

Whether the fifty insane convicts in Pentonville are of prison manufacture, or have found their way thither through judicial bungling, it is certain that their incarceration in such a place is highly improper.… Their presence in prison must seriously embarrass the officers, and interfere with its regular administration; and the denial to them of medical treatment at the time when it might be of service in rescuing them from lifelong insanity, is a cruel wrong.Footnote 1
By the late nineteenth century, it was widely acknowledged that many insane criminals were languishing in prisons in England and Ireland. However, this statement, appearing in the British Medical Journal (BMJ) in June 1880, was unusually forthright about this state of affairs, with its comment on judicial bungling and claim that the prison could ‘manufacture’ insanity. The article was triggered by the suicide of one of the Pentonville ‘lunatics’, and, describing the special measures that had been put in place to deal with the fifty insane prisoners in Pentonville, its governor explained that twenty cells were under observation, and that many prisoners had been deprived of their tin knives for fear that they would harm themselves. The article went on to state that it was very likely that the discipline of the prison was to some degree responsible for the prisoners’ insanity and suicidal propensities, but also that some prisoners had suffered a miscarriage of justice, being insane at the time of their trial, and ought never to have been Pentonville in the first place.Footnote 2
While highlighted as a pressing issue by the BMJ, the annual report of the Directors of Convict Prisons for 1880, far from being ‘embarrassed’, referred to the suicide in a curt, matter-of-fact manner, without further comment. Prisoner G.77 had committed suicide by hanging himself in his cell. He had been subject to epileptic attacks, sometimes preceded by ‘periods of excitement’, but he had never exhibited any suicidal tendency and his mental condition had been certified as ‘sound’ on his reception into the prison.Footnote 3 It was also reported that over the course of the year nine prisoners had been moved to other prisons as ‘insane’, together with an additional sixteen patients with ‘mental afflictions other than insanity’.Footnote 4
The suicide of prisoner G.77 illuminates the mounting disquiet concerning the mental wellbeing of prisoners and the ‘disposal’ of those suspected of suffering from mental illness, which by the second half of the nineteenth century increasingly preoccupied English and Irish prison administrators and medical officers, psychiatrists working outside of the criminal justice system and the medical press. Questions were raised about how prisons dealt with inmates who developed symptoms of mental disorder following their trial and removal to prison, many of whom appeared to be mentally disordered on their committal. While prison administrators and medical officers were concerned to pinpoint cases of feigned insanity, the subject of the following chapter, and to downplay the deleterious impact of prison regimes on the mental health of prisoners, by the late nineteenth century they too were expressing dismay and frustration at the accumulation of large numbers of lunatics in prisons ill-equipped to deal with them.
The scale of the problem was illustrated in 1889 when the Commissioners of Prisons for England and Wales reported that 349 insane persons had been held in prison that year, of whom 210 had been moved on to asylums. According to Dr R.M. Gover, Medical Inspector of Prisons, as many as 290 were found to be insane on reception.Footnote 5 Gover complained that ‘local prisons … are at present used to some extent as hospitals for the treatment of mental and bodily disease’. As they were not intended or adapted for that purpose, he continued, ‘this practice should as far as possible cease’.Footnote 6 In Ireland the story was similar, though the numbers involved were smaller, and by the 1880s it appears that most insane prisoners were being moved on to asylums. The 1884 Report of the Royal Commission on Prisons in Ireland highlighted, as one of the ‘most serious points’ brought to their notice, the large number of prisoners certified insane in the Irish convict prisons of Mountjoy and Spike Island, remarking, ‘The existence of such an excess ought certainly to have attracted the notice of the authorities to a greater extent than it appears to have done.’Footnote 7 Dr Hercules MacDonnell, Medical Officer at Dundalk Prison, criticised the Royal Commission, however, for its ‘curt dismissal’ of the concerns of witnesses relating to the lengthy detention of lunatics in prisons, noting
It is impossible to conceive any course more likely to prove hurtful to persons who have become insane, than that of subjecting them to the discipline and regime necessary in prison life. These cases require the most skilled personal attention, which it is quite impossible for them to obtain in gaols … and when it is borne in mind that in the majority of prisons there is no adequate provision for the proper nursing of even sick prisoners, it can be readily seen that lunatics must fare very badly.Footnote 8
In 1888, 85 insane prisoners were moved from local gaols to asylums in Ireland and in 1892, 71.Footnote 9 The General Prisons Board complained regularly in their reports about this objectionable state of affairs, a complaint upheld by the Lancet: ‘It is not alone the inhumanity of subjecting lunatics to the unsuitable discipline of an ordinary prison which calls for remark, but also the waste of power involved in providing by means of makeshift arrangements for their safety.’Footnote 10 While the Lancet castigated the Irish prison authorities for their negligence on this score, it is clear that both English and Irish prisons were under enormous pressure to deal with large numbers of insane prisoners in environments unsuited for their confinement.
An impressive literature has explored trial proceedings involving the insanity plea, the role of doctors as ‘expert witnesses’ and the processes of deciding whether defendants were ‘mad’ or ‘bad’, acting under an insane impulse and thus not to be held responsible for their actions or guilty of a criminal act.Footnote 11 As Roger Smith has demonstrated, it became more common over the course of the nineteenth century for medical men to put forward a plea of insanity, though such pleas were not necessarily successful.Footnote 12 Notwithstanding, many defendants were found to be insane prior to or during their trials, and, based on the verdict of ‘not guilty by means of their insanity’, and in Ireland ‘guilty but insane’, moved to lunatic asylums or, after 1850 in Ireland and 1863 in England, to state criminal lunatic asylums at Dundrum and Broadmoor.Footnote 13
This scholarship has, however, focused only in a limited way on the detection of mental illness among prisoners after their conviction and imprisonment, the transfers of prisoners to asylums, and the debates surrounding the appropriate placement and care of insane offenders, many of whom ended up traversing back and forth between asylums and prisons.Footnote 14 Yet, as Janet Saunders has pointed out with regard to England, in addition to decisions reached during trials, the issue of the disposal of mentally disordered offenders became increasingly important after mid-century. Alongside the removal of prisoners labelled as ‘insane convicts’, county and borough asylums became ‘the major receivers of offenders found insane in local prisons’, typically accused of mundane crimes and sentenced to short prison terms.Footnote 15 While prison doctors expressed extreme concern about the number of cases of insanity in prisons, asylum superintendents were up in arms about the clusters of insane criminals accumulating in their institutions, ‘the pests of all asylums’.Footnote 16 They were described as difficult to manage and disruptive for the other patients, at a point when many asylums were under great pressure to admit increasing numbers of pauper lunatics and facing severe shortages of accommodation. Yet at the same time, asylum superintendents were often highly critical of prison medical officers for their failure to detect and move genuinely insane prisoners to asylums where they could receive appropriate care.
Chapters 2 and 3 have demonstrated how concerns about damage limitation shaped policy and practical responses to the treatment of the mentally disordered in English and Irish prisons. Highlighting mental illness and removing prisoners out of the prison system into asylums ran the risk of being interpreted as the failure of prison regimes to improve the minds of prisoners or linked to accusations that the discipline itself had triggered mental breakdown. This was a problem for both the showcase convict prisons and local prisons attempting to implement the separate system as effectively as possible. As Chapter 5 explains, concern about prisoners’ efforts to feign mental illness led to extreme caution in transferring prisoners to asylums, and many prisoners whose insanity was doubted would remain in prison until their sentences terminated. Nonetheless, many prisoners were moved out of prisons, to Broadmoor and Dundrum, or to county, district and private asylums, and it is the mechanisms through which decisions were reached to prompt removals, and the experiences of prisoners who were declared insane following their incarceration that is the main focus of this chapter. For a number of prison surgeons, the business of assessing prisoners began in the courtroom or during the remand process, while for others the mundane processes of diagnosing mental illness and authorising transfers to asylums, and oftentimes back to prison became part of their day-to-day workload.
