



The modern day food environment in high- and middle-income countries is characterised by the widespread availability and persistent marketing of ultra-processed food and non-alcoholic beverages that are high in fat, sugar and/or salt (HFSS). Concerns have been raised about the implications of such marketing (commercial promotion that includes not only advertising but also product placement, sponsorship, product design/packaging and point-of-sale promotions(1)) for children’s health(Reference Swinburn, Sacks and Hall2–4). Exposure to HFSS advertising has a direct effect on children’s food behaviours and diet-related health(Reference Cairns, Angus and Hastings5–Reference Smith, Kelly and Yeatman9). Youths of lower socio-economic status (SES) may have greater exposure to HFSS advertising(Reference Adams, Tyrrell and Adamson10–Reference Fleming-Milici and Harris12) and be more vulnerable to the effects(Reference Kumanyika and Grier13,Reference D’Alessio, Laghi and Baiocco14) relative to those of higher SES. Similarly, greater impact of advertising on food intake has been seen in children with overweight and obesity(Reference Russell, Croker and Viner15).
Debate has tended to focus on the promotion of energy-dense foods and whether this contributes to the development of childhood overweight(Reference Swinburn, Sacks and Hall2,Reference Norman, Kelly and Boyland8) , but studies have also noted that children’s food advertising exposure is large for items potentially harmful to their dental health(Reference Al-Mazyad, Flannigan and Burnside16). Whilst the global epidemic of obesity, including in children, and its economic cost is well documented(4,Reference Wang and Beydoun17,Reference Ng, Fleming and Robinson18) , prevalence of dental caries has arguably received less attention(Reference Fisher, Selikowitz and Mathur19) despite being recognised as a global public health concern by the WHO(Reference Petersen20). Untreated dental decay in primary teeth affects 560 million children worldwide(21). Dental disease is associated with increased rates of school absenteeism(Reference Agaku, Olutola and Adisa22) and work absenteeism by parents or guardians(Reference Ribeiro, Gomes and de Lima23), with the direct costs of treatment alone estimated at US$298 million annually (4·6 % of total global health expenditure)(Reference Fisher, Selikowitz and Mathur19).
Evidence suggests that obesity and dental caries are related(Reference Hayden, Bowler and Chambers24), and although both are multifactorial in their aetiology, a common risk factor is the excessive consumption of sugar(Reference Swinburn, Sacks and Hall2,Reference Selwitz, Ismail and Pitts25) . In 2015, the WHO published updated guidelines on sugar intake, recommending that both adults and children should reduce their intake of free sugars to <10 % of total energy intake, and ideally <5 % (approximately 25 g (six teaspoons/d))(26).
However, the role of food marketing in driving chronic overconsumption of sugar in children and the associated dental consequences is unclear. There are some cross-sectional studies that suggest an association. For example, children who watch more television have been found to consume more soft drinks and have poorer oral hygiene(Reference Anand, Suresh and Chandrasekaran27) or to be more likely to consume cariogenic foods and have dental caries(Reference Silva, Duarte and de Oliveira28,Reference Ghimire and Rao29) than those who watch less.
Numerous experimental studies show that television advertising for unhealthy foods in general increases immediate snack food (both sweet and savoury) intake in children(Reference Boyland, Nolan and Kelly6). However, there is a dearth of experimental evidence in relation to the impact of high-sugar (cariogenic) food and beverage (hereafter, food) advertisements specifically or how intake of sweet items is affected. Gatou et al.(Reference Gatou, Mamai-Homata and Koletsi-Kounari30) showed that following food advertisement exposure (v. non-food), children chose significantly fewer healthy foods from a photograph-based checklist and those with poor dental health in particular chose a higher percentage of unhealthy foods. However, to our knowledge, no studies have used solely and specifically cariogenic food advertisements (rather than general HFSS products) as the experimental stimuli and included actual energy/sugar intake as an outcome measure. In addition, there is insufficient understanding of the potential moderating role of individual differences such as dental health, weight status and SES in this effect. The current study was designed to address these gaps.
The primary hypotheses were that all children would consume a greater amount of food overall (energy) and sugar specifically (g) following food advertisement exposure relative to non-food advertisement exposure. The secondary hypothesis was that this increase in intake would be greatest for those children with dental caries experience, overweight or obesity, and/or lower SES.
Patients and methods
The research was conducted according to the Declaration of Helsinki. Ethical approval was obtained from the University of Liverpool Research Ethics Sub-committee for Non-invasive Procedures in January 2016 (RETH000945). Written informed consent was obtained from the school head teacher and parents. Verbal child assent to participate was also obtained. Parents were asked to indicate any history of anaphylaxis, food allergy or intolerance to the foods to be used in the study, these children would have been excluded from participating but no such cases were reported.
