CVD represent the main causes of death globally, accounting for nearly one-third of all deaths worldwide( Reference Wong 1 ). Moreover, as life expectancy has improved in both developed and developing countries, the number of healthy years lost due to disability has been increasing consistently( Reference Salomon, Wang and Freeman 2 ). Within this scenario, primary prevention of CVD-related morbidity and mortality represents a major priority for public health strategies to reduce the burden of such conditions( Reference Forman and Bulwer 3 ). Lifestyle factors have been considered main targets to prevent CVD, because they are modifiable behaviours that could highly affect both the risk and the prognosis of the disease. A number of healthy dietary patterns have demonstrated beneficial effects in decreasing the burden of CVD-related risk factors and CVD incidence and mortality( Reference Grosso, Mistretta and Frigiola 4 , Reference Sofi, Macchi and Abbate 5 ). Scientific literature suggests that a diet rich in antioxidants (such as vitamins and polyphenols), fibre, n-3 fatty acids, MUFA and PUFA may decrease the risk of the aforementioned conditions( Reference Grosso, Mistretta and Marventano 6 , Reference Hirotani, Ozaki and Tsuji 7 ). Among the potential mechanisms of protection, the antioxidant and anti-inflammatory action of these compounds may mediate their effects( Reference Bahadoran, Mirmiran and Tohidi 8 , Reference Stedile, Canuto and de Col 9 ). From a nutritional point of view, legumes are a source of some of these nutrients and bioactive compounds as well as an excellent source of fibre and vegetable proteins( Reference Bouchenak and Lamri-Senhadji 10 , Reference Guine, Ferreira and Correia 11 ). Despite not being associated with decreased risk of CVD themselves, vegetable proteins may be a valuable alternative to animal proteins, which on the contrary are associated with saturated fats and possible adverse outcomes( Reference Berciano and Ordovas 12 ).
Meta-analyses of studies on legume consumption and cardiovascular health demonstrated no association with stroke or diabetes( Reference Afshin, Micha and Khatibzadeh 13 , Reference Shi, Tang and Wu 14 ). Legumes considered as part of a Mediterranean dietary pattern have been associated with a decreased risk of CVD risk and mortality in studies evaluating Mediterranean diet as main exposure( Reference Grosso, Marventano and Yang 15 ), but a comprehensive evaluation of their independent role on such outcomes is lacking. The aim of the present study was to systematically review and perform a meta-analysis of prospective cohort studies exploring the association between dietary legume consumption and CVD risk, including CHD and stroke.
Participants and methods
Search strategy
We performed a systematic search in PubMed (http://www.ncbi.nlm.nih.gov/pubmed/) and EMBASE (http://www.embase.com/) databases of all English-language studies published up to December 2015. The search terms used for the study selection were ‘legume’, ‘Mediterranean diet’, ‘soy products’, ‘protein sources’ combined with ‘cardiovascular disease’, ‘coronary heart disease’ and ‘mortality’. Inclusion criteria were: (i) having a prospective cohort design; (ii) evaluating the association between dietary consumption of legumes and CVD; and (iii) assessing and reporting hazard ratios (HR) and the corresponding 95 % CI for the outcome considered. Reference lists of included studies were examined for any additional article not previously identified. If more than one study was conducted on the same cohort, only the most comprehensive or most updated was included in the meta-analysis. The selection process was performed independently by two authors (G.G. and J.G.).
Data extraction and study quality assessment
Data were abstracted from each identified study by using a standardized extraction form. The following information was collected: (i) author name; (ii) year of publication; (iii) country; (iv) number, sex and age of participants; (v) HR and 95 % CI for all categories of exposure; and (vi) covariates used in adjustments.
The quality of each study was assessed by applying the Newcastle–Ottawa Quality Assessment Scale( Reference Wells, Shea and O’Connell 16 ). The instrument consists of three domains indicating the study quality as follows: selection (4 points), comparability (2 points) and outcome (3 points), for a total score of 9 points (with 9 points representing the highest quality). Studies scoring 7–9 points, 3–6 points and 0–3 points were identified as of high, moderate and low quality, respectively.
