


Introduction
The prevalence of disablement following traumatic brain injury (TBI) is well known,Reference Dawson and Chipman 1 – Reference Corrigan, Cuthbert and Harrison-Felix 3 and of increasing concern as we now recognize that several sequelae can persist and worsen in the chronic stages.Reference Corrigan, Cuthbert and Harrison-Felix 3 – Reference Wilson, Stewart and Dams-O’Connor 5 One longitudinal study found that in the first 5 years following injury 39% of individuals had deteriorated in global functioning, 55% were unemployed, and about 30% were not independent in performing activities of daily living.Reference Corrigan, Cuthbert and Harrison-Felix 3 Indeed, TBI has been described as a chronic condition, with a potential for lifelong activity limitations and participation restrictions. Moreover, level of function is not static and can deteriorate with time post injury.Reference Wilson, Stewart and Dams-O’Connor 5 Decline in functioning has been attributed to psychosocial factors, co-morbidities, aging, or to neurodegenerative processes.Reference Green, Colella, Maller, Bayley, Glazer and Mikulis 6 , Reference Corrigan and Hammond 7 For example, atrophy in at least one brain region in the first 2 years post injury was observed in 95% of participants in one study.Reference Green, Colella, Maller, Bayley, Glazer and Mikulis 6 Because TBI is now recognized as a chronic condition,Reference Corrigan and Hammond 7 and in the context of limited research dollars, researchers and funding agencies agree that setting priorities with the aim of maximizing well-being for survivors and their families is critical.Reference Wilson, Stewart and Dams-O’Connor 5 The purpose of this paper is to describe the process and results of a summit held in 2016 with Canadian experts in TBI to formulate research priorities. The aim of reporting these data is to highlight the priority research areas needed to optimize the long-term community integration for individuals with TBI, and to illustrate a methodology to identify research directions.
Traumatic brain injury may affect all aspects of a person’s functioning, including the physical, cognitive, emotional, and social spheres. Developing research priorities is thus essential because of the breadth of support needs and multiplicity of important research directions. For instance, current research in TBI addresses epidemiology,Reference Roozenbeek, Maas and Menon 8 health service needs and usage,Reference Jaglal, Guilcher and Bereket 9 consequences of TBI in terms of functioning, community integrationReference Corrigan, Cuthbert and Harrison-Felix 3 and individuals’ views of self,Reference Levack, Kayes and Fadyl 10 and the nature and efficacy of specific healthcare and/or rehabilitation service models and interventions.Reference Zitnay, Zitnay and Povlishock 11 The latter category can be further divided according to interventions that aim to remediate or compensate for impairments in emotional, physical, cognitive, communication and/or behavioral functioning,Reference Cicerone, Langenbahn and Braden 12 medical management of TBI,Reference Zitnay, Zitnay and Povlishock 11 and interventions designed to enhance participation in everyday life (e.g., meta-cognitive strategy training,Reference Dawson, Binns, Hunt, Lemsky and Polatajko 13 vocational rehabilitation,Reference Wehman, Kregel and Keyser-Marcus 14 and social services such as affordable and supportive housing, income supports, and accessible transport).Reference Jaglal, Guilcher and Bereket 9 It is also essential to consider the needs of family caregivers who play a vital role in facilitating long-term community integration.Reference Nalder, Fleming, Cornwell and Foster 15
Given the limits in terms of funding and resources for research, it is critical to prioritize the many potential research directions that could be pursued to optimize the long-term community integration of individuals with TBI and their caregivers, as they both age. A recent review paper synthesizing evidence on long-term outcomes and chronic neurological changes following TBI called for more research to examine how neurological functioning and participation change over time. Such information is essential to identify potential targets for intervention, and guide researchers to develop and evaluate interventions that may improve community integration.Reference Wilson, Stewart and Dams-O’Connor 5 We were given an opportunity by two Canadian provincial organizations to identify research priorities that could ultimately be pursued by an interdisciplinary TBI research team on the theme optimizing long-term community integration. This team consisted of clinicians, decision-makers, TBI survivors and caregivers, and over 40 top Canadian researchers in the field of TBI, and the funders’ vision was to promote collaboration and innovation by allowing the team to work on a common research agenda.
