child) for all adoptive families and for EPoCh birth families; food and activity diaries for adoptive families; medical records for birth parents and the adopted and birth children; DNA collection via buccal cells for adoptees, adoptive parents and birth parents and from saliva for EPoCh children; diurnal cortisol measures for adopted children, EPoCh children and birth parents; teacher questionnaires for EGDS and EPoCh children; and official arrest records for birth parents. The interviews included interviewer-administered questions, which created a context whereby the interviewer could establish rapport with the participant, and computer-assisted personal interviews that were completed privately by participants to facilitate confidentiality and honest responses. In-person assessments (adoptive family: age 9 months, 18 months, 27 months and age 4.5, 6, 7 and 8 years; birth parents: 5 and 18 months’ postpartum and 4.5 years’ postpartum; and age 7 years for EPoCh families) lasted approximately 3–4 h each and were conducted in a location convenient for the participant, most often at home.
Brief telephone interviews (15 min) were conducted for birth and adoptive parents in between the primary in-person assessments. These served as a means of maintaining contact and rapport with participants. Overall, 208 different assessment measures have been administered focusing on the primary theoretical model and aims. A full listing of study measures by age is available at https://egdstudy.org/measures/. De-identified data that are part of ECHO’s common measures will also ultimately be shared on a secure portal for access by the broader research community. Currently, we share existing de-identified data with external colleagues throughout the USA and Europe. Procedures for accessing de-identified data are available from the corresponding author and include receipt of a signed data security policy and submission of a detailed project abstract. Our study’s publication policy provides guidelines for approval of new projects, review timelines and authorship.
Summary of Results
Table 3 provides a summary of some of the main areas that have been examined and a sampling of some of the publications in each area. We continue to place an emphasis on examining environmental influences on child temperament, behavior problems and psychopathology (General Hypothesis 1), with expansion to areas such as peer relations (Elam et al., Reference Elam, Harold, Neiderhiser, Reiss, Shaw, Natsuaki and Leve2014; Leve et al., Reference Leve, Griffin, Natsuaki, Harold, Neiderhiser, Ganiban and Reiss2019) and child obesity and health (Blackwell et al., Reference Blackwell, Elliott, Ganiban, Herbstman, Hunt, Forrest and Camargo2019; Marceau, Abel et al., Reference Marceau, Abel, Duncan, Moore, Leve, Reiss and Ganiban2019). Our findings regarding General Hypothesis 1 indicate main effects of parenting (overreactive parenting, responsivity, parenting efficacy and observed structured guidance), marital hostility and adoptive parent depressive symptoms (including adoptive fathers) and anxiety on child temperament, behavior and psychopathology outcomes across infancy, toddlerhood and childhood. We also published a review paper on the environmental association between maternal depression and child development (Natsuaki et al., Reference Natsuaki, Shaw, Neiderhiser, Ganiban, Harold, Reiss and Leve2014). Many of our empirical papers have used longitudinal data and utilized coded observational data on parents or parents and children, where available, to reduce self-report and within-rater bias issues (e.g., Hyde et al., Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Leve2016; Roben et al., Reference Roben, Moore, Cole, Molenaar, Leve, Shaw and Neiderhiser2015). In addition, many of our analyses have included both adoptive mothers and fathers, with results typically showing unique effects of fathers (e.g., Bridgett et al., Reference Bridgett, Ganiban, Neiderhiser, Natsuaki, Shaw, Reiss and Leve2018; Hails et al., Reference Hails, Shaw, Leve, Ganiban, Reiss, Natsuaki and Neiderhiser2018; Harold, Leve, Elam et al., Reference Harold, Leve, Elam, Thapar, Neiderhiser, Natsuaki and Reiss2013). Although the main effects of parenting, marital function and parent psychopathology are not new to the field of psychology, EGDS is able to show that associations between these family characteristics and child psychosocial adjustment are not attributable to passive rGE, and that they can be detected across childhood.
Table 3. Manuscript content areas and sampling of representative manuscripts in each area

General Hypothesis 2 examines evocative rGE. As the children in EGDS move out of early childhood and into middle childhood, we are seeing evidence of evocative rGE (e.g., Harold, Leve, Barrett et al., Reference Harold, Leve, Barrett, Elam, Neiderhiser, Natsuaki and Thapar2013, Klahr et al., Reference Klahr, Burt, Leve, Shaw, Ganiban, Reiss and Neiderhiser2017). We also have numerous examples of child effects on a parent characteristic (e.g., Ahmadzadeh et al., Reference Ahmadzadeh, Eley, Leve, Shaw, Natsuaki, Reiss and McAdams2019), although in the absence of a significant path from a birth parent variable to the child variable, we cannot determine whether these child effects are genetically mediated. We have sought to identify evocative rGE associations in some of our analyses and failed to detect a genetic signal. These null findings could be for several reasons, including: (a) we may not have identified or measured the relevant birth parent variable, including possible incongruence between an adult phenotype and a child phenotype, (b) evocative effects may not appear until later in child development, (c) evocative effects may be masked by interaction effects, as moderated mediation (see Fearon et al., Reference Fearon, Reiss, Leve, Shaw, Scaramella, Ganiban and Neiderhiser2015, as an example), (d) we only have birth father data for approximately one-third of our sample and thus are missing a portion of the potential genetic influences, (e) the child variables we have examined may not show intergenerational genetic transmission or (f) the genetic influences involved are nonadditive. Regardless of the source of the lack of consistent evocative effects, we will continue to test hypothesis-driven questions about evocative rGE as the sample enters adolescence in the coming years.