Statistical analysis
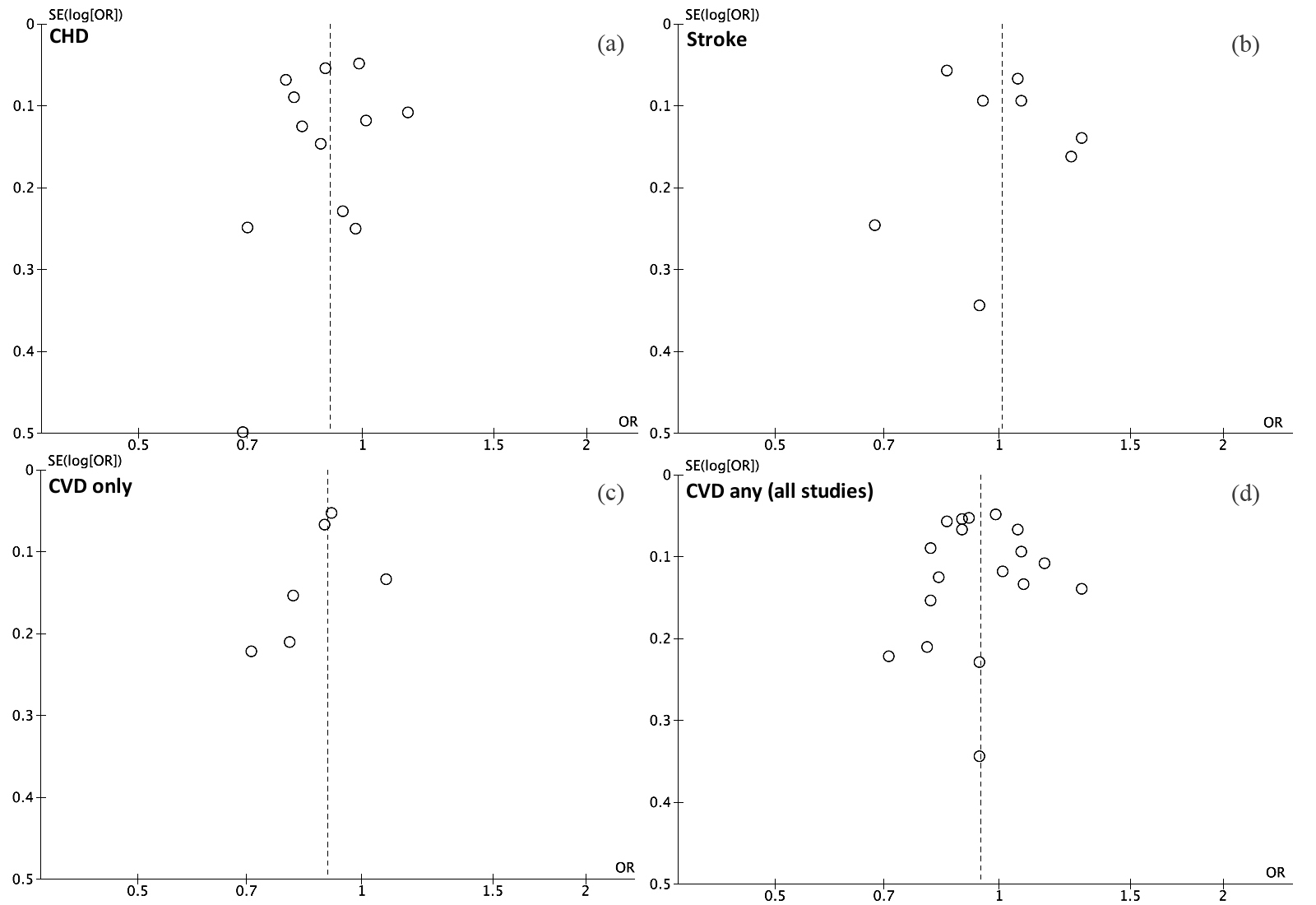
HR with 95 % CI for all categories of exposure were extracted for the analysis and random-effects models were used to calculate pooled relative risks (RR) with 95 % CI for the highest v. lowest (reference) category of exposure. The risk estimate from the most fully adjusted models in the analysis of the pooled RR was used. When analyses were presented by sex, stratified results were taken into account for the pooled analysis. Since most of the studies considered a composite outcome of CVD incidence or mortality, when studies presented separate analyses for the two outcomes, a pooled RR was estimated within the same study and only secondarily it was included in the general analysis in order to compare more homogeneous outcomes. Heterogeneity was assessed by using the Q test and I 2 statistic. The level of significance for the Q test was defined as P<0·10. The I 2 statistic represented the amount of total variation that could be attributed to heterogeneity. I 2 values of ≤25 %, ≤50 %, ≤75 % and >75 % indicated no, small, moderate and significant heterogeneity, respectively. A sensitivity analysis by exclusion of one study at a time was performed to assess the stability of results and potential sources of heterogeneity. Subgroup analyses were also performed to check for potential source of heterogeneity according to geographical area, sample size, year of publication, study quality, type of exposure ascertainment method and length of follow-up. Publication bias was evaluated by a visual investigation of funnel plots for potential asymmetry. All analyses were performed with Review Manager (RevMan) software version 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration).