The first step toward identifying research priorities for our team was to engage stakeholders in discussions around the theme to identify potential research directions. Stakeholder meetings are specifically effective at engaging members of the community and identifying research questions that reflect their priorities,Reference Graham, Kothari and McCutcheon 16 and are an important component in efforts to develop research agendas designed to influence policy and practice.Reference Restall, Carnochan, Roger, Sullivan, Etcheverry and Roddy 17 In addition, using stakeholder meetings to set research priorities is viewed as a method for reducing research waste and fostering innovation by promoting collaboration and knowledge exchange across researchers in different disciplines or fields.Reference Chalmers, Bracken and Djulbegovic 18
There are a few examples of research agendas published in relation to TBI, but to our knowledge none explicitly focus on long-term community integration. Some address specific topics, such as homelessnessReference Topolovec-Vranic, Ennis and Ouchterlony 19 or the needs of women with TBI,Reference Harris, Colantonio and Bushnik 20 whereas others are more global looking at all aspects of TBI.Reference Zitnay, Zitnay and Povlishock 11 One of the first published examples of a consensus activity to identify research priorities specific to TBI occurred in 2005.Reference Zitnay, Zitnay and Povlishock 11 The Conemaugh International Brain Injury Symposium brought together over 100 neuroscientists, and other associations and professionals, involved in the rehabilitation and treatment of individuals with TBIReference Zitnay, Zitnay and Povlishock 11 to review progress made in research over the preceding decade, and to make recommendations to government on the priority areas for TBI research moving forward. The committees formulated research priorities in four areas: basic science, acute care, post-acute rehabilitation, and improving quality of life. The basic science group identified mechanisms of progressive brain injury and therapeutic discovery and development as two priorities for further study, and the acute care and post-acute teams called for more clinical trials to determine the efficacy of interventions, noting the paucity of level I evidence. Participants at this meeting also identified a need for more precise assessment tools to measure outcomes, and for studies looking at comparative effectiveness and cost-effectiveness of different models of interventions.Reference Zitnay, Zitnay and Povlishock 11 As over 10 years has passed since this symposium, and more is now known regarding the chronic nature of TBI, it is timely to review and update research priorities for TBI.
In sum, our broad objective was to formulate research priorities with the most potential for improving the long-term community integration of individuals with TBI and their family caregivers. Our specific objectives were (1) to identify the primary challenges to optimal long-term community integration that are encountered by survivors, their families, and caregivers; (2) to identify potential short-term (2 years) and longer-term initiatives (5 years) that will address these barriers to community integration; and (3) to synthesize and prioritize these initiatives into specific research priorities.
Methods
Design
A 2-day stakeholder meeting was arranged, using the World Café Methodology—a conversational method designed to engage large groups in conversation around important issues to catalyze change,Reference Sheridan, Adams-Eaton, Trimble, Renton and Bertotti 21 and used, in other contexts, to generate research priorities.Reference Restall, Carnochan, Roger, Sullivan, Etcheverry and Roddy 17 This type of conversational method is effective in promoting interdisciplinary collaboration, fostering innovation and creative thought, and enhancing the relevance of research, by asking end-users about their priorities.Reference Sheridan, Adams-Eaton, Trimble, Renton and Bertotti 21 , Reference MacFarlane, Galvin and O’sullivan 22 A team grant in TBI research provided by two provincial organizations was used to fund the 2-day meeting.
The World Café method involves groups of people discussing a topic of importance to them. Participants change groups, so that they discuss the issue with different people. The method is based on a social constructivist paradigm, whereby knowledge is viewed as socially constructed through interactions with others.Reference Sheridan, Adams-Eaton, Trimble, Renton and Bertotti 21 Key principles for hosting a World Café discussion are as follows: (1) create a hospitable space; (2) explore questions that matter; (3) encourage everyone’s contribution; (4) connect diverse people and ideas; (5) listen together for insights, patterns, and deeper questions; and (6) make collective knowledge visible.Reference Brown and Isaacs 23 The specifics of how we implemented this method to develop research priorities follows.