General Hypothesis 3 examines environmental moderation of genetic influences and genetic moderation of environmental influences (G × E). We have found significant G × E effects during infancy, toddlerhood and middle childhood for several types of child behavior, including externalizing problems, total behavior problems and callous-unemotional behavior (e.g., Hyde et al., Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Leve2016; Leve et al., Reference Leve, Harold, Ge, Neiderhiser, Shaw, Scaramella and Reiss2009; Lipscomb et al., Reference Lipscomb, Leve, Shaw, Neiderhiser, Scaramella, Ge and Reiss2012; Roos et al., Reference Roos, Fisher, Shaw, Kim, Neiderhiser, Reiss and Leve2016), attention behavior (Brooker et al., Reference Brooker, Neiderhiser, Kiel, Leve, Shaw and Reiss2011; Leve, Kerr et al., Reference Leve, Kerr, Shaw, Ge, Neiderhiser, Scaramella and Reiss2010), fussiness and anger (Natsuaki et al., Reference Natsuaki, Ge, Leve, Neiderhiser, Shaw, Conger and Reiss2010; Rhoades et al., Reference Rhoades, Leve, Harold, Neiderhiser, Shaw and Reiss2011), inhibition (Natsuaki, Leve, Neiderhiser et al., Reference Natsuaki, Leve, Neiderhiser, Shaw, Scaramella, Ge and Reiss2013) and positive peer relations (Van Ryzin et al., Reference Van Ryzin, Leve, Neiderhiser, Shaw, Natsuaki and Reiss2015). We have also found G × E interaction effects on children’s cortisol regulation (Laurent, Leve, Neiderhiser, Natsuaki, Shaw, Harold et al., Reference Laurent, Leve, Neiderhiser, Natsuaki, Shaw, Harold and Reiss2013). Our G × E findings may reflect the fact that in adoption designs, we assess how environmental factors moderate the genetic transmission of parental phenotypes to their children at the age of child measurement. In contrast, twin designs examine the degree to which environmental factors moderate the heritability of a child trait as the time of measurement. These methodological differences may explain the different patterns of G × E findings between the two approaches.
General Hypothesis 4 requires measurement of longitudinal pathways of continuity and change across development in relation to genetic and environmental influences. Our analyses suggest fairly high stability of child behavior, temperament, parenting behavior and marital behavior across early and middle childhood (e.g., Ahmadzadeh et al., Reference Ahmadzadeh, Eley, Leve, Shaw, Natsuaki, Reiss and McAdams2019; Lipscomb et al., Reference Lipscomb, Leve, Harold, Neiderhiser, Shaw, Ge and Reiss2011; Liu et al., Reference Liu, Moore, Beekman, Perez-Edgar, Leve, Shaw and Neiderhiser2018; Mannering et al., Reference Mannering, Harold, Leve, Shelton, Shaw, Conger and Reiss2011; Trentacosta et al., Reference Trentacosta, Waller, Neiderhiser, Shaw, Natsuaki, Ganiban and Hyde2019), and indicate that changes in parenting are associated with changes in child behavior (Lipscomb et al., Reference Lipscomb, Leve, Shaw, Neiderhiser, Scaramella, Ge and Reiss2012; Trentacosta et al., Reference Trentacosta, Waller, Neiderhiser, Shaw, Natsuaki, Ganiban and Hyde2019). As the study children enter adolescence, which is a period of significant change in the youth’s social world that requires new parenting strategies, we will continue to examine stability and change in children’s developmental trajectories to examine developmental windows that may be more or less susceptible to environmental influences, and thus garner insights for prevention or intervention development. General Hypothesis 5 — to examine moderation of evocative rGE effects — has only been examined in one paper to date (Fearon et al., Reference Fearon, Reiss, Leve, Shaw, Scaramella, Ganiban and Neiderhiser2015), with findings suggesting that genetic factors associated with birth mother externalizing psychopathology may evoke negative reactions in adoptive mothers in the first year of life, but only when the adoptive family environment is characterized by marital problems; favorable marriages facilitate positive parental reactions to the same heritable traits. As this study focused on very early childhood, future work will continue to test moderated mediation and mediated moderation as the children enter adolescence.