Participants
A total of 101 children (forty male) aged 8–10 years (mean 9·86 (sd 0·54) years) were recruited from a primary school in Merseyside, UK. The power calculation for the current study was based on 80 % power and a two-sided significance level (α) of 0·05 to find a medium effect size for the food intake effect (our primary hypothesis) (d = 0·3, reflecting previous short-term advertising exposure studies(Reference Boyland, Nolan and Kelly6)). This indicated a required sample of ninety participants; however, this was an opportunity sample with about 10 % over recruitment included to allow for potential attrition (e.g. school absence). Data were collected during May and June 2016.
Design
The study design was adapted from similar studies previously conducted by the researchers(Reference Boyland, Harrold and Kirkham31,Reference Halford, Gillespie and Brown32) . Participants were exposed to four food advertisements or four non-food advertisements (all approximately 30 s long for a total advertisement exposure of 2 min, embedded within the same 21-min episode of the TV cartoon ‘Scooby Doo’) on two different occasions (each at a similar time of day) on a large projector screen in a spare school classroom. Counterbalancing of condition order was conducted using www.randomizer.org. A 2-week interval between conditions was enforced to minimise the crossover effect from each exposure, and children were asked (via instructions to parents in the information sheet and reminder information sent prior to the study sessions) to keep other activity (e.g. breakfast consumption and physical activity) consistent on test days and the 24 h prior. The food advertisements all promoted high-sugar food and beverage items (snacks, confectionery and sugar-sweetened beverages), and the non-food advertisements were for toys. All advertisements were obtained from contemporary UK television recordings held by the researchers.
Procedure
Children were asked to indicate their level of hunger on a ‘smiley face’ five-point Likert scale (adapted from a similar scale(Reference McGale, Halford and Harrold33)). Participants then viewed the stimuli (cartoon with food/non-food advertisements embedded in the middle) in small groups (4–8 children). Groups were held consistent across the two testing sessions, and each child always participated on the same day of the week and at the same time of day.
Following advertisement exposure on each occasion, children were each given an individual, standardised tray of pre-weighed snack foods and beverages. The items offered were chosen to represent options with a range of sugar content to allow variations in expression of food choice (towards or away from sweeter items) to be assessed (see Table 1). Orange juice was selected as the high-sugar drink (rather than a sugar-sweetened carbonated beverage or cordial-based drink) for reasons of (i) minimising provision of nutrient-poor items to children and (ii) experimental control (avoiding inconsistency in drink fizziness and individual preferences around strength of cordial dilutions). As evidence suggests that food advertising operates at a category (e.g. sugary drinks) level, rather than an individual product level(Reference Cairns, Angus and Hastings5), using a familiar and liked item was perceived as an appropriate option despite fruit juice typically being advertised to children less frequently than carbonated beverages.
Table 1. Nutritional composition of the test food and drink items*
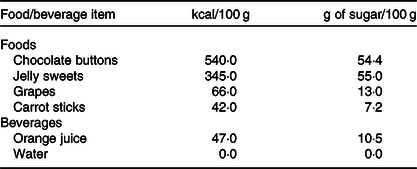
* To convert kcal to kJ, multiply by 4·184.
The food items were removed from all packaging and placed in plain white bowls. The beverages were provided in clear bottles with no labelling and a sports cap to prevent spillages. The children were allowed 15 min to eat and drink as much or as little as they wanted. They could, on request, receive more of any item. After 15 min, the trays were collected. The remaining items were weighed, and subsequent calculations determined the amount of each item consumed and the overall energy and sugar intake.
At the end of the second session, a dental examination was undertaken by two UK General Dental Council registered dentists (J. K. and R. F.). As children of this age are at different stages of dental development, only first permanent molars were examined. The dental examination involved a visual inspection under using a high-powered head-torch (Energizer Vision HD + Focus headlight- 300 Lumens). A disposable mirror and probe (Kerr TotalCare, sterile dental mirror and periodontal probe) were used to explore the tooth surfaces. Any decayed, missing or filled teeth were noted and a Decayed, Missing, Filled Teeth (DMFT) score was recorded. DMFT is a long established and commonly used method of assessing dental caries prevalence(Reference Klein, Palmer and Knutson34). Where possible, children were assessed by both dentists independently (sixty-six children were assessed by both dentists and the remainder by one dentist (J. K.)). Inter-examiner reliability was calculated for DMFT. Also at the second session only, children’s height (m) and weight (kg) were measured using a stadiometer (Leicester Portable Height Measure: SECA) and digital scale accurate to 0·2 kg (SECA 875 Flat Scales). These data were not obtained for two children.