Results
Study characteristics
The process of study selection following PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines is summarized in Fig. 1. Among the thirty-four articles obtained after screening on the basis of title and abstract, twenty studies were excluded after a full-text examination because they were not relevant for the research (n 11), did not study CVD as outcome (n 3), had a study design other than prospective (n 2), reported insufficient statistics (n 2), were conducted on the same cohort of another study but had shorter follow-up (n 1) or considered composite legume and other foods consumption (n 1). This inclusion strategy resulted in the final inclusion of fourteen studies( Reference Bazzano, He and Ogden 17 – Reference Nouri, Sarrafzadegan and Mohammadifard 30 ) and thirty-two data sets eligible to be considered for the quantitative analysis. Studies included were conducted on eleven cohorts and accounted for a total of 367 000 individuals and 18 475 cases of CVD, including 7451 CHD and 6336 stroke cases.

Fig. 1 Flowchart indicating the selection of relevant studies for the systematic review exploring the association between dietary legume consumption and CVD risk
Table 1 shows the main characteristics extracted from all selected studies. The studies were conducted on cohorts based in the USA( Reference Bazzano, He and Ogden 17 , Reference Kelemen, Kushi and Jacobs 18 , Reference Bernstein, Sun and Hu 23 , Reference Bernstein, Pan and Rexrode 26 , Reference Haring, Gronroos and Nettleton 28 , Reference Haring, Misialek and Rebholz 29 ), Japan( Reference Kokubo, Iso and Ishihara 19 , Reference Nagura, Iso and Watanabe 22 ), Spain( Reference Buckland, Gonzalez and Agudo 20 , Reference Martinez-Gonzalez, Garcia-Lopez and Bes-Rastrollo 24 ), Greece( Reference Dilis, Katsoulis and Lagiou 25 , Reference Misirli, Benetou and Lagiou 27 ), Finland( Reference Mizrahi, Knekt and Montonen 21 ) and Iran( Reference Nouri, Sarrafzadegan and Mohammadifard 30 ). The results of quality assessment yielded a score of 8 or above for all studies with no substantial limitations or significant weaknesses across studies. Most of the studies included more than 10 000 individuals and follow-up periods were long enough to plausibly observe occurrence of the outcomes considered in the present review. The amount of dietary legumes considered as the highest category of exposure varied across studies in terms of measurements, but in summary could be roughly estimated as <1 serving/d or 3–4 servings/week.
Table 1 Background characteristics of the studies included in the present meta-analysis exploring the association between dietary legume consumption and CVD risk

NHANES I, First National Health and Nutrition Examination Survey; IWHS, Iowa Women’s Health Study; JPHC, Japan Public Health Center-based; EPIC, European Prospective Investigation into Cancer and Nutrition; JACCS, Japan Collaborative Cohort Study; NHS, Nurses’ Health Study; SUN, Seguimiento Universidad de Navarra; HPFS, Health Professionals’ Follow-up Study; ARIC, Atherosclerosis Risk in Communities; M, male; F, female; MI, myocardial infarction; CBVD, cerebrovascular disease; PA, physical activity; TC, total cholesterol; SBP, systolic blood pressure; HDL-C, HDL cholesterol; WHR, waist-to-hip ratio.