Overall, the findings to date contribute in novel ways by showing that family environmental variables (e.g., parenting, parental psychopathology and marital relations) are associated with child adjustment outcomes even when passive rGE effects are removed, and that specific G × E effects can be detected across early and middle childhood. We have some evidence for evocative rGE effects, although such effects have been less prominent than originally hypothesized. The DNA collected as part of EGDS Prenatal was genotyped for a select set of specific genes, consistent with the standards of the time. More recently, in 2018–2019 in EPoCh, we sequenced salivary DNA samples from a subset of children using Illumina microarray technology. We currently have several manuscripts in process using the genotyped data from both studies. Results from our dual-family adoption study are just one source of knowledge about the interplay between genetic and environmental influences on development; there is a need to synthesize findings across multiple design types. As described next, our participation in NIH’s ECHO project is one of our newest efforts to increase the rigor and reproducibility of findings on child behavioral and health outcomes.
Future Plans
Our data collection activities during childhood (EPoCh), late childhood (Cohort II) and early adolescence (Cohort I) were very recently completed. Accordingly, we will continue to examine our original study aims and hypotheses across development, using longitudinal approaches and data from children in Cohort I and II and their siblings, where available. We are particularly interested in testing whether evocative rGE effects become more prominent during adolescence when youth spend more time outside of the family context. We are also interested in identifying environmental influences that help children have positive health outcomes, despite having genetic or prenatal liabilities. We are developing methods to test sibling models that examine rearing and genetic influences based on the complex and nested nature of siblings of different ages residing in two different homes that vary on sociodemographic features (e.g., Natsuaki et al., Reference Natsuaki, Neiderhiser, Harold, Shaw, Reiss and Leve2019), and who vary in genetic relatedness to additional children in the home (ranging from sharing no genes for unrelated siblings, to sharing 50% for full siblings and dizygotic twin pairs, to sharing 100% for monozygotic twin pairs).
To pursue these objectives, in addition to continuing to analyze our existing data, we are engaged in two new studies that will include new data for the original EGDS children and their siblings during adolescence. First, in a new study that will assess the Cohort II children at ages 11, 13 and 15, and Cohort I children at age 15, we will explore the interplay among genetic influences, prenatal experiences, pubertal development and postnatal environment on children’s risk for substance use. This study (EGDS-ADOL) includes the collection of hair samples to measure pubertal hormones and cortisol, and questionnaires for the youth and their parent(s) that measure adolescent behavioral and health outcomes, including substance use and related behaviors, and the family and contextual environment.
Second, as noted earlier, we are part of NIH’s ECHO program and will be collecting data in collaboration with other pediatric cohorts across the USA to learn about early environmental influences on children’s neurodevelopment; positive health; airways health; pre, peri and postnatal outcomes; and obesity. Approximately 500 of our adoptees and EPoCh children and 500 of their siblings will complete in-home and web-based assessments at age 7, 11 or 15, depending on the current age of the child, as part of EGDS-ECHO2. In addition to measures of child behavior and health, and of the family and contextual environment, this study will collect a number of biospecimens, including saliva (for genotyping), blood spots, hair, shed teeth, toenail clippings, stool and urine that together can be used to provide genetic data and index chemical exposures. Our sample of approximately 1000 children will be part of the larger ECHO aggregate sample of approximately 50,000 children and families. Data will be harmonized across cohorts, and ultimately shared in a de-identified manner with the broader scientific community for access by independent researchers. We are eager to embark on this collaborative effort and to make de-identified data from this study available to a broader range of researchers.
Acknowledgments
We thank the birth and adoptive parents who participated in this study and the adoption agencies who helped recruit study participants. Special gratitude is given to Rand Conger, John Reid, Xiaojia Ge and Laura Scaramella who contributed to the original study aims; to Sally Guyer for data management; to study coordinators, recruiters, data teams and assessors; and to our collaborators and coauthors who developed and tested hypotheses using study data.
Financial support
This project was supported by R01 HD042608, NICHD, NIDA and OBSSR, NIH, U.S. PHS (PI Years 1–5: David Reiss; PI Years 6–10: Leslie Leve), R01 DA020585 NIDA, NIMH and OBSSR, NIH, U.S. PHS (PI: Jenae Neiderhiser), R01 MH092118, NIMH, NIH, U.S. PHS (PIs: Jenae Neiderhiser and Leslie Leve), R01 DK090264, NIDDK, NIH, U.S. PHS (PI: Jody Ganiban), R01 DA035062, NIDA, NIH, U.S. PHS (PI: Leslie Leve), R56 HD042608, NICHD, NIH, U.S. PHS (PI: Leslie Leve), and UG3/UH3 OD023389, Office of the Director, NIH, U.S. PHS (PIs: Leslie Leve, Jenae Neiderhiser and Jody Ganiban). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Eunice Kennedy Shriver National Institute of Child Health & Human Development, the Office of the Director, or the National Institutes of Health.
Conflict of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.