



Undernutrition among children widely exists in low- and middle-income countries, most of which are in Asia and Africa. Globally 21·3 % or 144 million children were reported stunted, and 24·7 % in Southeast Asia(1). In Myanmar, formerly known as Burma, there is a challenge to understanding the magnitude of the undernutrition problem due to the lack of nationwide nutrition surveys. The first Demographic Health Survey in Myanmar was conducted in 2015–2016(2), and the findings confirmed the existence of undernutrition among under-five children, with 29·2 % stunted and 57·8 % anaemic. These findings indicated stunting and anaemia as severe public health problems in Myanmar and needed attention(3). Stunting reflects chronic undernutrition due to inadequate dietary intake and repeated bouts of infections. There is a link between the immediate and long-term consequences of child stunting and the underlying adverse environment, which also increases the risk of inadequate child growth and development(Reference Dewey and Begum4). A stunted child is less likely to achieve optimal brain development and higher education(Reference Grantham-McGregor, Cheung and Cueto5). It was also possible that those children would miss their educational potential, consequently impacting the nation’s economy since each year of schooling was associated with increased wages by 7–11 %(Reference Duflo6).
Many factors contribute to child stunting, but household food security plays a fundamental role in child nutrition. Household food insecurity access score intends to measure the food security level in households, and it is frequently used for nutrition surveys(Reference Coates, Swindale and Bilinsky7). Household food insecurity is a sensitive indicator reflecting socio-economic changes and, at the same time, influences the nutritional status of vulnerable groups in the household through its impact on dietary quality or access to nutrient-dense food(Reference Jun, Cowan and Dodd8). Studies have shown that food insecurity is associated with the poor nutritional status of children. Children from moderately food-insecure households were 2·47 times more likely to be severely stunted (AOR = 2·47; 95 % CI (1·77, 3·46)), and those from severely food-insecure households were more likely to be severely stunted (AOR = 1·82; 95 % CI (1·34, 2·48)), compared with children aged 6–59 months from food-secure households(Reference Agho, Mukabutera and Mukazi9). A recently reported meta-analysis of twenty-one studies among 55 173 children and adolescents showed that food insecurity increased the risk of stunting OR: 1·17 (95 % CI: 1·09, 1·25), and the degree of food insecurity intensified the risk of stunting(Reference Moradi, Mirzababaei and Mohammadi10). These studies underline the importance of food insecurity for child stunting but highlight that the link between food insecurity and undernutrition is complex. It is essential to have longitudinal data to understand these associations better. Dietary adequacy is an important factor for healthy child development and even in food-secure household, dietary adequacy for children is not guaranteed. Ensuring dietary adequacy requires good feeding practices, which can be assessed using UNICEF/WHO indicators for feeding practices and whenever possible, effort should be given to assess the feeding practice of children(11). Myanmar has rich natural resources, agriculture is its main economic sector and it was once the main rice exporter in the region. Due to political instability, the country was left behind in all sectors, including health and nutrition. When the country initiated its democratic transition in 2010, there was a high expectation of improvements in the socio-economic status of the population and, eventually, the health and nutritional status of the people. However, it is unclear whether those residing in rural areas benefited from those socio-economic changes. We took this opportunity to investigate the impact of rapid economic transition on the food security and nutritional status of a vulnerable population in rural areas of the country in the early stage of a democratic transition. In this paper, we report the findings from two rounds of cross-sectional surveys (2016–2017) conducted in the same households in three geographical regions of the country.
The study’s objective was to investigate multiple underlying social, economic and agricultural determinants of stunting among under-five children in three distinct ecological areas in rural Myanmar.
Methods
Study design and setting
The study was a repeated cross-sectional panel survey conducted in early 2016 and late 2017 in rural Myanmar, covering pre- and post-harvest seasons. Field teams visited the same households in each round of the survey. We conducted the study in rural villages in three agro-economic zones of Myanmar: Chin state, a mountainous and food insecure area; Magway state, a central plain area with dry zone agricultural land and Ayeyarwady region, a river delta agricultural area (Fig. 1)(Reference Beck, Zimmermann and McVicar12).

Fig. 1 Locations of study townships
Sampling methods and sample size
We purposively selected two adjacent townships in each zone, and from each township, we randomly selected twenty villages by probability proportionate to population size sampling. We randomly selected thirty households in each village to achieve 1200 households per area. A list of households from villages was obtained from township health offices, complemented by information from village midwives or primary health care workers. We listed the households with or without under-five children from each village before randomly selecting fifteen from each category. This process ensured we recruited a minimum number of under-five children from each village.