Statistical analysis
DMFT scores, representing experience of dental caries, were converted to a dichotomous ‘present’ (DMFT score of 1, 2, 3 or 4 indicating experience) or ‘absent’ (DMFT score of 0, no experience). BMI was calculated using height and weight data, and weight status was defined using cut-off points equivalent to adult BMI of 25 kg/m2 (overweight) and 30 kg/m2 (obese)(Reference Cole, Bellizi and Flegal35). Due to disparities in weight status group sizes, children with overweight and obesity were combined into a single ‘overweight/obesity’ group for analysis purposes. Parents provided the child’s home postcode, which was used to calculate the Index of Multiple Deprivation using the English indices of deprivation 2010 as markers of SES(36). Using this tool, participants were assigned to one of the five quintile groups ranging from ‘least deprived’ to ‘most deprived’.
Data were analysed using IBM® SPSS® Statistics version 24 and SAS software version 9.4. Cohen’s kappa statistic was used to calculate the inter-examiner reliability of the duplicated dental examinations, this was 0·87 for DMFT with an observed agreement of 96·97 %. The effect of advert type on overall intake of energy and sugar was analysed using repeated-measures mixed models, adjusting for the fixed effect of sequence (first or second) and random effect of group allocation. Differences in the effect of advertisement exposure in groups based on caries experience, weight status and SES were explored by adding these variables and interaction terms to the models. All models were fitted using PROC MIXED in SAS.
Results
Table 2 lists demographic and anthropometric characteristics of the completing participants. The levels of overweight and obesity recorded in the sample were broadly consistent with national statistics(37). This was a relatively deprived sample, with 89·1 % of participants falling into the two most deprived quintiles, and the proportion of children with caries experience (19·8 %) was relatively low in comparison with UK national data(Reference Pitts, Chadwick and Anderson38).
Table 2. Characteristics of completing participants
(Numbers and percentages)

DMFT, Decayed, Missing, Filled Teeth.
* Does not equal 100 % due to rounding.
† No weight or height data obtained for two study participants.
A paired t test showed that hunger did not differ significantly across the two sessions (P > 0·05), so this variable was not included in further analyses.
Overall intake
On average, children consumed a greater amount of energy following food advertisement exposure compared with after toy advertisements (see Table 3). The difference between advertisement types in least squares means adjusted for group and sequence was 203·3 (95 % CI 56·5, 350·2) kJ (48·6 (95 % CI 13·5, 83·7) kcal) (P = 0·007). The difference in adjusted means for sugar consumption was 6·0 (95 % CI 1·3, 10·7) g (P = 0·012). These increases largely reflect greater consumption of chocolate and jelly sweets (the items with the greatest sugar content) following the food advertisements relative to the toy advertisements (see Table 3). No significant differences in drink consumption (drink choice or volume consumed) were seen between conditions.
Table 3. Sugar (g) and energy (kcal) intake of individual items across advertisement conditions†
(Mean values and standard deviations)
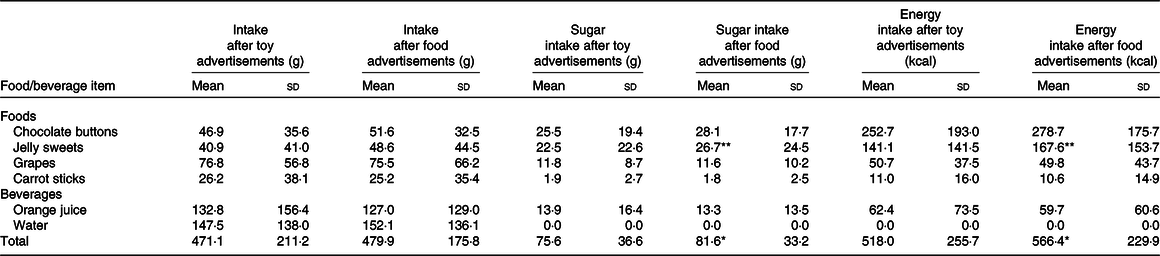
** P < 0·01, * P < 0·05; results from paired t tests between toy and food conditions using actual means (data in text of results section are estimated least squares means from the model adjusting for group and sequence).
† To convert kcal to kJ, multiply by 4·184.