Participants
We used purposeful snowball sampling to identify a diverse group of participants (n=54) with broad expertise for the 2-day summit. Researchers who were part of existing inter-provincial TBI research teams in Ontario and Quebec were first invited, and they invited others from their networks including researchers, persons living with TBI, and persons working for community-based TBI organizations, specifically Brain Injury Canada, the Ontario Brain Injury Association, the Quebec Association for Individuals Living with Traumatic Brain Injury, and the Quebec Rehabilitation Research Network. Graduate students and post-doctoral fellows working with researchers were also invited. The resulting team (see Table 1 for details of participants, n=54) comprised a broad range of professionals, stakeholders, and individuals with lived experience with expertise in occupational therapy (n=15), psychology (n=13), physical medicine and rehabilitation (n=3), medicine (n=4), service delivery/administration (n=3), computer science (n=3), speech and language pathology (n=3), biomechanics (n=2), case management (n=2), epidemiology (n=2), neuroscience (n=2), nursing (n=2), physical therapy (n=2), and social work (n=1). In addition, there were two representatives from Brain Injury Associations: one individual with lived experience and one caregiver. Further, several participants held leadership roles on TBI advisory boards and professional associations that influence policy and service delivery, and several of the researchers were engaged in work to synthesize current best evidence and produce clinical practice guidelines for the management of mild TBI,Reference Marshall, Bayley and McCullagh 24 and rehabilitation in moderate-to-severe TBI.Reference Bayley, Tate and Douglas 25 Each team member attended either one (n=24) or both meetings (n=15), or, if unable to attend in person, provided input via email (n=15, all researchers).
Table 1 Participants involved in formulating the research priorities*

*Some participants had more than one role; hence, the totals do not add up to n=54, which was the total number of participants engaged in the process.
Procedure
The stakeholder meeting was held over 2 days in February and April 2016 in Canada. The first day involved multiple group conversations to identify a broad range of challenges pertaining to long-term community integration and potential solutions to these issues. The second day was used to refine this list, reach consensus on priorities, and develop a research agenda. The 2 days were not held consecutively so that participants had time to further reflect on the discussions before formulating research priorities.
Day 1
The meeting began with a series of presentations illustrating ongoing research on TBI in Canada. Of note was a presentation of key findings from a recent national survey in Canada, designed to identify research gaps in relation to TBI and spinal cord injury rehabilitation and recovery from the perspective of individuals living with these conditions. Priority research topics identified in this survey were improving mood and cognitive function, understanding the functioning of the brain, housing, and enhancing community living skills. After these initial presentations, small groups of ~9 individuals per group discussed the barriers to community integration and short- and longer-term initiatives that could address these barriers. Group discussions were based around a key question (see Table 2). Questions were developed before the meeting by the meeting chairpersons (DD, IG) and adapted from questions used in published stakeholder meetings using the World Café Methodology.Reference Restall, Carnochan, Roger, Sullivan, Etcheverry and Roddy 17
Table 2 Key questions guiding the small-group discussion

TBI=traumatic brain injury.
Three 35-minute group conversations occurred simultaneously, each led by a facilitator and addressing one of the three questions. The facilitators were team members and received instruction before the summit regarding how to structure the conversations. Following each conversation, participants moved to another room, to discuss a different question, with a different group of people. After the three small-group conversations, the facilitators presented a summary of the major ideas that had emerged to the reassembled, whole group. The summit chair then facilitated a town-hall-style discussion in which emerging ideas were grouped together into broad themes. Themes were recorded on flip chart paper, and then placed on the walls around the room forming a visual gallery of the key themes derived through the conversations.