This chapter is divided into two sections. Section I investigates the series of legislative changes and institutional provisions that were put in place in England and Ireland from early in the nineteenth century to manage the allocation of patients to prisons and asylums, as well as focusing on the courtroom as the site where prisoners declared insane around the time of their trials would, in theory, be sifted out of the prison system. Yet, as explored in section II, many prisoners suffering from insanity continued to be committed to prison, while responses to particular prisoners, the limitations of institutional space and resources, and the diverse actions of individual doctors and prison and lunacy administrators demonstrate that legal frameworks were subject to hugely varied interpretations in practice. Such actions were closely related to prison medical officers’ growing experience and claims of expertise in psychiatry, expressed in both the courtroom and prison, and their ability to assess and diagnose insanity among criminals, as well as their anxieties about how the accumulation of mentally ill prisoners might conflict with their assertion that they were best equipped to deal with such cases. From time to time, as also examined through exploration of a select number of such cases in section II, the regular business of assessment and transfer exploded into high-profile disputes surrounding removals, triggered by insane prisoners arriving in a dreadful state at asylums, with severe injuries or close to death. These cases illuminate the depth of intraprofessional antagonism and completing claims of knowledge and expertise that could arise around the issue of dealing with mentally disordered offenders.
I Provision for Criminal Lunatics and Lunatic Criminals
Accumulating in Prisons and Asylums: Legislative Change and Institutional Provision
The question of where to house the criminally insane taxed prison and asylum administrators from the early nineteenth century. As asylum facilities began to be set up in England and Ireland, accommodating the criminally insane within them presented enormous challenges in terms of the availability of space, governance and their impact on the welfare of the other patients. In England the 1800 Criminal Lunatics Act first made provision for the custody of criminal lunatics, those found unfit to plead or acquitted of an offence on the grounds of insanity at ‘His Majesty’s Pleasure’, which could mean indefinitely.Footnote 17 In effect, however, with no provision for the costs of their maintenance, most criminal lunatics continued to be confined in workhouses or more commonly gaols, often in terrible conditions, where ‘the poor criminal lunatics became objects of sport to their unfeeling fellow-prisoners, by whom they were taunted, ridiculed and tormented’.Footnote 18 In 1808 the County Asylum (Wynn’s) Act authorised counties to set up asylums on a permissive basis with provision for pauper patients and criminal lunatics. It was also recommended that a separate asylum for criminal lunatics be set up at Bethlem to serve the whole country, supported at the state’s expense, and in 1816 two wings opened at Bethlem to accommodate sixty criminal patients.Footnote 19 A few years later it was found necessary to double the accommodation at Bethlem, and in 1849 a separate ward was erected at Fisherton House private asylum for the excess of criminal lunatics.
In 1816 further provision was made to transfer convicted criminals who became insane during their sentences, with a warrant from the Home Secretary, and in 1840 this was extended to unsentenced prisoners and prisoners awaiting execution. Those transferred under these acts were to be certified insane by two magistrates and two medical men, and would only be returned to prison with the approval of the Secretary of State.Footnote 20 These provisions initially applied only to those prisoners who were tried by a jury for more serious crimes, but after 1840 petty offenders showing signs of insanity might be sent to a county asylum.Footnote 21 Even with the absorption of criminal lunatics into the slowly expanding county asylum system (with twenty-four established in England and Wales by 1850), and the expansion of its facilities, Bethlem was overwhelmed by this class of patient, so much so that the Lancet was prompted in 1855 to describe the asylum as a mere receptacle of insane criminals rather than a curative institution ‘into which the waifs of criminal law are swept, out of sight and out of mind’.Footnote 22 In 1857 the Commissioners in Lunacy referred to the indiscriminate mixing of patients without regard for their previous moral and social condition and the ‘skeleton cupboards’ of Bethlem in the form of the male criminal lunatic wards, with its ‘dens … more like those which enclose the fiercer carnivora at the Zoological Gardens than anything we have elsewhere seen employed for the detention of afflicted humanity’.Footnote 23
In Ireland, the 1787 Prison Act and Lunatic Asylum Acts of 1817 and 1821 dealt with ‘the custody of insane persons charged with offences’. In 1821 provision was made for persons acquitted on grounds of insanity or persons indicted and found insane at the point of their arraignment, allowing for ‘safe custody’ in prison, prior to transfer to an asylum under a Lord Lieutenant’s warrant, and specified that ‘the custody of insane persons, charged with offences in Ireland shall be regulated in like manner as in England’.Footnote 24 The persistent accumulation of the insane in prisons had been one of the drivers behind the establishment of district asylums, and Ireland set up its national asylum system earlier than England. By 1835 nine asylums had been constructed, but their capacity to absorb the insane prisoners languishing in gaol was limited. Even as asylum superintendents, such as Mr Jackson of Armagh Asylum, referred in 1828 to the ‘many hopeless cases admitted from the gaols’, criminal lunatics continued to accumulate in prisons.Footnote 25 Particular pressure was felt in Dublin, served by Richmond District Asylum and in the areas covered by the district asylums of Armagh and Londonderry, ‘where the numbers crowding the County Gaols are truly distressing’.Footnote 26 During the 1840s it was proposed that an extra ward be set up at Richmond Asylum dedicated to criminal lunatics, but this was never brought into effect, and by 1849 – swelled by the Great Famine – the number of lunatics confined in gaols had increased to 338.Footnote 27
The situation was complicated in Ireland by the implementation of the Dangerous Lunatic Act in 1838, resulting in a new category, of ‘dangerous lunatic’, making provision for the certification of individuals ‘who displayed a propensity to commit an indicatable crime while denoting a “derangement of mind” and who were perceived to represent a threat to the community’.Footnote 28 This group came to account for the majority of the ‘lunatics’ confined in Irish prisons and asylums, most of whom had not been charged with a criminal offence. The 1843 Report on the State of the Lunatic Poor in Ireland claimed that the number of lunatics in gaols and bridewells had doubled over the previous two years to 214, of whom only forty had been charged.Footnote 29 In England, the same legislation also required two Justices of the Peace to commit dangerous lunatics to an asylum or licensed madhouse rather than a gaol. However, its impact was felt far less than in Ireland, and, when applied, tended to result in asylum admissions rather than confinement in prison.Footnote 30 In Ireland too dangerous lunatics, along with those becoming insane in prison, were in principle to be transferred from prisons to district asylums on the recommendation of two magistrates, who sought medical advice on such cases from local doctors attached to workhouses, gaols or dispensaries. In 1847 Lunacy Inspectors Dr Francis White and Dr John Nugent issued a circular advising all magistrates to seek medical advice, and after 1848 new certification forms were structured to include more medical information, and gaol governors obliged to ensure that the completed form accompanied persons moved from gaols to asylums.Footnote 31 However, until the Dangerous Lunatic legislation was amended in 1867, after which alleged lunatics were to be sent directly to an asylum, the confinement of dangerous lunatics put even more pressure on gaols, where they might be held for lengthy periods given the shortage of asylum accommodation. In 1866 some 685 dangerous lunatics were taken into county and borough gaols, of whom 514 were sent on to asylums. Dublin’s Richmond Bridewell housed 95 male lunatics and Grangegorman 98 female lunatics.Footnote 32 Up until 1867 such practices ‘established an intimate link between insanity and criminality’, associating the lunatic with the ‘degredation of the prison’.Footnote 33 Though some had separate lunatic cells or wards, or even padded cells, many public gaols had no effective means of separating the lunatic from the criminal. ‘The insane were often’, as a result, ‘made the sport of the guilty and subjected to indignities and cruel treatment’, though White and Nugent also pointed out that association with sane prisoners, alongside the removal of alcohol and other prompts to mental breakdown, might be beneficial.Footnote 34