Data collection
We developed a CommCare application to capture data using structured, error-detecting forms on Android tablets(Reference Style, James Beard and Harris-Fry13). We recruited the survey teams from a local university (University of Community Medicine, Magway) and trained them to interview respondents using electronic data capture and measure anthropometry. Each survey collected data on background characteristics of households such as household socio-economic status, source of drinking water, types of toilets, women’s dietary diversity, household food insecurity, agricultural land access, home gardens, agricultural assets, types of crops, household assets and women’s decision making. In addition, we measured anthropometry for under-five children and women of reproductive age in the recruited households. The women in the household were most knowledgeable about the activities of household members and the food consumption pattern of families and were the survey respondents.
Measures
Women’s decision-making: We classified women’s decision-making into three groups based on their responses to the six decision-making questions on (i) respondent’s health care, (ii) daily household purchase, (iii) large household purchase, (iv) visit to relatives, (v) types of food cook and (vi) using money. For each question, a score of three was given if the decision was made by ‘Respondent alone’, a score of one was given if the decision was made by ‘Respondent and husband/another male’ and a score of zero was given if the decision was made by ‘husband/another male alone’. Then, we calculated the weighted average score and categorised the scores ‘3’ as makes the decision by mother alone, ‘2’ as ‘makes the decision for at least three of the decisions alone and at least three of the decisions with her husband’, score ‘1’ as ‘at least six decisions together with her husband or a combination of fewer than six decisions with husband and less than four decisions alone’, and score ‘0’ as ‘no decision making’.(Reference Ghose, Feng and Tang14).
Household Food Insecurity: We assessed household food insecurity using the household food-insecurity access score to detect household food insecurity prevalence between the two surveys(Reference Coates, Swindale and Bilinsky7). The module consists of nine sets of questions, each related to the occurrence and frequency of experiencing food insecurity in households. Based on the scores, the households were categorised into food secure, mildly food insecure, moderately food insecure or severely food insecure.
Women Dietary Diversity: We interviewed women from households about their consumption of different food groups in the last 24 h. The ten food groups in the survey followed FAO recommendations on minimum dietary diversity for women(15). We defined minimum dietary diversity as women consuming five or more of the ten food groups.
Household wealth index: We constructed the household wealth index using the principal component analysis based on an inventory of the household’s ownership of consumer goods, household characteristics, source of drinking water, toilet facilities and other factors related to the household’s socio-economic status(Reference Filmer and Pritchett16,Reference Poirier, Grépin and Grignon17) . A total of twenty-eight variables were included in the index (sixteen for ownership of consumer goods, three for household characteristics, five for ownership of transport facilities, two for water source and treatment, cooking fuel and toilet facilities, respectively).
Village-level variables: We developed village-level scores to estimate the average village-level access to transportation, crop diversity and crop utilisation. We recoded each household transportation asset (bicycles, motorcycles, cars, light trucks or minibuses and boats) as one (for ownership) or zero (not owned). To construct the village transportation score, we summed these values for each household and then calculated the average of this score for each village. A higher score reflected more transportation assets and, therefore, more opportunities for household members to travel to local markets, district towns and health services.
Each survey recorded farm plot-level crops cultivated by households (with access to land) over the 12 months before the interview (excluding crops in home gardens) to estimate the crop species richness(Reference Jones18). We recoded each crop as one (for cultivation in the last year) or zero (no cultivation). To construct the village crop diversity score, we summed these values for each farming household and then calculated the average of this score for each village. In total, we identified seventy-six different crop species or varieties (e.g. Emata rice - poor quality or Pawsan rice - better quality) cultivated in the survey areas.
We asked respondents about crop utilisation using a five-level scale, from keeping it all for their consumption (value 1) to selling it all (value 5). To construct the village crop utilisation score, we summed these values for each farming household and then calculated the average of this score for each village.
Anthropometric measurements: The same instruments were used for the anthropometric measurements of the mother and child. For weight measurement, we used SECA 874 digital scales (SECA GmbH & Co.KG, Hamburg, Germany) with accuracy to the nearest 0·1 g. we used ShorrBoards with precision to the nearest 0·1 cm (Weigh and Measure, LLC, Olney, Maryland, USA) for height. We took anthropometry measurements twice and a third if the difference between the first two measurements exceeded a predetermined allowable limit. The tablets were also programmed to warn when the recorded values were extreme to alert for a potential error and the need for re-measurement(Reference de Onis, Onyango and Van den Broeck19). Length measurement was done in recumbent position for children under 2 years old and standing position for children above 2 years old. We conducted standardisation exercises for each anthropometrist before collecting the anthropometric data(Reference de Onis, Onyango and Van den Broeck19). We determined the technical error of measurement and systematic error (bias) from the standardisation exercises, and if required, we gave them further training. We used the ‘2006 WHO Child Growth Standard’ to calculate child anthropometric Z-scores - height-for-age, weight-for-age and weight-for-length. We defined stunting, wasting, and underweight as less than –2·00 sd of height-for-age, weight-for-length and weight-for-age, respectively. Children with very low weight-for-height (Z score < –3sd) were referred to the local health department to assess and treat their severe acute malnutrition.
