


INTRODUCTION
Everyday memory function, which encompasses actual or perceived mnemonic ability in daily life, is an emergent area of research. Adult studies suggest that these abilities cannot necessarily be inferred from neuropsychological tasks as there is, at best, a modest relationship between formal and functional measures (see Chaytor & Schmitter-Edgecombe, 2003 for review). Whereas this weak concordance could reflect limitations in the measures of everyday memory or the poor ecological validity of neuropsychological tasks, these data may also indicate that everyday memory is a distinct memory construct with unique predictors. For example, temporal lobe epilepsy (TLE) research suggests that objective test performance is a weak predictor of everyday memory and that these skills are more strongly related to mood and personality (see Perez-Garcia et al., 1998). Non-mnemonic factors are unlikely to be the only source of difficulties in memory ratings, as O'Shea (1996) found seizure variables were strong predictors when ratings were completed by a significant-other. These data suggest that everyday memory is a complex construct that is partially related to objective test performance, but also influenced by non-mnemonic factors.
Everyday memory has largely been overlooked in pediatric research. In terms of methodology, self-report measures are limited by a child's literacy and capacity for introspection. Parent-report scales can be utilized with a wider age group, but these scales must be well validated as extraneous factors can influence a parent's appraisal of their child's abilities. For example, parents may differ in terms of whether they consider the same behavior problematic or some family environments may provide more implicit structure to support memory function than others. Notwithstanding these considerations, Drysdale et al. (2004) explored the psychometric properties of a parent-report scale, an adapted version of the Everyday Memory Questionnaire (EMQ, Sunderland et al., 1983), in healthy controls. They found the EMQ had sound psychometric properties in healthy children and was moderately correlated with some objective memory tasks.
Kadis et al. (2004) and Drysdale et al. (2004) explored everyday memory in a clinical group. Although Kadis and colleagues found their adapted version of the Memory Observation Questionnaire (MOQ, McGlone & Wands, 1991) was predicted by parent ratings of attention, but not mood or objective test performance, in a mixed epilepsy cohort, these data are difficult to interpret in the absence of psychometric data on the MOQ. Drysdale et al. (2004) explored the diagnostic utility of the EMQ in children with attention deficit hyperactivity disorder (ADHD) and/or learning difficulties and found the clinical group performed at comparable levels to controls. This null finding may represent either limitations of the EMQ or the absence of a real effect, given that these groups performed within the average range on objective memory tests.
This study aims to further pediatric everyday memory research by introducing a new parent-report questionnaire, the Observer Memory Questionnaire–Parent Form (OMQ-PF). The properties of the scale were explored in a normative sample (Study 1) and clinical sensitivity was examined in children with TLE (Study 2). It was expected that the OMQ-PF would have sound internal validity in the normative sample and that children with TLE would perform below normative standards. The relationship between the OMQ-PF and traditional neuropsychological measures was explored in both cohorts. Consistent with other studies, it was expected that there would be a modest, yet significant, relationship between neuropsychological and everyday memory tasks.
METHOD
Study 1
Participants
Four hundred children aged between 5–16 years and their parents participated in this study. Subjects were recruited from the community (n = 313) or via schools located in metropolitan Melbourne (n = 87). School-based recruitment involved teachers distributing information about the study, consent forms and parent questionnaires to all eligible children. Once consent forms and parent questionnaires had been returned, children were assessed at their school. This method of recruitment proved to be slow and the sample size insufficient to meet the study aims. The remaining data were collected by undergraduate college students as part of their course requirements under the supervision of one author (VA). All data were scored by another author (LG). Students were instructed to test a child aged between 7–13 years if possible, as additional measures were collected targeting this age group. Collection and use of data, irrespective of method of recruitment, was approved by the Human Ethics Committee of the University of Melbourne and the Department of Education and Training, Victoria, Australia.
Inclusion criteria were enrollment in mainstream schooling and English as a first language. Exclusion criteria were enrollment in special (remedial) education classes and/or a history of neurological and developmental or psychiatric disorder, including ADHD and learning disorders. The selection criteria were verified by a background questionnaire completed by the child's parent/s.