Both the Lunacy Commissioners in England and Inspectors in Ireland lobbied for the setting up of specialist institutions for criminal lunatics in response to constant complaints about the disadvantages of housing them in the prison system, as well as the grave pressures they placed on asylums.Footnote 35 Dr Francis White, who prior to becoming Inspector of Lunatics in 1845 served as Inspector of Prisons with responsibility for overseeing lunatic asylums in Ireland, argued that bringing criminal lunatics together would save expense, increase security and put a stop to the use of district asylums for a purpose that they were never intended to fulfil.Footnote 36 In evidence presented to the 1843 Select Committee he provided many examples of failures within both prisons and asylums, including the case of the female lunatics housed in Grangegorman Prison, where there was an absence of proper accommodation, classification, employment and trained keepers: ‘They are in a most confined Place, and a great Number of them in Strait Waistcoats and muffed, and Two of them strapped to narrow inconvenient Chairs.’ Their presence, White concluded, interfered with prison discipline and in practice they were often cared for by other prisoners.Footnote 37 While eager to assert the quality of prison doctors – ‘they are all clever Men’ – they were unable ‘to devote their Time to the treatment of insanity so much as those who are attached to Asylums’.Footnote 38 Transfer papers and arrangements were also noted to be defective, and prisoners often arrived at asylums ‘in a most wretched and deplorable state’. They were also noted to be more prone to escape attempts.Footnote 39
In England too pressure mounted for the creation of a specialist facility, particularly as county asylums were under increased pressure to admit what appeared to be ever-growing numbers of patients, including in some areas of the country many Irish migrants.Footnote 40 In 1852 the Commissioners in Lunacy (who after 1850 were also responsible for lunatics confined in gaols) claimed that there were 436 lunatic criminals in asylums: 175 in county asylums, 104 in Bethlem, 108 in provincial private asylums, and 41 in metropolitan private asylums, with the remaining eight being held in hospital.Footnote 41 The Report bemoaned the association of criminal lunatics with ordinary patients, to whom they caused pain and disquiet: ‘the Language and Habits of criminal Patients being generally offensive, and their Propensities almost invariably bad’.Footnote 42 According to the Commissioners, they interfered with the routine and discipline of the asylum, with their efforts to feign insanity and to escape, and their bad habits caused insubordination and dissolution among the other patients. They also required stricter custody and strengthened ‘the common delusion that an asylum is a prison’.Footnote 43 Such issues were pointed out time after time by the Commissioners, just as they had been in Ireland a decade earlier, as they repeatedly advocated for a state criminal asylum, reaffirming that mentally ill prisoners were ‘morally tainted with crime’ and ‘unfit for association with the ordinary inmates of Asylums’.Footnote 44 Including individuals who had murdered fellow-prisoners and assaulted attendants, they terrified the other patients, who came to believe that the asylum was a prison, retarding their recovery.Footnote 45
This campaign was supported by eminent asylum superintendents, such as Dr Charles Hood, who, increasingly frustrated about the overcrowding and conditions at Bethlem, initiated its reform.Footnote 46 Dr John Charles Bucknill, superintendent of the Devon County Asylum at Exminster, agreed that Bethlem was clearly inadequate, but suggested (somewhat at odds with the findings of the Commissioners in Lunacy) that the county asylum could be a useful resource for treating carefully selected criminal lunatics, persons often committing minor offences and lacking true criminal propensities, who could be considered as ‘lunatics of criminal disposition’. He also argued that his experience showed him that the other patients could be sympathetic to this class of patient rather than offended by them.Footnote 47 One such case was an agricultural labourer, ‘generally industrious, but was fond of drink, and then liable to committ [sic] all manner of petty offences’. He was also thought to be ‘a little weak in the head’. He was committed to the house of correction for six weeks for indecent exposure and there found to be insane. Taken into Exminster Asylum, his maniacal excitement passed off quickly and he was described as jovial and industrious. After eight months he was discharged recovered by order of the Secretary of State. Three years later the man was again committed to prison ‘for want of sureties to keep the peace’ and then readmitted to Exminster. At this point Bucknill concluded that ‘As he is intensively fond of cider, and as cider causes in him maniacal excitement, the asylum is probably the best place for him.’Footnote 48
Based on his experience at Bethlem, Charles Hood advocated for an improved and specialised state asylum, but also recommended that not all criminal lunatics should be confined together, as this would deter recovery, increase public prejudice and, as a result, create a new ‘bastille’. Like Bucknill, Hood suggested, minor offenders should be placed in county asylums.Footnote 49 Hood also presented accounts of numerous cases confined in Bethlem, who were no longer insane but who he was unable to discharge. Between 1852 to 1858 120 prisoners charged with murder, attempted murder or personal violence were acquitted and seventy-nine of these were received at Bethlem. In a number of cases, no symptoms of insanity had been observed since admission.Footnote 50 In 1857 J.P., an ‘expert thief’, well known to the police in London and the West of England, committed murder in Westminster Workhouse where he was taken suffering from delirium tremens. He was tried and acquitted on the grounds of insanity and removed to Bethlem. At the time of reception, he was, according to Hood, sane and had since shown no symptoms of insanity. An ordinary lunatic asylum was no place for a character with such ‘vicious tendencies’, who had been in prison eleven times, Hood stressed, but neither was Bethlem. ‘Yet though perfectly sane, the doors of every prison are closed against him, and he must remain a tenant of the lunatic asylum, where he produces constant anxiety to those who have the charge of him.’Footnote 51 Similar issues were raised concerning cases of convicts admitted to Dundrum during the first five years of its operation. In some instances their sentences had expired, and others were simply deemed to be inappropriate subjects for confinement in Dundrum, such as Mary Sullivan, sentenced to seven years’ transportation for larceny, who was described as weak-minded rather than insane. Dundrum’s physicians, William Corbett and Robert Harrison, believed that Sullivan, who was unable to speak English, would be better off in an asylum in her native county Kerry, where she would have someone to talk to. Two legal advisors were brought in to provide an opinion on the general situation and concluded that prisoners were entitled to be discharged if recovered, while those still of unsound mind should be restored to the care of their friends or sent to the district asylum.Footnote 52