Statistical analysis
We checked the normality of the distributions of continuous variables with the Kolmogorov–Smirnov test. We presented means (±sd) for normally distributed data and median with upper and lower quartiles for the not normally distributed data. We conducted univariate and multilevel mixed-effects Poisson regression analysis to identify the risk factors for stunting among under-five children. We calculated the variance inflation factor (VIF) value for each variable to check the multicollinearity among the independent variables. We included three random effects; one for the township strata, one for the village clusters and another for the repeated measurements of children nested within the clusters. We also used a robust Huber/White/sandwich estimator. We calculated sampling weights to adjust for oversampling of households with children under-five. The weights were based on sampling probabilities and were calculated separately for each cluster and applied in all analyses. We used STATA version 15 for all data analysis.
Ethical consideration
This study was conducted according to the guidelines in the Declaration of Helsinki, and all procedures involving research study participants were approved by the Ethics Review Committee of the Department of Medical Research Myanmar (No.117/Ethics 2015) and the University of Sydney Human Research Ethics Committee. Written informed consent was obtained from all subjects/patients.
Results
We recruited 3231 households in the first-round survey in early 2016 and revisited 90·4 % of the same households in late 2017 (n 2921). A total of 2049 under-five children participated in the first survey and 1696 in the second.
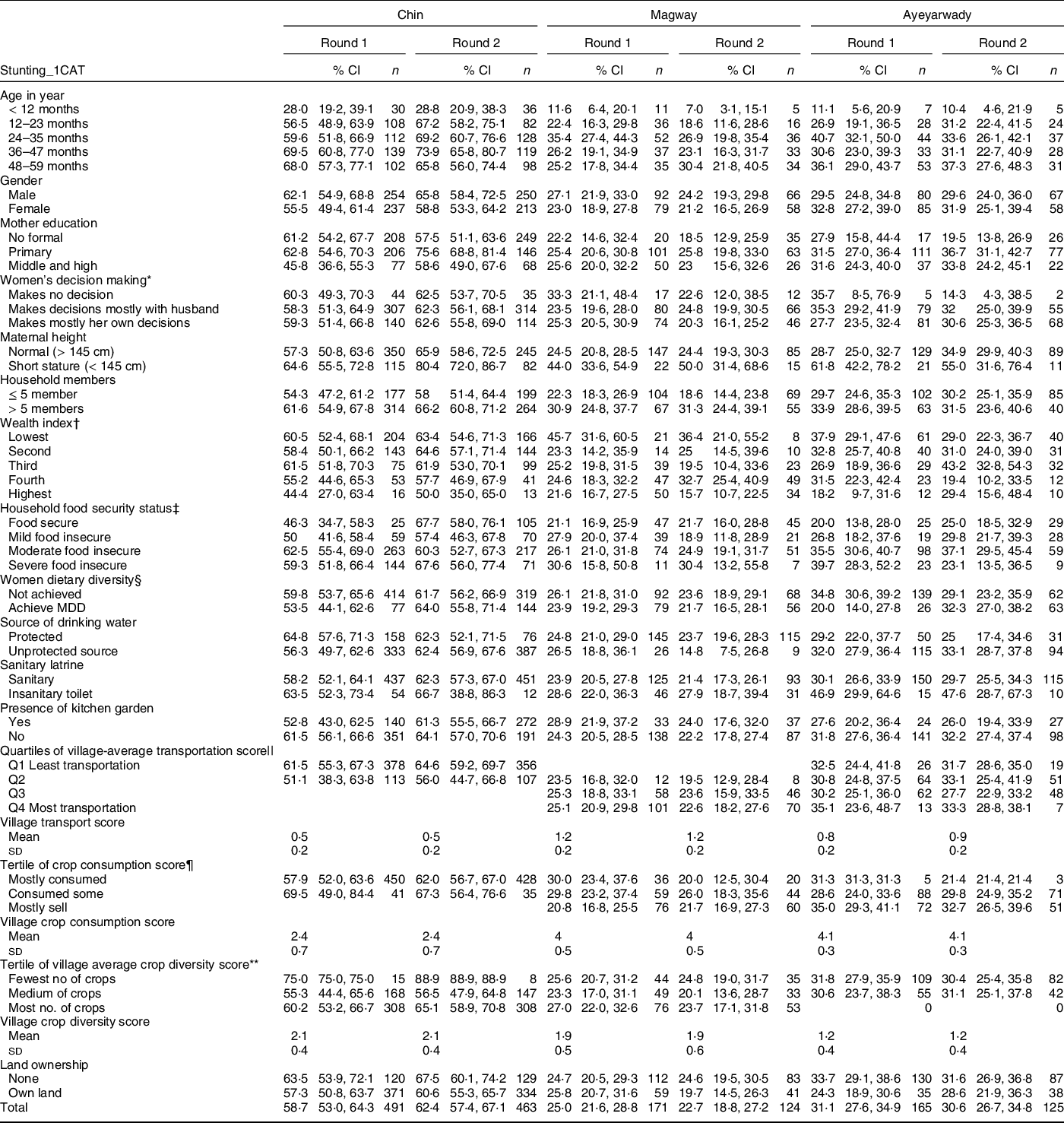
Table 1 shows the background characteristics of the children in each of the two surveys per region. Most mothers had achieved primary education, but most had some role in family decision-making. About 13 % of the mothers had short stature, and about 40 % of the households had more than five family members. Household wealth status remained similar in both survey rounds, but food-secure households increased from 19·6 % in the first to 28·2 % in the second round. The percentage of severely food insecure households decreased between the two survey rounds, from 16·4 % to 9·8 %. The households with women who achieved minimal dietary diversity score (DDS >= 5) tended to increase from 29·5 % to 40·0 % between the two survey rounds.