Intake and experience of dental caries
There was a significant interaction between advertisement exposure and experience of dental caries on energy intake (P = 0·044). Adjusted mean differences in intake between food and toy advertisements were 129·7 (95 % CI –31·4, 291·2) kJ (31·0 (95 % CI –7·5, 69·6) kcal) in those without caries experience and 503·3 (95 % CI 177·4, 829·3) kJ (120·3 (95 % CI 42·4, 198·2) kcal) in those with caries experience. Sugar consumption also showed a statistically significant interaction effect (P = 0·030), with adjusted mean differences of 3·5 (95 % CI –1·6, 8·6) g in those without caries experience, and 16·2 (95 % CI 5·9, 26·5) g in those with caries experience.
Intake and weight status
The energy intake of children with overweight and obesity was slightly lower in the food advertisement condition relative to the toy advertisement condition (difference in adjusted means of –101·3 (95 % CI −413·0, 210·5) kJ (–24·2 (95 % CI −98·7, 50·3) kcal)), and the interaction term from the repeated-measures mixed model showed the difference in response between that group and those of a healthy weight (who showed an adjusted mean increase in intake of 278·7 kJ (66·6 kcal) after food advertisements) was statistically significant (P = 0·037). Similarly, children with overweight and obesity consumed slightly less sugar after food advertisements than after toy advertisements (adjusted mean reduction of 2·8 (95 % CI –12·8, 7·1) g), but there was no statistically significant difference (P = 0·060) in response when compared with those children of a healthy weight (who showed an adjusted mean increase in sugar intake after food advertisements of 8·1 (95 % CI 2·8, 13·3) g).
Intake and socio-economic status
Inclusion of SES in the models did not show any statistically significant interaction effects.
Discussion
Following exposure to cariogenic food and beverage advertisements, children in this study consumed a greater amount of the test items (both in terms of energy and sugar content) relative to after toy advertisements. This is consistent with previous research both in terms of the observed differences in overall intake(Reference Boyland, Nolan and Kelly6,Reference Russell, Croker and Viner15) and the ‘beyond-brand’ nature of the advertising effect(Reference Halford, Boyland and Hughes39), whereby food advertisement exposure does not just influence consumption of the specific product(s) advertised but extends to others in the same category (in this instance, snacks)(Reference Hastings, Stead and McDermott40). The effects were driven by increased intake specifically of the items with the greatest sugar content (chocolate and jelly sweets with 54·4 and 55 g of sugar per 100 g of product, respectively) which is consistent with the conclusion of Hastings et al.(Reference Hastings, Stead and McDermott40), that food marketing operates at a food type or category level.
Although the effects were relatively small (increases of 203·3 kJ (48·6 kcal) and 6 g sugar), they should be considered in the context of children’s overall energy balance and the so-called ‘energy gap’(Reference van den Berg, Boer and Scholtens41). A sustained daily overconsumption (relative to energy requirements) of just 192 kJ/d (46 kcal/d) can be sufficient to lead to the development of overweight in children(Reference Plachta-Danielzik, Landsberg and Bosy-Westphal42). Indeed, the global rises in obesity prevalence are the result of relatively small but repeated, cumulative increases in overall energy intake by individuals(Reference Ford and Dietz43). Small, individual level effects can be hugely impactful when seen across populations(Reference Gortmaker, Swinburn and Levy44). Furthermore, the current study only examined short-term intake responses to acute advertisement exposure. In reality, children are continually exposed to food marketing delivered via numerous platforms (e.g. television, Internet, outdoor, event sponsorship and point-of-sale retail environments(Reference Boyland and Whalen45)) in many settings and repeated over time. This ‘real-world’ experience of food marketing exposure is likely to lead to an amplification of the effects observed in this study.
There were differences in food intake response to the advertising exposure across sub-groups related to dental health. Children with experience of dental caries had a greater intake response relative to those with no experience of dental caries. This finding is consistent with that of Gatou et al.(Reference Gatou, Mamai-Homata and Koletsi-Kounari30). This should not necessarily be taken as evidence that children with dental caries are more likely to respond to food advertising per se, as dental caries may simply be a proxy for prior intake of sugary foods or prior advertising exposure. Longitudinal research is needed to properly tease out the interrelationships between these factors and their causality.