By the mid-nineteenth century official reports and publications on the challenges of dealing with insane offenders increasingly adopted the terms ‘lunatic criminals’ or ‘insane convicts’ to distinguish this group from ‘criminal lunatics’ who had been found insane prior to or during the trial process. As also reflected in the medical taxonomies discussed in Chapter 3, use of such attributions was by no means consistent, and a crisp division into ‘bad’ or ‘mad’ was not strictly adhered to. While plans were put in place to set up a state criminal asylum in England, Bucknill referred to the problems of trying to sift out criminal lunatics and the implications in terms of institutional care, when those ‘who have become insane from the long indulgence of criminal propensities’ were mixed with ‘those who have become criminal for want of timely protection during their insanity’.Footnote 53 Further complicating the discussion, he expressed concern that many ‘regular insane’ confined in public asylums displayed violent, mendacious and immoral tendencies that made them more unmanageable than many categorised as criminal lunatics.Footnote 54 He described the present system of classifying criminal insanity as ‘arbitrary’, depending upon the manner in which the insanity developed and the persons appreciating its nature.Footnote 55 The English Commissioners in Lunacy and the Inspectors for Ireland described insane offenders interchangeably as ‘criminal lunatics’ and ‘insane convicts’, and the term ‘criminal lunatic’, far from being reserved for those committed to asylums rather than prisons after being found not guilty by means of their insanity, continued to be widely applied to prison inmates who became insane after committal.Footnote 56 Yet there was a push towards differentiating between these two groups in terms of facilities and treatment, Hood urging any new institution to establish rigorous separation between the two classes of patient who had been confined together at Bethlem: ‘The criminal lunatic may be a man of education and refinement brought by the deep affliction of insanity to his present position, or he may be a debased character, a hardened villain, who becomes insane while undergoing the punishment which his crimes have deserved.’Footnote 57
Spurred on by continuing pressure from Francis White, with the support of the Lord Chancellor, who also pointed to the benefits in terms of cost and security, Ireland was first to open a specialised state institution, the Central Criminal Asylum at Dundrum in 1850 (Figure 4.1). In 1845 the Central Criminal Lunatic Asylum Act transferred inspection duties from the Inspectors of Prisons to the Inspectorate for Lunacy, who took over responsibility for the oversight and inspection of asylums, and established a central asylum for insane persons charged with offences. Designed by Jacob Owen, architect to the Board of Public Works who also worked with Joshua Jebb on Mountjoy Convict Prison, Dundrum had provision for 120 patients, 80 men and 40 women, and took admissions directly from court as well as from prisons on the authorisation of the prison surgeon.Footnote 58 With its two divisions, the largest group of inmates were those committing offences while ‘labouring under insanity’, ‘where the disease itself depriving their acts of legal or moral responsibility, condones the criminality’, while the second, less welcome, group, those becoming insane while in prison, ‘not unfrequently bring with them to the Asylum the same obstinacy, impatience of restraint, and perversity of feeling, which had rendered them unmanageable under prison discipline’.Footnote 59 In 1856 twenty-four out of 127 inmates at Dundrum were under sentences of penal servitude.Footnote 60
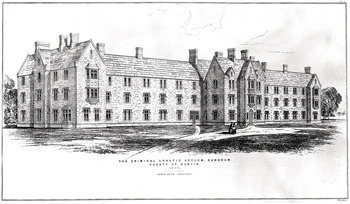
Figure 4.1 The Criminal Lunatic Asylum, Dundrum, Dublin. Transfer lithograph by J.R. Jobbins, 1850, after J. Owen
In 1863 England followed suit with the opening of Broadmoor Asylum (Figure 4.2). Built under the direction of Sir Joshua Jebb, Pentonville’s architect and Chairman of the Directors of Convict Prisons, it was larger than Dundrum, with provision for 100 female patients and 400 male patients. It was also designed to house two classes of patient – Queen’s Pleasure patients, found insane before or during their trial at a higher court, and insane convicts, admitted while undergoing penal servitude – a division reinforced by Dr William Orange, who served as Broadmoor’s second Superintendent between 1870 and 1886.Footnote 61
The first, and by far the more numerous, comprises those unfortunate persons who, in their various callings, have acquitted themselves blamelessly of their duties up to the period when they have become insane; then, under the influence of delusion, and perhaps not watched by those around them, or under a sudden impulse, they commit a crime. The important point to be observed is the sequence of events: first insanity, then crime, the crime being as clearly traceable to the insanity as the effect is to cause. The second class comprises persons whose histories are widely different. It is made up of those who for many years have been habitual criminals, have been frequently the inmates of gaols, whose lives have always been antagonistic to the laws that govern and restrain the rest of mankind. While in prison, these persons are difficult to manage, suspicious of those placed over them, impatient of discipline, insubordinate, and destructive. Sooner or later they are certified to be insane.Footnote 62
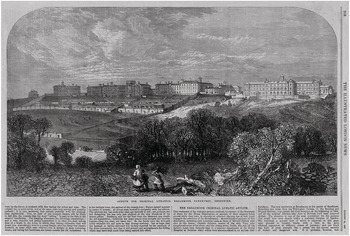
Figure 4.2 Asylum for Criminal Lunatics, Broadmoor, Berkshire, taken from Illustrated London News, 1867
Many of this second class were declared sane or recovered in Broadmoor and were sent back to prison. Those staying in Broadmoor until their sentences expired might be released or moved to another asylum. Following concerns about the number and character of patients transferred from prison and the contamination of the Queen’s Pleasure patients, they were subjected to a harsher regime, and spent more time in seclusion. Feigners were often described as a ‘third class’ of patient, and in both Broadmoor and Dundrum, once identified, moved quickly back to prison. At Richmond District Asylum, which took large numbers of prisoners transferred from Dublin’s local prisons, its Superintendent, Joseph Lalor, adopted a similar division to that established at Broadmoor and Dundrum, into the insane but largely honest, whose offences were caused by their insanity, and the habitual criminal, whose offences were largely part of their everyday life. The former might also be treated in district asylums, even though it was acknowledged that there were great disadvantages in mixing the latter with general asylum inmates. Lalor also suggested that ‘systematic and skilled education and training are obviously called for in the case of all inmates of asylums, who whether from insanity or criminality may be classed more or less as criminal lunatics, and who are prone to breaches of the moral laws’.Footnote 63
Owing to the pressure on Broadmoor, in 1874 a decision was made to incarcerate male lunatic convicts in a separate wing in Woking Invalid Prison instead of Broadmoor, which it was argued offered ‘greater security for safe custody … especially fitted for convicts whose lunacy is sometimes assumed and who are often dangerous’.Footnote 64 However, in 1888, following doubts about the legality of housing insane convicts in a prison rather than criminal asylum (Woking was never appointed an asylum under the Broadmoor Act), this decision was reversed and a new block commissioned at Broadmoor especially for convicts.Footnote 65 Prisoners becoming insane while incarcerated in county or borough gaols, meanwhile, continued to be sent to county asylums, even though many asylum superintendents saw their facilities as unsuitable for dealing with this class of patient.Footnote 66
Dundrum was designed as an institution for lunatics rather than criminals, with the inmates provided first and foremost with asylum facilities and care. Unlike Broadmoor, which imposed a harsher regime on inmates transferred from prison, ‘once within the walls of the Central Asylum no distinction is made in regard of the inmates, every just indulgence being alike conceded to all’, applying ‘those general principles which are now happily established as the foundation of all treatment in cases of mental disease … we have never recognised the merely legal distinction of their criminality’.Footnote 67 Dundrum also quickly became full, and by 1857 was declared ‘practically nearly useless for the disposal of lunatic convicts’, with prisoners being transferred too late to cure them. Instead, as Dundrum was unable to receive them, they were confined in Philipstown Prison, which housed invalid prisoners, under ‘most unfavourable circumstances’.Footnote 68 Meanwhile, local prisons in Ireland tended to send insane prisoners to local asylums.