To reach consensus, we used a voting procedureReference Rankin, McGregor and Butow 26 to prioritize these themes. Each participant was given six stickers and asked to place them on the theme or themes they perceived were most important to improving the community integration of individuals with TBI. Each sticker represented one vote and participants could assign multiple votes to a theme as they wished. After the meeting a list of the identified themes was sent to those participants who were not able to attend in person and they allocated their six votes to a theme (or themes) via email. Because there were fewer participants from community-based organizations, or with lived experience of TBI, these individuals (n=4) each received 12 votes to give them more influence.
A small group of researchers with experience in qualitative methods and/or who were involved in the overall planning and organization of the meeting (DD, CB, IG, EN, and KZ) met to tabulate the votes and develop definitions of each theme using a qualitative content analysis.Reference Hsieh and Shannon 27 This involved re-reading all the flip chart notes to increase familiarity with the data, coding the data, and theorizing the relationships between codes and the themes identified during the meeting on day 1. Codes were thus used to define the themes, ensuring internal validity (content all related to a core idea) and external validity (delineating conceptual boundaries between the themes identified). The thematic summary and tabulated votes were sent to all participants via email and discussed on day 2 of the meeting.
Day 2
The second full-day meeting was facilitated by the summit chairpersons (DD and CB). The day began with three small groups of ~9 participants, each with a facilitator, reviewing the thematic summary developed from the discussions on day 1, to decide whether they agreed with the identified themes, and to group similar themes together. Everyone then reconvened to listen to and discuss each group’s ideas for grouping themes, and to collectively decide on the two or three most important research priorities for our team.
Results
Research themes—initiatives to improve long-term community integration after TBI
The themes that emerged using the World Café Methodology (day 1) and the number of votes they each received are listed in Table 3. On day 2, consensus was achieved for combining the 12 themes into three priority areas for research (all focused on moderate-to-severe TBI): (1) optimizing functioning through individualized intervention; (2) supporting caregiver needs; and (3) using technology as a driver of care (see Figure 1). Two cross-cutting themes also emerged that were viewed as important for our team’s work in all three of these research areas, namely knowledge translation (KT) and enhancing the lens of TBI as a chronic condition. An explanation of each of these research priorities follows.
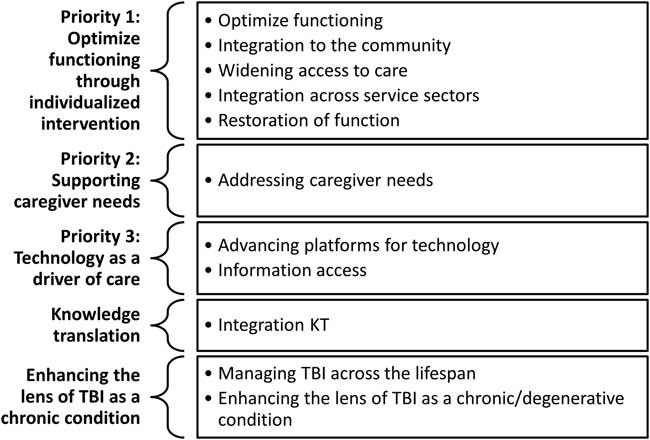
Figure 1 Prioritized research directions and their relationship to the themes emerging from the World Café discussions.
Table 3 List of themes describing challenges and strategies to optimal long-term community integration following TBI

KT=knowledge translation; TBI=traumatic brain injury.
Optimizing functioning through individualized intervention
The first research priority reflected the need for work to develop, evaluate, and implement interventions that would optimize the functioning and participation of individuals with TBI, and prevent relapse or deterioration in function over time. Some key discussion points related to this research priority included the need for (1) developing and evaluating the psychometric properties of ecologically valid assessments that can be used to evaluate intervention efficacy and monitor functional changes arising in the context of individuals’ daily life; (2) identifying and evaluating self-management interventions to maintain physical, psychological, and cognitive functioning; (3) understanding the critical characteristics of supported housing for individuals with TBI who may need to transition from the family home into alternative accommodation as caregivers age; and (4) producing evidence of real-world effectiveness of interventions, through information on how specific interventions influence participation in unstructured and changing environments more like real life, and by evidence that the skills acquired in therapy can be transferred to other tasks and contexts. Themes from day 1 of the World Café discussion initially separated interventions targeting the individual from those targeting aspects of the environment. However, the group felt that intervention research should consider the complex relationships between individuals and environments and how each influences the other over time.