Table 1 Percent distribution of under-five children by region, survey rounds and selected background characteristics

* Women’s decision-making was categorised into three groups (makes no decision, makes at least six decisions together with her husband or a combination of fewer than six decisions with husband and less than four decisions alone, makes the decision for at least three of the decisions alone and at least three of the decisions with her husband).
†Wealth index calculated by principal component analysis(Reference Filmer and Pritchett16).
‡Household food security was measured by household food security access score (HFIAS)(Reference Coates, Swindale and Bilinsky7).
§Women’s dietary diversity was based on FAO(15).
||Village transportation score estimates village-level access to transport based on household transportation assets.
¶Village crop consumption score was based on how the household used the crops.
** Village crop diversity score was based on the number of crops cultivated by households over the 12 months.
Overall, the prevalence of stunting increased from 40·4 % in the first round to 42·0 % in the second round. In the second survey, the highest stunting prevalence across survey rounds was in Chin State (62·4 %) (Table 2). The prevalence was low among under 1-year-old children but tended to increase by 2 years and older children. The prevalence of stunting among the children was lower if the mothers achieved higher education but tended to be higher if the mothers were short (< 145 cm). Children from higher wealth status and food-secure households tended to have a lower prevalence of stunting. At the village level, having better transportation was associated with a lower prevalence of stunting. On the other hand, children from households that consumed most of their crops had a higher prevalence of stunting.
Table 2 Percent distribution of under-five stunted children by region, survey rounds and selected background characteristics
* Women’s decision-making was categorised into three groups (makes no decision, makes at least six decisions together with her husband or a combination of fewer than six decisions with husband and less than four decisions alone, makes the decision for at least three of the decisions alone and at least three of the decisions with her husband).
†Wealth index calculated by principal component analysis(Reference Filmer and Pritchett16).
‡Household food security was measured by household food security access score (HFIAS)(Reference Coates, Swindale and Bilinsky7).