It was claimed in 1874 that while 25 per cent of Broadmoor’s inmates had been transferred from a convict prison, at Dundrum the figure was just 10 per cent, a decline from 19 per cent in 1856.Footnote 69 The BMJ suggested in 1874 that ‘lunatic convicts’ were found to be troublesome at Dundrum, ‘and as the inspectors have a special fondness for this asylum … they admit as few and send back to prison as many of the convict class as they can’.Footnote 70 Dundrum also reported in the same year on the strains resulting from the custody of the convict class, as they required a higher proportion of attendants; ‘their admission … in some instances constitute an unpleasant and unprofitable addition to the ordinary inmates of the institution’.Footnote 71 Yet diversions from Dundrum could end badly. In 1872 six prisoners were removed from Spike Island public works prison to the Central Lunatic Asylum, two of whom were subsequently sent back to Spike.Footnote 72 In the same year, the Director of Spike Island expressed his regret at the murder of a convict by one of these men when they were employed on public works. Convict Mahoney had been confined in Dundrum but then declared sane.Footnote 73 Following the murder, Mahoney was retried, acquitted on the grounds of insanity and sent back to Dundrum. He was later declared sane, but would not be moved again: ‘There is no doubt danger to be apprehended from the association of such a character with the inmates … one, however, less than were he again to mix with ordinary convicts.’Footnote 74
Discourses of Guilt and Disease: Psychiatrists, Prison Doctors and Mediating Insanity
Embedded in the issue of where to accommodate criminal lunatics was the complex question of assessing lunacy itself, which built on a long history of negotiations in and around the courtroom between ‘discourses of guilt and disease’.Footnote 75 This had produced tensions between psychiatry and the law, as the insanity defence became ‘an important way for the alienists’ claims to expertise and status to be ventured and tested’.Footnote 76 Judges questioned the ability of doctors to delve into and understand the minds of defendants, particularly when invoking pleas of temporary insanity or irresistible impulse. Medical witnesses, meanwhile, expressed frustration when judges and juries ignored psychiatric evidence.Footnote 77 Psychiatry in general was emerging as a more robust specialism, as the number of asylums expanded in the early and mid-nineteenth century and the volume of writing on medical psychology substantially increased. Disputes drawing on medical discourses and diagnoses to validate insanity, and thus non-responsibility for crimes, became common features of trial proceedings at this time, particularly with regard to serious crimes and capital offences. They were also mirrored in debates between magistrates and medical men in local courts in relation to lesser offences where the state of mind of the defendant was in doubt.Footnote 78
However, another set of tensions emerged during this period. As gaol surgeons appeared more frequently as court witnesses after the 1830s, this produced disputes between two sets of ‘expert’ medical witness, with ‘the prison doctor … clearly in the process of assuming the authority which was later to become a decisive factor in so many trials of the insane’.Footnote 79 Just as alienists saw their role as expert witnesses in criminal trials as a means of enhancing their status, so too did prison surgeons, at a time when there was a stepping up of emphasis on mental health as a major component of their work in prisons; through their courtroom interventions, prison doctors had the potential to divert mentally ill offenders away from the prison system. Yet, as Joel Eigen has demonstrated with regard to his analysis of Old Bailey trials in Victorian London, the term ‘expert witness’ was in itself something of a misnomer. While a number of psychiatrists, like Forbes Winslow, John Charles Bucknill and John Conolly, examined defendants and presented in court on numerous occasions and wrote extensively on criminal responsibility and insanity, other medical witnesses might provide testimony in just one or two cases over the course of their careers. Many of these witnesses would have had no particular knowledge of psychiatry, and much medical evidence continued to be based heavily on the accounts of lay witnesses.Footnote 80
According to even experienced medical witnesses, the problem of assessing prisoners whose mental condition was in doubt began pre-trial, with prisoners only being visited a couple of times by physicians for assessment before their court appearance. In cases taking many months to reach court, treatment would also be delayed with disastrous consequences.Footnote 81 Additionally, the process ‘pitted’ doctors against each other in the courtroom, while the medical evidence often failed to provide good guidance for the jury. In Charles Hood’s words,
A few hours, perhaps less, are all that is allotted, and he is hurried into the witness-box to state before a learned judge, an astute and adverse counsel, and a perplexed jury, the ground of the opinion he has formed, usually involving some of the more delicate questions of psychological science.Footnote 82
In response to the pressures experienced at Bethlem, Hood also advocated for a more speedy process for moving patients who were found to be no longer insane back into the criminal justice system.Footnote 83 Meanwhile, in 1851 Inspectors Francis White and John Nugent questioned the process of acquittal itself in Irish cases involving the insanity plea: ‘If there are extenuating circumstances connected with the psychological condition of the accused, they are legitimate subjects to be considered in meting out the after punishment, but certainly not in the first instance for an unqualified acquittal.’Footnote 84
The term ‘Criminal Lunatic’ itself was also something of a misnomer, running against the principle of not guilty by reason of insanity, and its meaning continued to be debated throughout the second half of the century, complicating the issue of where to place criminals who were also mad.Footnote 85 In 1883 William Orange argued that it was impossible to be guilty of a crime and a lunatic at the same time, as the latter could not be held responsible for their criminal act. He added that ‘The evils of sentencing persons who are really insane to penal servitude or imprisonment, are much graver than is commonly supposed’:
If the punishment is to be carried out in its entirety it necessarily involves much suffering … whilst if the sentence is not to be carried out thoroughly, but if the understanding is that it is to be modified in its severity, so as to suit the mental condition of the prisoner, it were surely better, in doubtful cases, not to pass sentence until after a satisfactory examination of the mental condition of the prisoner had been made … every instance in which a prisoner is found, on his trial, to be insane acts as a reminder to the community that, little or much, it has failed in its duty in not having prevented the commission of the crime by placing the prisoner under proper care at an earlier date.Footnote 86
Orange went on to suggest that in an ideal society,
the class of criminal lunatics would disappear, because no-one would be sentenced to punishment without his mental state being ascertained before sentence, instead of, as now so generally happens, afterwards; and, furthermore, because persons known to be insane would then be placed under control before, and not, as now, after they had committed some alarming act of homicide or violence.Footnote 87
He recommended bolstering the process of assessment around the trial and that a prisoner charged with a crime and suspected to be insane should be examined by the prison medical officer, a local asylum superintendent, and additionally by a ‘physician of standing’, as soon after the crime had been committed as possible.Footnote 88
Prison doctors might dispute the verdicts of psychiatrists based on their observations of prisoners pre-trial, though in other instances they drew the same conclusions concerning the defendant’s state of mind. The medical evidence ‘intended to show the defendant as sane and responsible’ was likely to rely less on deviant acts, but ‘simply on an absence of signs of insanity while remanded in prison’.Footnote 89 Gilbert McMurdo, surgeon to Newgate Gaol in London, gave evidence in numerous Old Bailey trials between the 1830s and 1850s, making him the most frequent medical witness to testify at insanity trials over that period.Footnote 90 McMurdo emphasised that he saw many cases of lunacy and was able to closely observe prisoners suspected of being mentally disordered, having almost daily interactions with them.Footnote 91 In 1854, he concurred with the opinion of Dr Forbes Winslow in the case of Hugh Pollard Willoughby, who was accused of wounding with intent to murder, that he was insane and suffering a ‘horrible delusion’. In giving evidence McMurdo explained, ‘since the day the prisoner was committed to Newgate I have continually seen and conversed with him – I happened to be in the prison immediately after he was taken there, and I saw him then – I am of opinion that he was then, and is now, of unsound mind.’ Willoughby was found not guilty and ordered to be detained.Footnote 92
One year later, however, McMurdo’s evidence was key in condemning Luigi Burinelli to death, following his Old Bailey trial for murder. There was a wealth of medical evidence in this case, and while it was agreed that Burinelli had suffered badly from internal piles, which had been treated in Middlesex Hospital, and was acknowledged to be in very poor spirits and melancholic following the death of his second wife in childbirth, McMurdo testified that under his observation at Newgate he had shown no symptoms of aberration of mind, but was suffering from hypochondria. John Conolly, along with other medical witnesses, disagreed, arguing that the defendant was of unsound mind and delusional. McMurdo, while he did ‘not profess to be what Dr. Conolly is, set apart to that part of the profession’, reaffirmed in giving his evidence his vast experience as prison surgeon:
I have had a great many persons, about whose state of mind inquiry has been made, or was made, under my care during my tenure of office, for a considerable time – I have been surgeon to the gaol of Newgate for twenty-five years, and I have had a great many under my care; some who have been of unsound mind, some who have been thought to be so.Footnote 93
Joel Eigen has argued that unmasking fakery was the primary goal of the prison surgeon.Footnote 94 However, beyond that, McMurdo appeared to be very concerned to assert his experience in detecting mental disorder based on daily observation and his lengthy prison career.