Supporting caregiver needs
The second research priority was supporting caregiver needs. Key discussion points related to this research priority included the following: (1) the need to better understand the experiences of aging caregivers providing support to someone with TBI in the home, and how their needs change over time and across contexts (e.g., during residential transitions, or as individuals go into respite care); (2) the importance of developing and evaluating individualized interventions that would reduce caregiver burden, in particular case management, respite services, social support, strategy training, and education; (3) the need to evaluate the cost-effectiveness of interventions that would improve caregiver well-being and family functioning; and (4) the importance of recognizing that families have complex needs including observing improvements in the functioning of their relative or friend with TBI. Thus, in addition to examining interventions targeting the caregiver, it will also be important to explore how interventions targeting the functioning and participation of individuals with TBI influence caregiver burden.
Technology as a driver of care
The third research priority was to explore how emerging technology platforms could be used to complete assessments, deliver interventions, or support the everyday functioning of individuals with TBI and/or their caregivers in the home and community. Key discussion points related to this research priority included the need to (1) develop and evaluate telehealth platforms and/or centers for intervention delivery, and examine whether they improve access to health and rehabilitation services for individuals with TBI; (2) understand the utility of technology to monitor body functions and/or participation patterns of individuals with TBI and provide this information to individuals or health professionals in a manner that can support self-management; (3) investigate the role of technology in supporting individuals with TBI and their caregivers to navigate the healthcare system, and more easily identify services to meet their needs, and coordinate different services and providers; (4) develop apps or websites to facilitate KT and inform end-users (e.g., professionals, individuals, and families) about the quality of evidence related to specific interventions or assessments; and (5) identify ethical aspects of technology use (e.g., choice, risk, and autonomy) and barriers to implementation of technology-mediated interventions with individuals with TBI so that those who need technology for community integration can access and use it. It was noted that not all individuals with TBI have access to technology platforms, or perhaps more importantly to the Internet, and thus the need to develop partnerships between industry, research, and service providers that could begin to address barriers to uptake of technology-mediated interventions.
Cross-cutting themes: KT and enhancing the lens of TBI as a chronic condition
A cross-cutting theme of KT emerged reflecting the need to identify and address evidence to practice gaps, and to develop, evaluate, and implement knowledge-translation interventions to ensure that interventions with best evidence are used in practice. Key discussion points related to this cross-cutting theme included the following: (1) the potential value of developing community–research partnerships, as this is suggested to increase the likelihood that research evidence can be applied in practice.Reference Kothari and Wathen 28 The impact of these partnerships on evidence-informed decision-making should also be studied; (2) the need for targeted exchange of knowledge across sectors to promote integrated care for individuals with TBI (e.g., between brain injury and mental health services); (3) the need for high-quality knowledge syntheses in each of our prioritized research areas (interventions to optimize functioning and participation, supporting caregivers, and the use of technology to drive care) was viewed as a vital step to facilitating KT.
Another cross-cutting theme that emerged was the need to advance the understanding of TBI as a chronic and long-term condition in order to address some of the systemic challenges of limited access to long-term care and support to enable community integration. Key discussion points related to this cross-cutting theme included the following: (1) when developing interventions, it may be beneficial to review existing evidence generated in other populations with chronic illness (e.g., in relation to self-management and caregiver needs); (2) there is a need to advocate and apply consistent language so that TBI is understood as a chronic condition rather than an acute condition; and (3) understanding and evaluating funding and service models that provide care across the life span.