There were also observed differences in food intake response to food advertisement exposure across weight status groups for energy intake (but not sugar). However, this was in the opposite direction to that hypothesised as the children with overweight and obesity consumed less energy after food advertisement exposure than after the toy advertisements, whereas those of a healthy weight consumed more. The extant evidence supports a causal link between food marketing exposure and weight gain in children(Reference Norman, Kelly and Boyland8), and previous research has suggested that this at least partly reflects a greater acute food intake response to the advertising content in children with overweight and obesity(Reference Russell, Croker and Viner15). Our findings do not support this. However, the effects observed here may have been driven by social desirability, in light of perceived links between self-efficacy and having overweight and obesity in childhood, as well as social devaluation and stigmatisation of children with excess weight(Reference Di Pasquale and Celsi46). It may also reflect habitual behaviours of the healthy-weight children, who may be more likely to be physically active and be permitted to consume sugar-containing snack foods at home. Advertising is thought to be influential across a hierarchy of behavioural outcomes(Reference Kelly, King and Chapman47), it is currently unclear whether robust weight status effects occur consistently across any of these outcomes. These gaps in understanding should be addressed by future research.
There were also no observed differences in intake patterns across the five quintiles of SES. There is a marked socio-economic gradient to obesity, whereby in industrialised nations, those of lower SES have a much greater risk of obesity(Reference Wang and Lim48); however, the current study does not support the premise that greater reactivity to advertising contributes to this phenomenon. This is in contrast to previous studies(Reference Kumanyika and Grier13,Reference D’Alessio, Laghi and Baiocco14) but may reflect the lack of variation in SES in this sample (the vast majority of participants fell in the two most deprived quintiles). Advertising could still contribute to the SES gradient to obesity via greater exposure of food marketing in low SES groups(Reference Adams, Tyrrell and Adamson10).
The lack of group differences appears to be at least partly an issue of power. The study was powered for our primary hypothesis (overall intake across advertisement conditions), not for the secondary considerations of dental caries, weight status or SES. It is clear that obesity and dental caries have common risk factors other than overconsumption of sugar, including SES(Reference Hooley, Skouteris and Boganin49), and larger studies with more heterogeneous samples will be required to explore the interrelationships between these factors and marketing further.
Limitations of the study
This paper describes a small experimental study, with a relatively homogeneous sample. The five-point Likert scale for hunger has not been validated. The advertising exposure was of brief duration on each occasion (approximately 2 min), and immediate food and beverage intake was measured from a small selection of items. This within-subjects experimental design accounts for any underlying food preferences but does not measure sustained effects beyond the testing period or the effects of cumulative exposure. The particular selection of foods offered for consumption may also be considered a limitation, as children had a binary choice between sweets and fruit and did not have the option of selecting savoury items (e.g. potato crisps) as an indication of reduced sweet preference. Because of this, we are unable to fully disentangle whether the observed effects reflect changing preference for sugar content across advertising conditions or a category level (confectionery) cued consumption effect in the food advertising condition. In addition, although children were asked to keep other eating behaviour (e.g. breakfast consumption) and physical activity consistent across study days (and the prior 24-h period), the level of compliance with these instructions is unknown. Fluid intake prior to the test sessions was also not controlled for, which may have influenced snack intake. Awareness of the dental examination taking place at the end of the second study session may also have affected eating behaviour (choice of snacks and level of consumption) in some participants.
Conclusion
To the authors’ knowledge, this is the first study to have empirically tested the impact of exposure to high-sugar food and beverage advertising specifically on intake of sweet foods while also exploring the role of dental health, body weight and SES in this effect. Exposure to such advertising did increase sugar and energy intake in this sample of children, and therefore, these data have implications for dental health as well as general dietary-related health and body weight. This study adds to the body of evidence suggesting that the marketing of HFSS foods could negatively impact on sugar and energy intakes in children and therefore supports action to reduce children’s exposure to the advertising of HFSS foods across all broadcast and non-broadcast media.
Acknowledgements
The authors wish to thank Lee Cooper and Gleb Komarov for their assistance with data collection. The authors are grateful to the participating school, pupils and parents and to the peer reviewers for their constructive feedback on a previous version of this manuscript.
The authors have no financial relationships relevant to this article to disclose. Funded by the University of Liverpool Doctorate in Dental Science (DDSc) research fund.
J. K. conceptualised and designed the study, coordinated data collection, collected data, carried out the initial analyses and reviewed and revised the manuscript. R. F. conceptualised and designed the study, drafted the protocol, collected data and reviewed and revised the manuscript. G. B. conceptualised and designed the study, supervised statistical analysis and reviewed and revised the manuscript. S. H. conceptualised and designed the study, collected data and reviewed and revised the manuscript. N. F. and J. C. G. H. conceptualised and designed the study and reviewed and revised the manuscript. E. J. B. conceptualised and designed the study, supervised data collection, collected data, contributed to data analysis and critically reviewed and revised the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
The authors have no conflicts of interest relevant to this article to disclose.