By the late nineteenth century the trial hearing had become a key interface where claims of insanity were disputed by prison doctors and psychiatrists working outside of prisons, and the medical press reported avidly on such proceedings. Such reports could be critical of prison surgeons’ testimony when this went against that of eminent alienists.Footnote 95 Tensions flared, for example, in a case tried in York in 1859, reported across several issues of the BMJ and in the Dublin Medical Press, when Mr Anderson, surgeon of York Gaol, sided with the counsel for the prosecution who had advised the jury to reject the opinions of three eminent medical witnesses. The three, including Dr Forbes Winslow, claimed the defendant, James Atkinson, who was charged with murdering his sweetheart, was an obvious case of insanity and ‘an imbecile’ with the intelligence of an eight-year-old child. Anderson declared that he did not think those gentlemen were better able to give an opinion on questions of lunacy than himself.Footnote 96 In August 1884, in another widely reported trial taking place in Dublin, the dispute centred on whether James Ellis French was fit to stand. Several medical men, including Dr Eames, Medical Superintendent of Cork District Lunatic Asylum (labelled by the Lancet as the ‘only specialist’), claimed that he was not in a mental condition to plead and conduct his defence with due caution. Three other doctors, including Dr McDonnell, claimed there was nothing wrong with French physically or mentally, and that he was shamming.Footnote 97
While serving as medical officer at Mountjoy Prison, Dr Robert McDonnell provided a candid assessment of the difficulties involved in making such assessments:
There is not a medical officer of a lunatic asylum, or of a prison in this country, who will not admit that, in many cases, to discriminate with precision between wickedness and madness is a task too difficult as to be often absolutely impossible, and that, too, after months of close and careful daily observation.Footnote 98
He added that half of the medical witnesses knew something of the prisoner and nothing of insanity and half knew something of insanity but nothing of the prisoner.Footnote 99 He was not surprised that many persons of unsound mind were found in convict prisons. Nonetheless, while the judge and jury system could not assess such cases ‘with the delicacy of a chemist’s balance’, and medical witnesses dealt not in certainties but ‘probabilities’, he pointed out that grave errors had been made, as in the case of Burton, tried at Maidstone and executed for the horrific murder of a boy. In McDonnell’s view Burton was clearly a madman.Footnote 100 Burton had declared that his only motive was that he wanted to be executed, and it was discovered that his mother was ‘a madwoman and his brother of weak intellect’.Footnote 101 In this case it was a prison surgeon who had gone ‘a long way towards banishing the idea of the prisoner’s insanity from the minds of judge and jury’. ‘He stated that he had observed the prisoner ever since he had been placed in confinement, that he appeared sane, nor did he observe that he was under any delusion.’Footnote 102
Though psychiatrists working outside of prisons were widely consulted in trial proceedings, in effect it was prison doctors who had most contact with prisoners on remand, many of whom showed symptoms of insanity or were regarded as suicidal. Magistrates sent those suspected of insanity to the local gaol for assessment by prison surgeons and in Ireland prison or dispensary surgeons; the latter were often already familiar with the patient’s history.Footnote 103 In contrast to the ‘expert witness’ in court who had seen prisoners just once or twice, prison doctors were ‘schooled in multiple observations’.Footnote 104 It was particularly in remand prisons (including numerous local prisons in England and Ireland) that prison medical officers built up impressive levels of experience dealing with mentally ill offenders, assessing the state of their minds pre-trial, and taking care of prisoners who had a high risk of suicide.Footnote 105 Prison doctors employed in remand prisons were particularly likely to assert their expertise in assessing mental illness, at the same time underlining their heavy workload. At Clerkenwell Prison in London, the medical officers had extensive dealings with suspected cases of insanity and attempted suicides. In 1859 alone a total of 107 attempted suicides were reported, who were placed under close observation by Clerkenwell’s surgeon Henry Wakefield.Footnote 106 Cases of temporary insanity caused by drinking were frequent that year and additionally thirty cases of suspected insanity were sent from various London police courts, ‘calling the surgeon’s attention to the state of the Prisoners’ mind, and requiring Certificates of his opinion; this duty involves a serious responsibility’.Footnote 107 Many prisoners were moved to asylums before their trial or were acquitted on the grounds of insanity and then transferred to asylums. Clerkenwell’s prison surgeons worked closely with local asylum superintendents, including Charles Hood at Bethlem and William Sankey at Hanwell, to obtain further assessments on the mental state of prisoners and to organise removals. In February 1860, for example, Elizabeth Livermore was charged with unlawful assault and attempting to stab her victim with a knife. She was acquitted on the grounds of insanity and sent to Clerkenwell to be kept under strict custody, before being removed on the order of the Home Secretary to Colney Hatch Asylum.Footnote 108
II Criminal or Lunatic? Prisoner or Patient?: Places and Practices of Confinement
Removals between Prisons and Asylums
Decisions concerning the state of mind of prisoners prompted removals back and forth between the prison and asylum, and preoccupied prison and asylum officers throughout the nineteenth century. Processes of removal between institutions were much more than administrative exercises, and a great deal was at stake in determining the placing of lunatics who had committed crimes in terms of the welfare of individual prisoners, institutional wellbeing and management, cost, intraprofessional relationships, the assertion of specialist knowledge and authority, and the very definition of criminal lunacy itself. The ambivalent position taken by asylum doctors has already been referred to, concerned as they were about the impact of mentally ill offenders in asylums, yet also critical of their retention in prisons. Prison doctors too were ambivalent. Along with asylum doctors, they shared a concern to remedy what was increasingly depicted as a disastrous situation for the prison system and the numerous mentally ill prisoners held within it, and, as Robert McDonnell indicated, were likely to find the state of mind of prisoners extremely difficult to assess. However, they were also keen to underline their growing knowledge and expertise, and ability to produce an accurate diagnosis. By the late nineteenth century, as shown in Chapter 3, not just those working in remand prisons, but prison medical officers more generally were expressing confidence about undertaking this work, and were spending a far greater proportion of their time dealing with mentally disordered offenders. In 1869 the Howard Association, expressing concern about ‘the fact’ that many victims of mental disease were exposed to ‘penal treatment’, quoted figures showing that one in nine prisoners was more or less insane at Perth Prison, while in 1870 Perth’s medical officer, Dr James Bruce Thomson, estimated that 12 per cent of the Scottish prison population were ‘mentally weak in different degrees’, noting that similar rates were reported in English and Irish prisons.Footnote 109 Dr Charles P. Measor, late Deputy-Governor of Chatham Convict Prison, also claimed in 1869 that his ‘experience of convicted criminals induces in me a strong conviction that the amount of mental disease actually existing among them is inadequately appreciated’, while he was aware that as many as 5 per cent of inmates of an Irish convict prison were confined in separation under medical observation with a view to ascertaining their mental condition, ‘quite exclusive of a large proportion who might be said to have possessed inferior degrees of irresponsibility’.Footnote 110
Managing mentally disordered prisoners, as demonstrated in Chapter 3, was doubtless a significant part of all prison doctors’ workloads, particularly as cases were retained in prison when officials were unable to decide – or agree – on their state of mind. If cases of mental disorder were missed at the trial and the prisoner sent to a prison rather than the asylum, this added to the responsibilities of overburdened prison medical officers as they attempted to assess and deal with mental illness in a punitive environment lacking in therapeutic resources. Medical officers were often slow to initiate transfers to asylums, because their heavy workload hindered this, and also as it indicated the failure of the institution to manage the mental health of its prisoners and the detrimental impact of prison regimes on their minds. These factors might vary depending on local circumstances and the type of prison involved, and the weighing up of the disruption such prisoners created against the trouble of moving them. Bucknill observed how,
In the new gaols for separate confinement a noisy lunatic proves such a nuisance, from the reverberation of his cries through the resonant structure of the building, that every effort is sure to be made to have him transmitted to an asylum without delay; but this evil is not felt in the old prisons, nor in the new ones with silent or melancholic patients.Footnote 111