Twenty-four questionnaires were excluded as they contained missing data or the child did not meet the inclusion criteria. Table 1 reports the age and gender distribution of the remaining 376 participants.
Demographic statistics for normative sample

Measures
Parents of participants completed the OMQ-PF and children were administered a selection of objective memory tasks.
The OMQ-PF is a 27-item questionnaire designed to ascertain parents' perceptions of their child's memory function (Appendix 1). The scale was adapted from the Observer Memory Questionnaire (OMQ, O'Shea, 1996), which was developed for the significant-others of adults with epilepsy to rate everyday memory. The OMQ differs from other adult scales as items were drawn directly from the complaints patients and relatives offer in clinical interview. Seventeen items on the OMQ-PF were taken directly from the original scale. The remaining items were generated from clinical experience to reflect the memory difficulties parents report their children encounter in everyday life. These items were drawn from a review of the principal author's case files.
The OMQ-PF primarily comprises items inquiring about memory function in everyday scenarios (e.g., does your child frequently lose important information such as notes to and from school?) and beliefs about memory function (e.g., compared with other children of the same age, his/her memory ability is poor). A small number of items pertaining to non-mnemonic functions were also included (e.g., “your child is easily disrupted by changes to his/her routine”), as parents often include these difficulties as part of their child's memory complaint. Seventeen items were posed in the form of a question. The remaining items were presented as statements. Each item was scored on a 5-point Likert scale. In order to reduce the likelihood of a response bias, questions were mixed in terms of whether a high or low rating was optimal. Items where a low score was optimal were re-coded (see Appendix 1). After re-coding, a high score reflected better everyday memory function. Items were summed to yield a total score ranging from 27–135.
Because the scale was not designed to capture developmental increments in everyday memory, parents were instructed to rate items negatively only when difficulties were beyond what would be expected for other children of the same age.
Verbal paired associates (VPA), Wechsler Memory Scale–Revised (WMS-R, Wechsler, 1987) The dependent variables were total words recalled across three learning trials and total words recalled after a 30-minute delay. This measure of verbal memory was administered to provide normative data for a parallel study which required the separation of arbitrary and semantic associative learning (Gonzalez et al., 2007).
Rey Complex Figure Test (RCFT, as described in Spreen & Strauss, 1998). Incidental recall was assessed three minutes after the initial copy. The dependent variable was the proportion of the initial copy recalled on delay.
Digit span (Anderson & Lajoie, 1996). Forwards digit span was administered as a measure of short-term memory. The dependent variable was the maximum number of digits correctly recalled. This measure was only available for 279 participants.
Statistical analysis
The 27 items of the OMQ-PF were screened to identify redundant items, defined as those with poor item-total correlation (r < .30) or high item-item correlation (r > .80). A series of Cronbach's alpha analyses was then run on the remaining items. One of the items on the scale was excluded from each analysis to determine if its removal resulted in an improvement in internal consistency.
Two-way ANOVA was employed to examine age and gender effects for the scale. For the purpose of this analysis, the 5- and 6-year-olds were combined as were 14–16 year olds to ensure more equal sample sizes across age groups. Pearson correlations were performed to examine the relationship between neuropsychological measures and the OMQ-PF.
RESULTS
The average correlation between each item and the total OMQ-PF score was .56, range .36–.79. The average correlation between each item was .30, range .04–.76. Cronbach's alpha was .92 for the 27-item scale. This level of internal consistency was not improved by removing any of the items from the analysis (Cronbach's alpha range .91–.92). These data support retention of all items.
The mean score for the OMQ-PF was 107.26, SD = 13.00, range 57–135. Two-way ANOVA revealed no main effects for age, F(8,358) = 0.93, p = .50, or gender, F(1,358) = 2.62, p = .11, nor any interaction between these variables, F(8,358) = 1.64, p = .11. The correlation between VPA pairs learnt and the OMQ-PF was significant, r = .12, p = .02. Correlations were non-significant between the OMQ-PF and VPA pairs recalled on delay, r = .08, p = .12, RCFT proportion retained, r = .06, p = .30, and Digit Span, r = .03, p = .59.