Legume consumption and CVD risk
All fourteen studies including CVD, CHD and/or stroke incidence or mortality were considered for the analysis of the extreme categories of legume consumption and total CVD. RR with 95 % CI of CVD for the highest v. the lowest legume consumption category were calculated for eighteen data sets and resulted in a 6 % decreased risk of CVD (RR=0·94; 95 % CI 0·89, 1·00; Fig. 2) with little heterogeneity (I 2=40 %). Sensitivity analysis led to evidence that heterogeneity was mainly due to one cohort( Reference Haring, Gronroos and Nettleton 28 , Reference Haring, Misialek and Rebholz 29 ) after exclusion of which heterogeneity was significantly reduced and risk estimates remained significant. No publication bias was found for this analysis (see online supplementary material, Supplementary Fig. 1(d)). Subgroup analyses were conducted to test the stability of results or potential confounding factors (Table 2). Overall, higher legume consumption had a protective effect against CVD in most subgroups. However, the association was not significant when analyses included men only, when studies were conducted in non-Mediterranean countries and after controlling for dietary variables (Table 2).

Fig. 2 Forest plot of summary relative risk (RR) of CVD for the highest v. lowest (reference) category of legume consumption. The analysis was stratified by pooling studies exploring as outcome the risk of CHD, stroke, CVD only and any CVD (all studies). The study-specific RR and 95 % CI are represented by the black square and horizontal line, respectively; the area of the black square is proportional to the specific-study weight to the overall meta-analysis. The centre of the diamond represents the pooled RR and its width represents the pooled 95 % CI
Table 2 Subgroup analyses of studies reporting risk of CVD for the highest v. lowest (reference) category of legume intake

RR, relative risk.
A second analysis was conducted including only studies that specifically considered CVD as the outcome( Reference Bazzano, He and Ogden 17 , Reference Kokubo, Iso and Ishihara 19 , Reference Nagura, Iso and Watanabe 22 , Reference Martinez-Gonzalez, Garcia-Lopez and Bes-Rastrollo 24 , Reference Nouri, Sarrafzadegan and Mohammadifard 30 ). Overall, a decreased risk of 10 % (RR=0·90; 95 % CI 0·84, 0·97; Fig. 2) was observed, with no evidence of either heterogeneity or publication bias (see online supplementary material, Supplementary Fig. 1(c)). Stratified analyses were conditioned by the limited number of data sets (Table 2). However, no substantial differences from the primary analysis were found in studies with a larger sample, longer follow-up and adjusted for nutritional factors.
Legume consumption and CHD risk
The analysis relative to CHD risk related to consumption of legumes comprised twelve data sets derived from eight studies( Reference Bazzano, He and Ogden 17 – Reference Buckland, Gonzalez and Agudo 20 , Reference Bernstein, Sun and Hu 23 , Reference Martinez-Gonzalez, Garcia-Lopez and Bes-Rastrollo 24 , Reference Dilis, Katsoulis and Lagiou 25 , Reference Haring, Gronroos and Nettleton 28 ). Comparison of the highest v. the lowest legume consumption category showed a similar risk estimate to the previous analysis considering CVD as outcome (RR=0·90; 95 % CI 0·84, 0·97; Fig. 2). Little heterogeneity (I 2=34 %) and no publication bias were found (see online supplementary material, Supplementary Fig. 1(a)). Exclusion of one study at the time did not change the strength of the association. Subgroup analyses demonstrated stability of results across strata considered, showing a significant decreased risk of CHD by high consumption of legumes in all subgroups with the exception of pooled analysis of studies conducted in the Mediterranean region.