§Women’s dietary diversity was based on FAO(15).
||Village transportation score estimates village-level access to transport based on household transportation assets.
¶Village crop consumption score was based on how the household used the crops.
** Village crop diversity score was based on the number of crops cultivated by households over the 12 months.
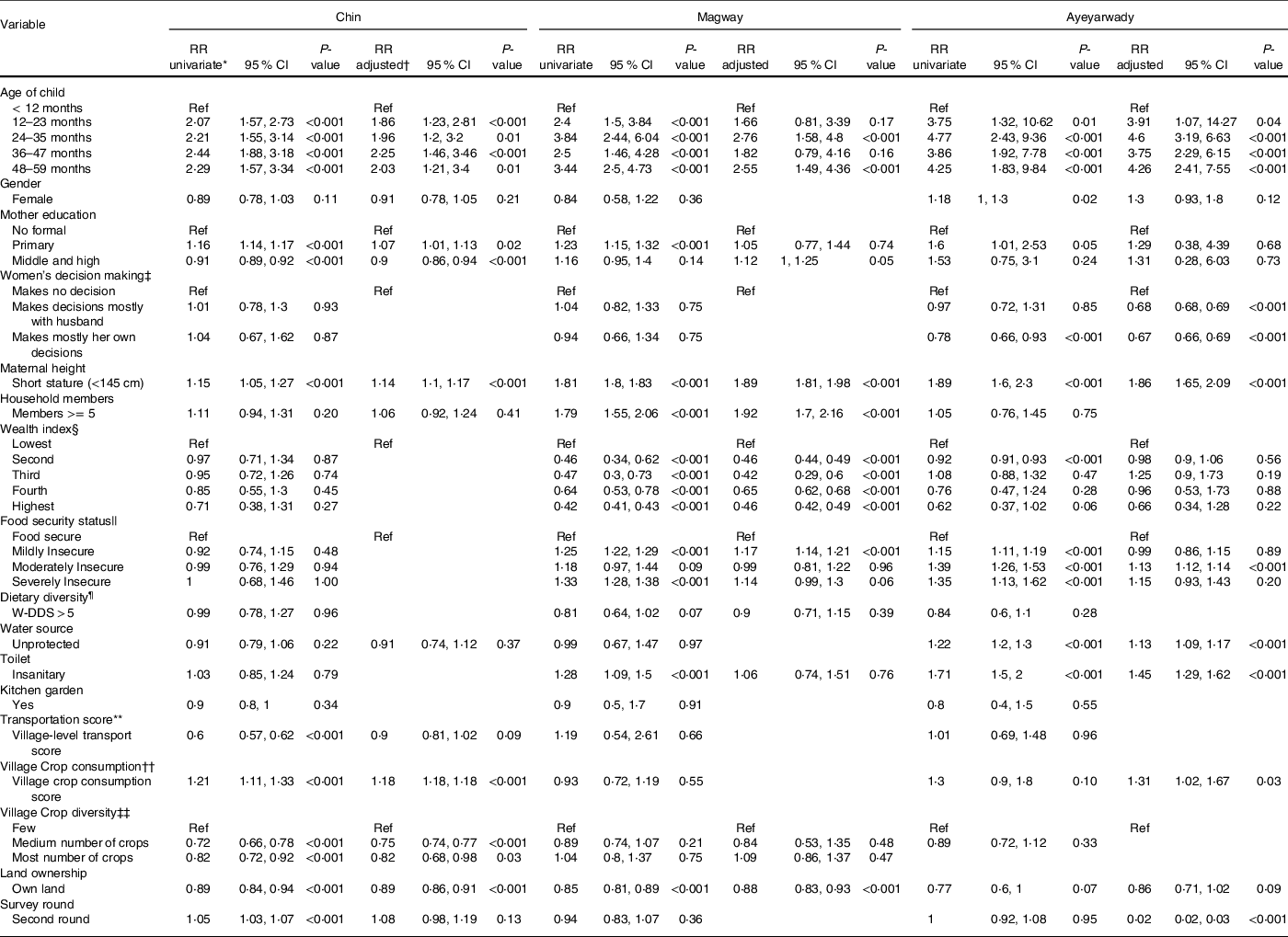
Univariate Poisson regression analysis showed that child age and maternal height were the consistent variables contributing to the risk of stunting among children in all three geographical areas (Table 3). In Chin State, maternal height (RR: 1·14 (95 % CI 1·1, 1·17)) the mother’s educational status (RR: 0·9 (95 % CI 0·86, 0·94) for middle school and higher) and agricultural-related variables such as crop consumption score (RR: 1·18 (95 % CI 1·18, 1·18)) for consuming most of the crops, crop diversity (RR: 0·75 (95 % CI 0·74, 0·77)) for having medium crops and (RR: 0·82 (95 % CI 0·68, 0·98) for having most number of crops) and land ownership (RR: 0·89 (95 % CI 0·86, 0·91)) were important factors associated with stunting in the adjusted model. In the adjusted model for Magway, maternal height (RR: 1·89 (95 % CI 1·81, 1·98)), the number of household members (RR: 1·92 (95 % CI 1·7, 2·1)), wealth status ((R: 0·46 (95 % CI 0·42, 0·49) for highest wealth status), food insecurity status (RR: 1·17 (95 % CI 1·14, 1·21) for mildly food insecure household) and land ownership (RR: 0·88 (95 % CI 0·83, 0·93)) were associated with stunting. Similarly, in Ayeyarwady, maternal height (RR: 1·86 (95 % CI 1·65, 2·09)), women’s decision making (RR: 0·67 (95 % CI 0·66, 0·69)), food insecurity status (RR: 1·13 (95 % CI 1·12, 1·14) for moderately food insecure households), hygiene, sanitation-related variables (RR: 1·13 (95 % CI 1·09, 1·17) for having unprotected drinking water and RR: 1·45 (95 % CI 1·29, 1·62) for having insanitary latrine) and crop consumption score (RR: 1·31 (95 % CI 1·02, 1·67)) were significantly associated with stunting in the adjusted model. The mean VIF value was 1·26, and there was no multicollinearity among the independent variables.
Table 3 Multilevel mixed-effects Poisson models to identify factors associated with child stunting in three regions in Myanmar
* Relative risk for stunting by univariate multilevel mixed-effect Poisson regression analysis, significant at P < 0·05.
†Relative risk for stunting by multilevel mixed-effect Poisson regression analysis, adjusted for covariables, significant at P < 0·05.