METHOD
Study 2
Participants
Forty-four children aged 6–16 years (M = 12.23, SD = 2.69) with lesional TLE participated in this study. Participants were recruited prospectively from the Royal Children's Hospital (n = 38) and the Austin Hospital, Melbourne, Australia (n = 6). This study was approved by the Ethics Committees at both institutions. This sample has been described in detail in Gonzalez et al. (2007) and included seizure free and refractory cases. No participant had undergone temporal lobe surgery.
Measures
The OMQ-PF was completed by a parent of each participant. In addition to VPA and RCFT (as described in Study 1), the following measures were administered:
Faces subtest, Children's Memory Scale (Cohen, 1992). The immediate and delayed conditions were administered and scaled scores utilized as dependent variables.
Digit Span subtest, Wechsler Intelligence Scale for Children, third edition (WISC-III, Wechsler, 1991). This measure was preferred over that used in Study 1, as it allowed for separation of digits forwards (DF) and digits backwards (DB), which are accepted measures of short term and working memory respectively. Scaled scores were generated for DF and DB utilizing the WISC-III-PI (Kaplan et al., 1999).
Intelligence was estimated from the Block Design and Vocabulary subtests of the WISC-III (Wechsler, 1991), which Sattler (1992) suggests is a particularly reliable short-form.
Statistical analysis
Raw scores were utilized for the OMQ-PF given the absence of age effects in Study 1. Scaled scores were reported for Faces, IQ, DF and DB. Z-scores were generated for VPA and RCFT on the basis of the normative data collected in Study 1. The relationship between the OMQ-PF and neuropsychological variables was explored through Pearson correlation.
RESULTS
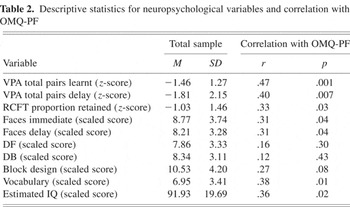
The total TLE sample, M = 93.48, SD = 23.04, scored more than one standard deviation below the mean of the healthy cohort on the OMQ-PF, which is a significant decrement, t (43) = −3.97, p < .001. As detailed in Table 2, the OMQ-PF was significantly correlated with immediate and delayed recall of VPA and Faces, proportion recalled on RCFT, Vocabulary and the overall IQ estimate.
Descriptive statistics for neuropsychological variables and correlation with OMQ-PF
DISCUSSION
This study introduces a new measure of everyday memory suitable for the use with children. The OMQ-PF has sound internal consistency in healthy children and no age effects were detected, suggesting that the scale is not tapping developmental increments in everyday memory. The OMQ-PF was sensitive to impairment in a TLE cohort. These findings are encouraging in terms of the properties of the OMQ-PF and suggest that further development is warranted.
The study examined the correlation between the OMQ-PF and neuropsychological tasks in both samples, providing some preliminary insight into the construct validity of the scale. In the normative group there was a small but significant correlation between the OMQ-PF and VPA learning trials. Although the finding of a modest effect is consistent with the studies reviewed by Chaytor and Schmitter-Edgecombe (2003) and Perez-Garcia et al. (1998), the absence of correlations between the OMQ-PF and other memory tasks was unexpected. This pattern of results may indicate that the OMQ-PF is more closely related to new learning ability rather than the retention or recall of information. Given the effect was small, replication is recommended. The OMQ-PF was not correlated with measures of short term memory, which may indicate that the OMQ-PF is not tapping the initial stages of information processing. However, this finding does not exclude the possibility that everyday memory function may be influenced by more specific attentional processes that were not assessed in the current study.
Unexpectedly, there were more numerous and stronger correlations between the OMQ-PF and neuropsychological measures in the TLE group relative to controls. The basis for this different pattern of results in the TLE and normative samples is not clear. One possibility is that parent's of children with TLE may be more aware of their child's memory function, as they may have been alerted to the vulnerability of these skills by their treating professionals. Alternatively, significant correlations may be more easily elucidated in the TLE group on account of greater variability in function within this cohort. Drawing items directly from the complaints offered by TLE patients may have contributed to differences in results between the samples. Finally, it may be that there are differences between the characteristics of the parents in both samples, possibly in terms of stress, mood or socio-economic status, which explains this disparity.