The destinations of many insane prisoners were governed in the first place, not by prison or asylum doctors and administrators, but by the actions of local magistrates. Both the Commissioners in Lunacy and Inspectors complained that lunatics committing minor offences were sent by magistrates to prison, and their insanity ignored, or were passed over to the Poor Law authorities, though it was suggested that there was some merit in the latter arrangement, as many such cases were regarded as ‘ordinary lunatics’ who had not been properly looked after and were rarely of the criminal class.Footnote 112 What came to be described as ‘magisterial dumping of the insane’ was largely prompted by cost considerations, as workhouses and asylums, unlike prisons, were supported by local rates, with maintenance costs in the workhouse being much lower than asylums.Footnote 113 Meanwhile, the certification process for asylum admissions was expensive and time-consuming. In Ireland the Prison Inspectors’ Report for 1868 described how circulars had been issued in 1807 and then again in 1868, enclosing forms for the committal of lunatics to asylums, yet it was found from returns and on inspections of gaols and bridewells that magistrates still committed insane persons to prison, ‘thus, besides the injury inflicted on the individual, seriously interfering with the discipline of the gaols’.Footnote 114
At the local level, a series of cases reported to the magistrates of the West Riding of Yorkshire in 1860 demonstrated how complex the dispersal of prisoners showing symptoms of mental disorder ended up being, involving transfers between prison, asylum and workhouse.Footnote 115 In April 1860 James Jenkins, a blademaker, was committed to Wakefield Prison for four months for the theft of steel. His ‘friends’ reported that he had been leading an ‘unsteady’ life before he was sent to prison and had showed ‘a strangeness of mind indicating insanity’. Once in prison the surgeon came to a similar conclusion. The prisoner’s insanity was reported to the Secretary of State, and he was removed in August 1860 to the West Riding Lunatic Asylum.Footnote 116 Inquiries into the dispersal of prisoners were also made at the end of their sentences. In May 1860 Robert South was removed to Wakefield House of Correction as a ‘disorderly pauper’. At the end of his three-week sentence the prison surgeon, William Wood, reported that, while nothing had occurred during his imprisonment to warrant removal to the asylum, when he was sent on to Sheffield Workhouse the institution’s medical officers were warned to pay ‘special attention to the state of his mind as his Conduct has been such as to create a strong suspicion that he is a Lunatic’. Robert South was transferred a few days later to the West Riding Asylum.Footnote 117
A memo to the West Riding justices a year later explained the ‘great inconvenience’ resulting from the actions of local magistrates in committing persons charged with offences who were in a state of insanity or mental imbecility to the Wakefield House of Correction. Such persons, the memo complained, caused much trouble to the prison officers, interfered with the discipline of separate confinement, and later put the county to considerable expense and trouble in removing the individuals to an asylum, and obtaining an order of maintenance after establishing which parish was responsible for payment. They urged the magistrates ‘where a person was manifestly an idiot or insane at the time of committing felony or indictable misdemeanours’ to send them directly to a lunatic asylum.Footnote 118 However, as Saunders has pointed out, magistrates were under considerable pressure to make rapid decisions, and the Home Office might have believed that magistrates were sending insane offenders to prison for careful observation by the prison doctor, which would result in a more informed decision about where to send such individuals than their own hasty diagnosis.Footnote 119 Both Cox and Saunders have also argued that magistrates might be well informed on the subject of insanity, involved as they were in making arrangements for the medical examination of suspected lunatic prisoners, while many were also members of asylum visiting and management committees, and, as such, aware that local asylums were short of space, security and staff.Footnote 120
The advisability of moving criminals from prison once they were declared insane also divided opinion. Charles Hood proposed that if a criminal became insane after sentencing, ‘he should be put into a lunatic ward connected with the infirmary of the prison in which he may be confined, and there treated by the officiating surgeon in the same way as if he were suffering from any other disease’. Though Hood suggested elsewhere that minor offenders who were insane might be sent directly to county asylums, he argued that ‘the practice of sending insane prisoners from gaols to county asylums is, in every point of view, objectionable’.Footnote 121 Hood also observed that ‘the medical officers, connected with our public prisons, are men of undoubted professional skill and experience … fully competent to deal with a disease which may, it is well known, by active treatment, be cut short in its early stages’.Footnote 122 Such prisoners, he added, would be closely supervised by the Commissioners in Lunacy whose duties included visiting gaols where lunatics were held.Footnote 123
During an inquiry into the operation of Broadmoor Asylum in 1877, it was also suggested (albeit by means of a minority opinion) that convicts becoming insane after conviction might be better off in lunatic wards in prison, where they would have the possibility of employment, describing the atmosphere in prison as less ‘depressing and desponding’ and presenting more hope for the future than in an asylum.Footnote 124 The conditions for some of Broadmoor’s patients appear to have been woeful, with disruptive patients placed in seclusion and several, exceptional for their ‘dangerous violence’, held for many months in large cages. A number of these had attacked Broadmoor attendants, including W.T., admitted from Millbank Prison in 1867. Sentenced to fifteen years’ penal servitude, his conduct in Woking, Portsmouth and Dartmoor was described as ‘bad’, and he had escaped from Portsmouth Prison in 1865. W.T. had been kept in a strait waistcoat and hobbles for some time before admission to Broadmoor, and in January 1868 he attempted to attack the attendants and take their keys, then in September bit an attendant’s leg.Footnote 125
While many claimed expertise in dealing with mental illness, prison surgeons might have a very different perspective on the best place to confine such cases, particularly when prisoners were violent or for those working in poorly resourced local prisons. Surgeon Read, referring in 1862 to the confinement of lunatics in ordinary (local) prisons in Dublin, emphasised how the imprisonment of lunatic prisoners, including ‘the violent maniac, the feeble and the imbecile’, had been a heavy responsibility for him for the past twenty years:
The consequences are rendered apparent in sanguinary incidents, loss of life, and the most perilous operations of surgery. This blood-stained scene is a blot on humanity, as well as an extravagant impolicy; in fact, an institution for converting derangement into permanent insanity.… Every Board of Superintendence for many years has deprecated the principle of committing insane persons to prison, and they have made increasing representations of the violation of prison discipline consequent upon their confinement therein.Footnote 126
There were also resource implications. Over the year 1861 the number of lunatics confined in Richmond Bridewell alone rose from eighteen to thirty-four, making it necessary to employ an additional warder to supervise them.Footnote 127
In effect, by the second half of the century prisons, criminal lunatic asylums and public and district asylums were all housing large numbers of criminal lunatics. In England around 50 per cent of the total were accommodated in public asylums, ensuring that their medical officers had extensive (and often unwelcome) experience of dealing with this group. In 1863, 419 of the total of 877 criminal lunatics were held in custody in county or borough asylums. By 1880, when the total number of criminal lunatics and ex-criminal lunatics in England was 1,288, public asylums held 720 of them.Footnote 128 In Ireland the situation differed in a number of respects. Though there were continued complaints about the strains the mentally ill put on both prisons and asylums, the number of criminal lunatics was smaller, and by the 1880s most lunatic prisoners were being moved on to district asylums. In 1866 eight prisons were declared to be the ‘most encumbered’ with criminal lunatics, with 315 lunatics between them. However, it was suggested that two new asylums at Letterkenny and Castlebar would clear the gaols of most of their lunatics, and with further asylum expansion elsewhere, ‘the prisons in Ireland will virtually cease to be as heretofore receptacles for the insane’.Footnote 129 In 1868 a total of 69 criminal lunatics were confined in Irish gaols. Of these, twenty-six were moved to Dundrum, twenty-nine to district asylums, five were discharged by the Lord Lieutenant to the charge of their friends, seven, largely committed as vagrants, were discharged by order of the magistrates, and three remained in gaol at the end of the year.Footnote 130 Of the 99 lunatics confined in Irish gaols in 1879, eighty-nine were moved to district asylums and ten were discharged by the Lord Lieutenant. This figure included fifty-three who were under sentence of imprisonment or transportation who became insane in gaol, fifty-two of whom were moved to district asylums while one was discharged.Footnote 131