Discussion
The broad objective of this study was to formulate research priorities with the potential for improving the long-term community integration of individuals with TBI and their family caregivers. To achieve this broad goal, we used the World Café Methodology in a 2-day stakeholder meeting. The primary questions that were addressed in the first day revolved around the identification of current realities that individuals with TBI and their families are confronted with, and which strategies have a higher probability of improving the lives of individuals with TBI and their families in the long term, according to experts’ own experiences or research programs, and their knowledge of existing evidence related to TBI. The second day of stakeholder discussion revolved around the identification and prioritization of strategic research directions. Many potential directions for research emerged through the process, and as per the request from our funder to develop a collaborative research network working on a common research agenda, we synthesized these into three priority areas: optimizing functioning through individualized intervention, supporting caregiver needs, and using technology as a driver of care. It was interesting to note that although we began this process with experts working in mild and moderate-to-severe TBI, the consensus-building process narrowed the focus to research addressing the needs of those with moderate-to-severe injuries and their caregivers.
The World Café Methodology engaged experts in TBI rehabilitation including individuals from different disciplines engaged in research, service management/design, and frontline delivery of rehabilitation for individuals with TBI, as well as caregivers and individuals living with TBI. The team included participants from two provinces in Canada, which allowed for more nuanced considerations of how potential research projects could be carried out and ultimately influence two different healthcare systems. The varied expertise of participants ranged from basic science to clinical rehabilitation and enabled a breadth of issues that individuals who are living with TBI experience, to emerge through the process. In addition, the stakeholder meeting allowed for the identification of links between different research areas and opportunities for collaboration, and provided a voice to individuals working in TBI associations whose role is to advocate for individuals and families living with TBI.Reference MacFarlane, Galvin and O’sullivan 22 The breadth of expertise among participants in this 2-day meeting allowed for the identification of strategic priorities that cannot be addressed only by researchers in one discipline, and can potentially lead to new innovations as participants with very different backgrounds learn and problem-solve during their conversations.
Optimizing function and the need for evidence-based real-world interventions
The theme of optimizing functioning through individualized intervention was a very broad theme reflecting the need for intervention in many areas, such as enhancing physical/psychological/cognitive and behavioral functioning, optimizing inclusion and participation, and preventing decline with aging, as well as systems-level interventions that would widen access to care. The need for intervention research aligns with the literature, as recent systematic reviews and clinical practice guidelines in brain injury rehabilitation consistently note the lack of evidence demonstrating the efficacy and cost-effectiveness of rehabilitation interventions.Reference Bayley, Tate and Douglas 25 , Reference Kumar, Samuelkamaleshkumar, Viswanathan and Macaden 29 Moreover, other published research agendas for individuals with TBI, including the Conemaugh symposium, have called for a focus on research to develop and evaluate interventions.Reference Zitnay, Zitnay and Povlishock 11 Taken together, these findings suggest that producing evidence of intervention effectiveness is a continuing priority.
Although our team identified a need for intervention work in many different areas, there was a commonly identified theme, specifically the need for evidence of real-world effectiveness. This is in line with increasing evidence that highlights the importance of designing contextualized interventions that involve tasks and activities representative of everyday life,Reference Dawson, Binns, Hunt, Lemsky and Polatajko 13 , Reference Bayley, Tate and Douglas 25 and developing ecologically valid outcome measures.Reference Dawson, Anderson, Burgess, Cooper, Krpan and Stuss 30 , Reference Bottari, Dassa, Rainville and Dutil 31 Developing ecologically valid assessments and evidence of their reliability, validity, and responsivity is essential so that they can be used as outcome measures in intervention studies. This will enable researchers to draw conclusions about whether the intervention being studied and any improvements observed correspond with performance in daily life, and not just reflect performance in a controlled, clinical environment.Reference Burgess, Alderman and Forbes 32
Supporting caregiver needs
Supporting caregiver needs was another priority research direction. Representatives of the community-based organizations identified aging caregivers as experiencing major stressors when considering long-term community integration. Many of the challenges for caregivers that were identified in the stakeholder meeting were consistent with existing evidence pertaining to the experiences of caregivers of individuals with TBI, in particular the high levels of caregiver burden,Reference Ponsford, Olver, Ponsford and Nelms 33 lack of access to community services and supports, and the high levels of stress during transitions of care.Reference Kitter and Sharman 34 , Reference Minnes, Woodford, Carlson, Johnston and McColl 35 Although some qualitative evidence exists describing the perceptions of aging caregivers regarding their support needs,Reference Kitter and Sharman 34 , Reference Minnes, Woodford, Carlson, Johnston and McColl 35 these studies typically occur at one point in time, and lack detail regarding the contextual factors influencing caregivers’ experiences and how they change over time as they and the individual with TBI age.