Although the OMQ-PF is still in an early stage of development, it is a useful addition to the limited number of everyday memory questionnaires available for children. Further work is however required to better understand the characteristics of this scale. It is suggested that formal stratified standardization be undertaken including a thorough description of the characteristics of the parents and administration of a wider range of neuropsychological tasks to healthy children, including intelligence. It would also be useful to examine the factor structure of the OMQ-PF to identify whether there are more specific components to everyday memory.
Better understanding of the properties of the OMQ-PF facilitates the use of this measure in clinical research. There is considerable scope to explore the predictors of everyday memory function in TLE and other clinical groups, as adult studies suggest that such research is highly informative in identifying risk factors for day-to-day memory difficulties. Well-designed clinical studies should include careful consideration of non-mnemonic factors that could influence everyday memory, such as parent and child mood, severity, and duration of illness and parent perceptions of other cognitive skills.
ACKNOWLEDGMENTS
This research was supported by grants from the Perpetual Foundation and the Murdoch Children's Research Institute. The authors have no conflicts of interest, financial or otherwise, to declare. The authors thank Dr Marie O'Shea for granting permission to modify the OMQ and giving access to her PhD study. Finally they thank the children and their parents who participated in this study.
APPENDIX 1
Observer Memory Questionnaire—Parent Form
This questionnaire is designed as a measure of how your child remembers day to day information. We are trying to identify problems, beyond what is normal for your child's age group, therefore, it may be useful to keep in mind the abilities of other children of the same age.
- Does your child frequently lose important information (e.g., notes to and from school)?
- Does your child become anxious when he/she forgets things that other people appear to remember easily?
- Does your child recall details of previous conversations?
- Do you have to provide reminders for him/her?
- When your child is speaking, does he/she lose track of what they are trying to say?
- Does your child forget where he/she has put things in the house?
- Compared with other children of the same age, his/her memory ability is poor.
- Is he/she reliable at giving messages (eg. telephone messages) to others?
- Does your child repeat him/herself unintentionally in conversation (e.g. asking the same question)?
- If your child did not place things in the same location he/she would have difficulty finding them again (eg. school bag)?
- Do others (including teachers) comment that your child appears to have a poor memory?
- Your child's memory has progressed at the same rate as his/her peers.
- Does your child have to write themselves reminder notes if they are to remember to do things (eg. take a book to school)?
- Of all your child's abilities, memory is his/her weakest skill.
- Does your child set off to do something then forget what it is he/she wanted to do (eg, going into another room to fetch something, then wondering what it was)?
- Your child has a limited concentration span.
- Does your child get flustered when someone gives him/her a list of things to do (eg, errands to perform)?
- He/she has a poor memory.
- He/she forgets details of significant family events, such as birthdays and Christmas.
- He/she brings the correct books home for homework tasks.
- If your child does not do things as soon as he/she thinks of them he/she will forget them altogether.
- Does he/she learn new things quickly and easily (eg. rules of a game)?
- Does your child complain that his/her memory is poor?
- Does your child require information to be repeated several times before they grasp what they are being asked to do?
- Does forgetting interfere with his/her day-to-day activities?
- Your child's memory is limiting his/her achievements at school.
- Your child is easily disrupted by changes to his/her routine.
All items are rated on a 5 point Likert scale. For items 7, 12, 14, 16, 18, 19, 29, 21, 26, 27 that scale constitutes 1. agree strongly, 2. agree, 3. undecided, 4. disagree, 5. strongly disagree. For all remaining items the scale is: 1.never, 2. rarely, 3. sometimes, 4. often, 5. always.
Recode items 1, 2, 4, 5, 6, 9, 11, 12, 13, 16, 17, 20, 23, 24, 25 so that a high score is optimal