Legume consumption and stroke risk
Six studies( Reference Kokubo, Iso and Ishihara 19 , Reference Mizrahi, Knekt and Montonen 21 , Reference Nagura, Iso and Watanabe 22 , Reference Bernstein, Pan and Rexrode 26 , Reference Misirli, Benetou and Lagiou 27 , Reference Haring, Misialek and Rebholz 29 ) comprising eight data sets were considered for the analysis on the highest v. lowest level of dietary legume intake and stroke risk. The pooled analysis showed null results with no substantial risk increment or reduction for higher consumption of legumes (RR=1·01; 95 % CI 0·89, 1·14). The analysis showed moderate heterogeneity (I 2=59 %) due to divergent results reported in two studies( Reference Kokubo, Iso and Ishihara 19 , Reference Haring, Misialek and Rebholz 29 ). The stratified analysis (Table 2) revealed that heterogeneity was attenuated by pooling studies conducted in non-Mediterranean countries, showing consistently null results, while the study conducted in Greece( Reference Misirli, Benetou and Lagiou 27 ) reported significant decreased risk of stroke for higher intake of legumes. Interestingly, also pooling together studies reporting adjustment for dietary variables led to decreased heterogeneity and no significant risk variation. No evidence of publication bias was found (see online supplementary material, Supplementary Fig. 1(b)).
Discussion
In the present meta-analysis we found an association between legume consumption and decreased risk of CVD incidence or mortality, despite with little heterogeneity across studies. When the analysis was stratified by type of CVD outcome, legume consumption was associated with CHD only and not with stroke risk. The analysis considering the different outcomes showed that the heterogeneity was due to the null results relative to stroke risk. Previous meta-analyses showed similar results on stroke( Reference Afshin, Micha and Khatibzadeh 13 , Reference Shi, Tang and Wu 14 ), but to date the current meta-analysis is the first showing a relationship between legume consumption and CHD and overall CVD outcomes.
Research on legumes and CVD-related outcomes has been growing over the last years. The majority of prospective studies included in our meta-analysis reported a significant association between legume consumption and risk of CHD. Legumes have been studied lately due to a number of potential effects that may provide health benefits towards CVD risk factors, such as lowering of blood lipids and improvement in vascular function and insulin sensitivity( Reference Singhal, Kaushik and Mathur 31 , Reference Souza, Gomes and Naves 32 ). Legumes are rich in phytosterols, including soya isoflavones, which have been demonstrated to be associated with a significant reduction in serum total cholesterol, TAG and LDL cholesterol, and a significant increase in HDL cholesterol, in pooled analyses of randomized controlled trials on soya products consumption in the general population( Reference Anderson and Bush 33 ) and patients with type 2 diabetes mellitus( Reference Yang, Chen and Xu 34 ). Intakes of these compounds may also protect against atherosclerosis( Reference Schonfeld 35 ). Legumes, as plant-derived foods, are rich in fibre, which has been associated with decreased risk of mortality in prospective cohort studies( Reference Yang, Zhao and Wu 36 ). Dietary fibre is supposed to ameliorate body metabolism and reduce chronic inflammation by affecting body weight, serum lipid levels, blood pressure and insulin resistance, as well as to influence fibrinolysis and coagulation that may be important in the setting of established atherosclerotic plaques( Reference Satija and Hu 37 ). Some legume families, such as soya, are also dietary sources of flavonoids, vitamin E and PUFA (α-linolenic acid) which have demonstrated CVD protection in pooled analyses of prospective studies, hypothesized to be exerted probably by their antioxidant effects( Reference Marventano, Kolacz and Castellano 38 ).
Besides the aforementioned potential direct effects of legumes on cardiovascular health, another potential mechanism of protection may depend on the fact that increased consumption of legumes lowers CVD risk simply by reducing the intake of animal sources of protein that may be high in SFA( Reference Rebello, Greenway and Finley 39 ). Moreover, legume proteins are not only a source of constructive compounds (such as amino acids) but they may also exert bioactive effects on various physiological functions( Reference Malaguti, Dinelli and Leoncini 40 ). Indeed, legume protein-derived bioactive peptides have been demonstrated to exert blood pressure-lowering effects, cholesterol-lowering ability, antithrombotic and antioxidant activities in the laboratory setting, suggesting potential benefits that need to be further investigated in the future( Reference Malaguti, Dinelli and Leoncini 40 ).