A recent systematic review demonstrated that there is limited high-quality evidence from randomized controlled trials regarding how to intervene to alleviate caregiver burden,Reference Baker, Barker, Sampson and Martin 36 perhaps owing to the multiplicity of intervention strategies and factors contributing to caregiver burden. This supports the research direction identified within this stakeholder meeting that was to focus on developing, evaluating, and implementing interventions to alleviate caregiver burden, and to include caregiver outcomes as a secondary measure in trials evaluating interventions targeting the functioning of individuals with chronic TBI.Reference Baker, Barker, Sampson and Martin 36 , Reference Fisher, Lennon, Bellon and Lawn 37
The potential promise of new technology
The potential promise of new technology platforms within the context of optimizing long-term community integration of individuals living with a TBI was unanimously identified as a priority direction for further research. In fact, the group discussion highlighted numerous ways in which these new technologies could widen access to care, improve patient monitoring and system navigation, and support research and education. However, rigorous research is required to determine the benefits and also the limits of how technology can be applied.
Technology in the form of mobile applications, wearable sensors, and sensor networks is increasingly being explored to support the management of complex health conditions in the community.Reference Wilson and Maeder 38 In parallel, the emergence of generic commercial applications (e.g., smartphone apps) that promote health, and management of daily tasks, has also been widely accepted by the general public. One of the major areas in which technology is being used in general is to support self-management particularly of adults with chronic health conditions through self-monitoring of functioning, and the remote delivery of interventions (either in a self-directed or therapist-delivered manner using videoconferencing).Reference Aalbers, Baars and Rikkert 39 Within the context of TBI, however, the primary focus of technology-based interventions pertains to the use of assistive technology as a cognitive aid and to support the performance of activities of everyday living.Reference DuBois, Di Giovanni, Chui and Nalder 40 , Reference Teasdale, Emslie, Quirk, Evans, Fish and Wilson 41 Preliminary research has demonstrated the initial promise of telerehabilitation to serve as a tool to deliver rehabilitation and improve caregiver self-management.Reference Damianakis, Tough, Marziali and Dawson 42 , Reference Ng, Polatajko, Marziali, Hunt and Dawson 43 Smart home technologies have also shown much promise in optimizing independence and safety in the home for individuals with cognitive deficits.Reference Olivares, Giroux and De Loor 44 However, there still remains a need to fully explore the potential of the different types of technology and their optimal application, as well as the limitations of this method of delivering care. This work to enhance the evidence for technology driving care for individuals with TBI requires interdisciplinary input to produce innovation, to ensure that technologies can be implemented effectively and integrated within existing practices and systems, and to address complex ethical issues that accompany the increasing application of technology in healthcare.
Cross-cutting themes
Knowledge translation emerged as a cross-cutting idea, perhaps related to the fact that all three of our identified priorities focus on intervention development and evaluation, with the long-term goal of moving knowledge outputs into clinical practice. One strategy identified through the World Café discussions for enhancing KT was having integrated models where researchers work with end-users, or as part of service organizations.Reference Kothari and Wathen 28 Collaborative applied research with community members has been shown to influence evidence-informed decision-making among healthcare professionals, and is increasingly being requested by research funders;Reference Graham, Kothari and McCutcheon 16 however, to our knowledge, these models have not yet been evaluated in the context of TBI. A possible direction for our team moving forward is to evaluate the impact of our research partnership involving academics, service providers, and persons with lived experience, on key indicators of KT (e.g., evidence-informed decision-making).