‡Women decision making was categorised into three groups (makes no decision, makes at least six decisions together with her husband or a combination of fewer than six decisions with husband and less than four decisions alone, makes the decision for at least three of the decisions alone and at least three of the decisions with her husband)(Reference Ghose, Feng and Tang14).
§Wealth index calculated by principal component analysis from an inventory of household assets and facilities(Reference Filmer and Pritchett16).
||Household food security was measured by household food security access score (HFIAS)(Reference Coates, Swindale and Bilinsky7).
¶Women dietary diversity used recall of at least five out of ten food groups as recommended by FAO(15).
** Village transportation score estimates village-level access to transport based on household transportation assets.
††Village crop consumption score estimates the household’s use of the crops with higher values indicating more selling than consumption of crops.
‡‡Village crop diversity score was based on the number of crops cultivated by households over the 12 months before the interview.
Discussion
This unique panel study followed the same households in two rounds of surveys in rural areas from three agro-climate regions, hilly, central dry zone and delta regions of Myanmar. Among the three regions, we found the highest prevalence of stunting in Chin State, and it increased between the two survey rounds. However, the prevalence was lower in both Magway and Ayeyarwady regions. Factors contributing to the stunting varied across the three regions, but we identified the child’s age and maternal height as consistently associated with child stunting in all regions. In Chin State, village-level variables were important factors related to child stunting; in Magway, it was wealth status, land ownership and number of household members; while in Ayeyarwady, it was women’s decision-making and indicators related to hygiene and sanitation. Food security status improved in all regions between the two rounds of surveys, and in Ayeyarwady and Magway, household food security was an important factor contributing to stunting.
The strength of this study was the geographic coverage since it covered rural areas in three different geographical regions, including hard-to-reach areas in both surveys. The teams successfully followed up with more than 90 % of the households. The panel dataset generated from the study allowed us to compare the food security status, food consumption patterns and nutritional status of under-five children over 2 years in the same households over time. The study identified common factors related to stunting in all three areas and region-specific factors, which are important for planning and implementing nutrition programs in the country. The limitation of the study was that the dietary intake or feeding practices of child, which is the immediate determinants of child stunting, were not collected in both rounds of surveys and thus we could not include these important factors in the analysis models. Distribution of household expenditure was also not collected in the surveys, which could provide a better understating of household-level determinants of stunting. Another limitation was that we could not validate the transportation index in the current study. Nonetheless, we included the variable in the analysis since it was an important factor for identifying the risk of having limited access to food and markets.
The findings from our surveys were consistent with previous national surveys. The Myanmar DHS (2015–2016) reported that the prevalence of stunting among under-five children in Chin state was 41·0 %, the highest in the country, while it was 37·2 % in Ayeyarwady and 25·9 % in Magway(2). Similarly, a nationwide micronutrient survey (Myanmar Micronutrient and Food Consumption Survey MMFCS) conducted in 2017–2018 reported the prevalence of stunting in Chin was 40 %, followed by 37·9 % in Ayeyarwady and 22·4 % in Magway(20). These findings are consistent with our survey results. We also found the highest prevalence of stunting in Chin state, followed by Ayeyarwady and Magway.
However, our results differed from an earlier analysis(Reference Vu and Rammohan21) of the same data used in this study. They reported a negative association between greater diversity of household agricultural production and child nutrition. In contrast, we found a protective effect of crop diversity for stunting in Chin but no effect in other states. We observed higher crop diversity in Chin State, which has the highest child stunting levels. The earlier analysis pooled the data from the three states and may have been confounded by the state of residence. A further difference between our results and the earlier analysis is for kitchen gardens. We found no association between the presence in the household of a kitchen garden and child stunting. In contrast, Vu and Rammohan (2021) reported a protective association(Reference Vu and Rammohan21).
The child’s age was consistently associated with stunting in all study regions, the older the child’s age, the higher the stunting rate. A study in Nepal reported similar findings with child age as one of the significant determinants of stunting, even after adjusting for family size, household headship and household food security status(Reference Adhikari, Shrestha and Acharya22). The most common reason is poor child feeding practices, which leads to inadequate intake of nutrients for the full growth potential of the children, especially through sub-optimal complementary feeding practices. There is a need for counselling on appropriate infant and young child feeding from the start of ante-natal care.