The meta-analyses of the studies providing stratified analysis by some selected variables showed that a potential difference between men and women, as well as studies conducted in Mediterranean and non-Mediterranean countries, may occur when examining the relationship between legume consumption and either CVD or CHD risk. A possible explanation for such difference between men and women may rely on the fact that men were generally more likely to be smokers and drink more alcohol( Reference Kelemen, Kushi and Jacobs 18 , Reference Buckland, Gonzalez and Agudo 20 , Reference Dilis, Katsoulis and Lagiou 25 ), thus somehow counteracting the potential beneficial effects of legumes. Another methodological issue may depend on lower accuracy in reporting dietary patterns among men than women. It is noteworthy that only a limited number of studies were included in our sub-analysis by sex, thus limiting the strength of such findings. However, current results were quite consistent and this hypothesis needs further attention in future studies. Regarding the geographical origin of the cohorts included in the pooled analysis, risk of CHD was significantly reduced in high legume consumers in studies conducted in non-Mediterranean countries while CVD risk was reduced in Mediterranean countries. The conflicting results may depend on a bias associated with the relative limited number of studies available for the grouping. One possible explanation for the lack of significant results in meta-analyses of studies conducted in Mediterranean countries could be the impact on cardiovascular health of all components of the diet typically consumed in these countries, or at least those included in the individual analyses. Indeed, most of these studies did not explore the effects of dietary legumes alone as the primary variable of interest towards CVD outcomes, but rather included analyses on Mediterranean diet and, secondarily, on legumes as a component of the diet. It is well known that the Mediterranean diet exerts beneficial effects against CVD( Reference Estruch, Ros and Salas-Salvado 41 ) and thus the effects of legumes, when considered as part of this diet, may be attenuated by the overwhelming effect of all the other components of this dietary pattern. Moreover, consumption of legumes in non-Mediterranean countries is generally associated with a significant lower consumption of red meat, which itself may enhance the lower risk of CHD( Reference Bernstein, Sun and Hu 23 ).
The current review has several strengths. First, all studies included in the pooled analysis were of high quality. Indeed, most of them had a large sample and a long duration of follow-up. Furthermore, all studies provided adjusted analyses for known risk factors, such as smoking, alcohol use and physical activity. Finally, results were not affected by significant heterogeneity and publication bias. Moreover, we included a number of subgroup analyses to test for potential confounders as well as a number of sensitivity analyses to test stability of results. Besides these strengths, the findings have to be considered in light of some limitations. First, the nature of studies included in the meta-analysis was observational, thus no causal relationship can be assessed. Second, despite most studies adjusting multivariate analyses by known confounding factors (smoking, alcohol drinking and physical activity), residual confounders related to dietary and lifestyle factors may still exist. Third, methods of assessment of legume consumption (such as FFQ) may be affected by recall bias. Finally, the number of data sets was sufficient to perform a meta-analysis, but the amount of studies for stratified analyses by sex was relatively low to draft definite assumptions. Moreover, due to the limited information provided in the studies regarding the amount of legumes consumed in each group of exposure, we were unable to perform a dose–response meta-analysis.
Conclusion
In conclusion, results from the current meta-analysis showed that high legume consumption is associated with lower risk of CVD. As legumes have often been reported as part of an overall healthy diet as well as a substitute for unhealthy sources of proteins, a number of bioactive natural compounds may provide the biological plausibility for such potential beneficial effects. Thus, further efforts should be made to explore the specific role of legumes in the diet.
Acknowledgements
Financial support: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflict of interest: The authors have no conflicts of interest to disclose. Authorship: G.G. designed and performed the analysis and wrote the paper; C.S.-G. and M.I.P. performed the data set preparation; J.G. performed the study search and data set preparation; S.M. performed the analyses; M.I.P., F.G. and A.S. provided critical revision to the study. Ethics of human subject participation: Not applicable.
Supplementary material
To view supplementary material for this article, please visit http://dx.doi.org/10.1017/S1368980016002299