The final cross-cutting theme reflects the need to consider TBI as a chronic condition when developing and evaluating interventions and advocating for system-level changes. This aligns with accumulating evidence that demonstrates that functioning after TBI is not static, and that both deterioration in functioning and brain atrophy have been observed over time.Reference Corrigan, Cuthbert and Harrison-Felix 3 – Reference Green, Colella, Maller, Bayley, Glazer and Mikulis 6 Traumatic brain injury is therefore considered to be a chronic condition, and that, similar to other chronic illnesses, interventions should be focused on how to monitor functioning, developing, and evaluating lifestyle interventions that can support self-management, and at a system level provide access to supports, and the flexibility to match services to needs over the life span.Reference Wilson, Stewart and Dams-O’Connor 5 , Reference Jaglal, Guilcher and Bereket 9
Limitations
As the process of forming research priorities was driven through consultation and engagement of a purposeful sample of stakeholders, in one context, there is a potential that important perspectives from stakeholders that were under-represented, or from other contexts may have been omitted. Thus, the three directions presented do not represent the only priorities for research in TBI but rather the areas prioritized by our team. In particular, there was only one caregiver and one individual with lived experience of TBI involved in the current process, so the perspectives of survivors and families may have been under-represented, and we had a large number of participants from occupational therapy and psychology, meaning the weight given to their perspective may have been stronger than other professions with less representation (e.g., social work, recreation therapy). However, TBI association members were included and they work directly with individuals and families on a daily basis as advocates for their needs.
We were requested by our funding body to identify two or three research priorities related to a broad theme (optimizing long-term community integration). We approached this using the World Café method, which draws out experts’ perspectives of strengths and gaps in the literature. This approach has been recommended to enhance the relevance of the research to end-users, and to promote collaboration and reduce duplication.Reference Chalmers, Bracken and Djulbegovic 18 , Reference MacFarlane, Galvin and O’sullivan 22 Stakeholder consultation focuses on expert opinion, and reviews of the existing literature should also be part of developing research priorities. To ensure that current literature was considered throughout the 2-day summit, we began the stakeholder meeting with a series of presentations summarizing current research related to the theme (health services and systems, mild TBI, community integration in moderate-to-severe TBI). In addition, subsequent to this stakeholder meeting, members of our group have initiated systematic reviews of the literature related to the priority areas that were identified in this meeting—specifically, reviewing evidence for interventions to alleviate caregiver burden, and describing how technology is used in TBI rehabilitation.
Conclusion
In a 2-day summit, involving researchers, clinicians, individuals with TBI and their caregivers, and representatives from Brain Injury Associations, research priorities were developed with the goal of optimizing the long-term community integration of individuals with TBI. Prioritized directions for research were developing interventions to optimize functioning and evaluating their effectiveness in real-world contexts, supporting caregivers, and using technology to drive care. The results of this summit provide a guide for stakeholders in research and government on target areas for research funding, and may foster interdisciplinary study, by bringing together a diverse group of stakeholders to collaboratively form research priorities.
Acknowledgments
The authors thank all members of the ONF-REPAR research team who participated in this process of formulating research priorities, as well as Yarden Levy, Denise Dubois, and Lisa Engel who helped to compile data from the 2-day meeting for analysis.
Statement of Authorship
EJN and KZ drafted the paper with input from all authors. DRD, CLB, and IG conceptualized the summit, and developed the agenda and questions guiding the discussions using the World Café Methodology. EJN, KZ, BJM, SM, and AWH facilitated group conversations within the summit. All authors participated in the summit meeting, and in subsequent discussions to analyze the data, helped to edit the manuscript, and read and approved the final paper, before its submission.