Our finding also showed that maternal height was a consistent determinant of stunting for children among the three regions. This finding demonstrated the widespread existence of an intergenerational problem of undernutrition in the country’s rural areas in all three different agro-ecological zones. To date, not much is known about the interplay between genetics, epigenetics and environmental determinants of stunting. But studies show a strong association between maternal stature and child stunting(Reference Beal, Tumilowicz and Sutrisna23–Reference Titaley, Ariawan and Hapsari25) and suggest it is a strong and reliable maker for assessing intergenerational growth faltering. The finding from a pooled analysis of fifty-four low- to middle-income countries reported that the risk of stunting among offspring of short-statured mothers (< 145 cm) was more than two times higher (RR = 2·132, 95 % CI: 2·103, 2·161) compared with tall mothers(Reference Ozaltin, Hill and Subramanian26). A study from Bangladesh using the dataset of four rounds of DHS surveys reported the risk of stunting was more than two times higher (OR: 2·10, 95 % CI: 1·97, 2·23) among children of the short-statured mothers and confirmed the existence of intergenerational undernutrition problem in the country(Reference Khatun, Rasheed and Alam27). Similarly, a recent paper from Indonesia also indicted that children from mothers and fathers with short stature had almost six times likelihoods of being stunted at birth(Reference Sari and Sartika28).
The study’s primary purpose was to investigate the livelihoods and food security status of households in rural areas of the country during the rapid social-economic transition since the country experienced its democratic period for the first time. Overall, our findings showed that food security improved between the two survey rounds. The number of food-secure households increased from 19·6 % at the first round to 28·2 % at the second round, with more food-secure households in Magway. The adjusted regression analysis showed household food insecurity was an important determinant of stunting for children in Ayeyarwady and Magway, but not in Chin. Ayeyarwady was the most agriculturally productive region in the country, and normally, rice produced from this region is distributed to other parts of the country. However, after the devastating cyclone Nargis in 2008, there was a major impact on the population’s livelihoods, and people in rural areas are still vulnerable(Reference Kostner, Han and Pursch29). Our findings highlighted that the people in the area have still not fully recovered from the consequences of the cyclone and that food security remains a major issue in the area, contributing to an increased risk of stunting among children.
Magway is in the central dry zone of the country, typically characterised by having lower rainfall compared to the rest of the country. We found the number of household members and household wealth status was significantly associated with child stunting in the region. A study in Cambodia has similarly reported the number of household members as the risk factor of stunting. In addition, a pooled analysis of three Cambodian demographic health surveys identified maternal height, child age and gender, parents’ education and household wealth status as the risk factors for stunting(Reference Ikeda, Irie and Shibuya24). Similarly, in Indonesia, a study reported children from households with five to seven members had a higher risk for stunting(Reference Titaley, Ariawan and Hapsari25). These results suggested that children were most vulnerable, especially among households with large family sizes. In addition, our findings showed that household wealth status and land ownership played a significant role in child stunting. This finding was consistent with earlier reports of land and livestock ownership as major determinants of household food security in the dry zone and the association between the ownership of land and livestock and maternal BMI in this arid zone(Reference Sibson30). On the other hand, most of the population in the area does not own land, according to a JICA report(31).
Chin is the hilly region of the country, and most of the population lives in hard-to-reach areas and mainly relies on their self-production of agricultural produce. Access to health care or education is challenging, and as a result, the region is considered one of the least developed areas in the country. It is also prone to rodent infestation, and with each rodent infestation, people suffer from more severe food insecurity, with such events contributing to secular trends in undernutrition. Although our findings showed that food security status was not a significant determinant of child stunting in Chin State, the prevalence of food-insecure households was the highest in Chin State in both rounds of surveys 93·5 % and 79·1 %, respectively. Earlier surveys conducted in 2011–2012 in the same townships (Min Dat and Kan Pat Let) showed more than 96 % of the household experienced food shortages in the past 12 months(Reference International32).
The finding from MMFCS showed Chin and Magway were among the states with the highest rate of food-insecure households, but most households in Ayeyarwady were relatively food secure (77·5 %). In contrast, we found more food-secure households in the Magway region among the three states in both survey rounds. One of the possible reasons was the difference in the sampling of households in MMFCS, which covered a wider population, while in our surveys, the sampling was limited to two purposively selected townships in each region. In Chin State, village-level indicators such as crop consumption score and crop diversity score were significant determinants for stunting of children. In a normal year, farmers in Chin are not self-sufficient, and they are not well equipped with technology and resources to cope with increased erosion and decreased soil fertility(Reference International32). Earlier studies reported access to markets had a stronger relationship with dietary diversity compared to production diversity(Reference Ruel, Quisumbing and Balagamwala33). Better transportation and communication would further improve the livelihoods and eventually the population’s nutritional status.
Mothers are the primary person responsible for preparing nutritious food in the family and play an important role in the nutritional status of children in the family. But in the current study, women’s dietary diversity showed no significant contribution to child stunting, a finding that requires further investigation. A survey conducted among Bangladesh women reported that 58 % of mothers of stunted children did not achieve minimum dietary diversity for women (< 5 groups), and the risk of child stunting was 1·7 times higher compared to those mothers who achieved minimum dietary diversity for women(Reference Hasan, Islam and Mubarak34). The finding suggests that achieving minimum dietary diversity among women is an important factor contributing to child stunting, and it needs more attention in programs. A study from northern Thailand reported widespread food insecurity and that stunted children were less likely to meet minimum dietary diversity(Reference Roesler, Smithers and Wangpakapattanawong35). A study among 15–19 years young women working in the garment sector in Yangon, Myanmar, showed that food security level was one of the risk factors for achieving minimal women dietary diversity score among these women(Reference Goudet, Hlaing and Griffiths36). Our study showed an improvement in women’s dietary diversity in Chin and Ayeyarwardy but not in Magway between the two survey rounds. It is likely that the women’s dietary diversity increased with improved socio-economic conditions, but the lack of improvement in women’s dietary diversity in Magway needs further exploration.
Women’s leadership or decision-making in the family plays an important role in achieving household food security. Our findings showed that most women who participated in the survey hold at least some role in the decision-making process in the family. Using two rounds of DHS surveys, a report from Malawi suggested that maternal autonomy was associated with a lower risk of early childhood stunting(Reference Chilinda, Wahlqvist and Lee37). In our survey, women’s decision-making in the households did not appear as an important contributor to child stunting in Chin and Magway, but interestingly, it was in Ayeyarwady. Background education status of women was comparable across the three states, and distribution of household expenditure could further explain the discrepancies. Findings from Indonesia suggest an association between smoking and food insecurity among poor households as smoking uses some of the household expenses that could be used for food(Reference Semba, Campbell and Sun38). However, this information on household expenditure was unavailable in our study, but it needs further exploration in future studies.
The findings showed a long-standing problem with undernutrition among the rural population, and more comprehensive interventions are required to address maternal and child nutritional problems. Since agriculture is the major source of income generation for the population, improving the agricultural sector is essential to improve the livelihoods and nutritional status of the population in rural areas. Following the democratic transition in 2010, with the support from the international trust fund, a multi-sectoral approach for improving the population’s nutritional status was developed known as the Multi-sectoral National Plan of Action on Nutrition (MS-NPAN)(Reference Siong, Florentino and Noor39). Understanding the importance of the links between different sectors in nutrition, the Ministry of Health and Sports, together with four other ministers (Ministry of Education, Ministry of Agriculture, and Ministry of Social Welfare), endorsed the MS-NPAN. This agreement was encouraging for the country and an important step toward improving the population’s nutritional status since it provided a strong foundation for tackling undernutrition.
As a consequence of the global COVID-19 pandemic, the impact on food security was inevitable worldwide, especially among vulnerable populations due to disruptions of the supply chain and production. In addition, Myanmar people faced another political turmoil magnifying the underlying existence of food security problems amid COVID-19. World Food Program estimates about four million people in Myanmar will face food insecurity in 2022(40). There is an imminent negative impact on decades of hard work and resources to improve livelihoods, food security and child stunting. Policymakers should consider approaches to improve the determinants of stunting, such as improving food security, dietary diversity, women empowerment when implementing National Nutrition programmes and strategies like MS-NPAN, which will tackle the multi-dimensional nature of undernutrition. It may take time to develop a new comprehensive nutrition programme such as MS-NPAN. Nonetheless, in the future, it should consider innovative approaches to breaking the problem of intergenerational undernutrition based on our findings.
Acknowledgements
Acknowledgements: We want to thank all the participants who contributed to the study in both survey rounds. We acknowledge the significant contribution of graduates from the University of Community Medicine, Magway, for their participation in data collection. We recognise the contribution of Prof. Bill Pritchard and Mark Vicol from the School of Geosciences, University of Sydney, Australia, Prof. Anu Rammohan from the University of Western Australia in the development of the original grant and implementation of the surveys. We are grateful for the support of Prof. Khay Mar Mya, Prof. Nay Soe Maung from the University of Public Health, Yangon, and Prof. Htin Zaw Soe from the University of Community Medicine, Magway. We appreciate the support of Prof. Kyaw Swa Mya and Dr. Kay Khine Linn from University of Public Health, Yangon to supervise the field work in Ayeyarwady. Authorship: M.J.D., B.P. and A.R. designed the study, M.K.H., M.J.D., T.W., T.Z., M.P.H. conducted the field work, M.K.H., T.T.D. and M.J.D. analysed the data, M.K.H. and M.J.D. drafted the manuscript, M.K.H., T.T.D., T.W., T.Z., M.P.H., S.R., E.K. and L.M.H. reviewed the paper and provided critical inputs to revise the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Ethics Review Committee of the Department of Medical Research Myanmar (No.117/Ethics 2015) and the University of Sydney Human Research Ethics Committee. Written informed consent was obtained from all subjects/patients.
Financial support:
The Australian Research Council funded the study – grant number DP150102053.
Conflict of interest:
There are no conflicts of interest.





 Open access
Open access