After 1867 county and district asylums had to accept from either state asylums (Broadmoor and Dundrum) or convict prisons certified criminal lunatics whose sentences had expired and could only be detained thereafter as pauper lunatics. This must have been welcome in Broadmoor, which in 1865 had admitted 50 convicts from Chatham, 59 from Portsmouth and 64 from Portland, bringing the total number of lunatic convicts to 266, and in 1868 Broadmoor removed 134 patients whose sentences had terminated to county asylums.Footnote 132 Lunatics, however, who had been retained in the prison system without medical certification could be released at the end of their sentences. In October and November 1874 two ‘dangerous lunatics’ were sent from Millbank Prison to the St George Union Workhouse. Shortly after, one, John Maloney, escaped and the other, Henry Balls, discharged himself. It was reported that neither while in the workhouse showed any symptoms of insanity.Footnote 133 The Lunacy Commissioners and Home Office expressed grave concerns about the discharges, underlining the unsuitability of workhouses for confining dangerous lunatics. Rather, the Lunacy Commissioners proposed that ‘they should with all possible dispatch be placed in a lunatic asylum’, and also questioned why the two men, as dangerous lunatics, were not sent directly to an asylum rather than a prison. The Broadmoor authorities and asylum superintendents, meanwhile, continued to object to the mixing of criminals with lunatics, while Du Cane and the Home Office were keen to retain the penal emphasis with regard to lunatic criminals, and in 1875 the opening of the lunatic wing at Woking appeared to resolve the issue. Male ‘prisoner lunatics’ were to be retained there, with fewer ‘indulgences’ than Broadmoor and outside the authority of the Lunacy Commissioners.Footnote 134
In Ireland the 1875 Lunatic Asylums Act confirmed that lunatics removed from prison or from Dundrum to a district asylum were to be treated as ‘ordinary patients’ and charged to their local district, and were to be subsequently retained or discharged on the authority of the asylum governors.Footnote 135 Broadmoor’s medical superintendent, William Orange, had suggested in 1870 that such a flow was vital to create space for insane convicts in the specialised criminal lunatic asylums who otherwise would be retained in prison ‘not only to their own detriment, but also to the detriment of the sane prisoners’.Footnote 136 The 1877 Prison Acts authorised central government to take over the running of local prisons in England and Ireland in addition to their funding, but local ratepayers were to continue to support lunatics and criminal lunatics in asylums.Footnote 137 This provided a major incentive for magistrates to keep sending offenders suspected of lunacy to prison, with some 621 being removed to local prisons in England in 1883 on suspicion of insanity, which in most cases in the view of the Prison Commissioners ‘was virtually certain’.Footnote 138 The prison authorities, they continued, were put in a particularly difficult position when medical officers reported prisoners to be insane but the magistrates declined to provide a certificate for removal to an asylum, ‘and it is a question whether in such a case a prisoner should not simply be discharged’.Footnote 139 The Prison Commissioners and Inspectors in Ireland protested regularly about this kind of situation, arguing that prison was not a proper place for those whose insanity had been questioned, given the need for special experience and treatment, ‘and it cannot be expected that such experience should be available in prisons, more particularly in the small prisons which form the large majority’.Footnote 140
In England the 1884 Criminal Lunatics Act bolstered the role of the Secretary of State in the certification and transfer of criminal lunatics from prisons to asylums.Footnote 141 This was in response to mounting pressure from asylum doctors attempting to get rid of dangerous patients, as well as local authorities wanting to be relieved of the burden of maintaining ‘quasi-criminal’ asylum inmates. It was also prompted by the Home Secretary Sir William Harcourt’s concern about the lack of allowance within the criminal justice system for mentally incapable offenders and prisoners, and the 1884 Act extended provision to certify prisoners not just as lunatics, but as suffering from ‘imbecility of mind’ that made them unfit for penal discipline.Footnote 142 This coincided with the stepped-up use and success of the insanity plea more generally, with The Times suggesting in 1882 that the notion was spreading that ‘there must be something wrong in a man’s mental organization before he could have committed a certain crime in certain circumstances’.Footnote 143 Harcourt transferred more prisoners than previous Home Secretaries to Broadmoor without trial, and under the 1884 Act all prisoners sentenced to death were to undergo medical examination ‘to ensure that no lunatic was executed’.Footnote 144 The Act made the Prison Commissioners responsible for the maintenance of prisoners moved to lunatic asylums – prior to that they had only been liable for those for whom a place of settlement could not be ascertained or those committed with very short sentences – and also included provision for interventions in prison regulations on behalf of those suffering ‘imbecility of mind’, though in practice few prisoners were placed in this category.Footnote 145 The 1884 Act encouraged the removal of Broadmoor patients whose sentences had expired to asylums, with twelve transferred in 1885 to English county asylums and ten to Dundrum, for subsequent distribution to district asylums in Ireland.Footnote 146 However, it also provided for the retention of criminal lunatics in Broadmoor upon a medical officer’s certification that they might be dangerous, care being taken to select for transfer those ‘not likely to cause annoyance’.Footnote 147
With costs now borne centrally, magistrates continued to send suspected lunatics to prison for medical observation, and their numbers increased dramatically, from averages of 8.2 and 11.9 per 1,000 committals between 1870 and 1882 to 18.2 per 1,000 between 1884 and 1889, with the number for 1889 rising to 22.8.Footnote 148 In 1885 Harcourt complained that the common practice ‘of using a prison as a place in which a supposed lunatic can be confined in order to ascertain his mental condition certainly calls for alteration’, though it was claimed that charging a person with a crime was the only way to keep a person in custody before being ‘certified’.Footnote 149 It was also regarded as crucial that the prison authorities took on the costs of supporting insane offenders in asylums, in order get rid of a class of prisoners ‘who encumber the gaol & interfere with Discipline’.Footnote 150 In 1889 the Home Office issued instructions to magistrates to send mentally ill offenders directly to asylums, but this failed to stem the rise in committals to prison, and then subsequent removals to asylums. Between 1890 and 1895 out of a total of 765 convicted lunatics, 334 ended up being converted to pauper lunatics at the end of their sentences.Footnote 151 Many mentally ill prisoners, meanwhile, continued to languish in remand prisons. In the year ending March 1893 some 88 cases of insanity were recorded in Holloway Prison, 72 of whom were remand prisoners and ‘insane before they came in’.Footnote 152 The practice was recognised as a good thing for prisoners and for the public, and difficult to curb, but ‘a very inconvenient thing to the prisons’.Footnote 153
The experience for mentally ill prisoners themselves was doubt about the genuineness of their insanity, delays in transfers and, for many, movements back and forth between prison and asylum.Footnote 154 Prisoners’ own accounts provide valuable, and almost invariably critical, evidence referring to delays in sending insane prisoners to asylums for treatment, and regarded the prison as wholly unsuitable for any form of treatment. These memoirs, for the most part condemning all aspects of prison discipline, highlighted the poor treatment by doctors of insane prisoners rather than instances of good practice, though occasionally prisoners were positive about their medical care and the prison doctors. One Who Has Endured It described the doctor’s visit in Dartmoor as a ‘brutal farce’, while Susan Fletcher commented that the doctor offered friendly and professional care at Westminster Prison and was as good to her as the prison regulations allowed.Footnote 155 Typically the memoirs referred to the inadequate handling of cases of mental breakdown as those afflicted were moved to the punishment cells following displays of violence or infractions of the prison rules, or to the infirmary or padded cell for long periods of observation, pointing out that it was often fellow prisoners rather than the prison medical officers who called attention to cases of insanity. One memoir described the case of a fifteen-year-old boy accused of shamming and found insensible on several occasions. He was treated with blisters to the nape of his neck and a mustard plaster, followed by the stomach pump. Back in his cell, he was found covered in blood, having cut his leg with a broken medicine bottle. He had then eaten the rest of the bottle. Though the doctor confirmed that boy ‘was not in his right mind’, he was kept in the prison hospital until he supposedly recovered.Footnote 156 Another young man described as ‘soft’ was left in a semi-dark cell without anything to employ his mind. After three weeks ‘he took to simply moaning like some dumb beast in mortal agony, and then after another week or so he became perfectly quiet and used to lie day after day stretched on the floor in a half stupefied condition’. He remained in this state for a month until the doctor decided that the boy was insane: ‘the necessary papers were signed, and the unfortunate youth transferred to the county lunatic asylum to live at the expense of the ratepayers for the rest of his life’.Footnote 157 Florence Maybrick recollected how many female prisoners developed symptoms of insanity over many months or years, adding to the ‘ghastliness’ of the prison experience and having a harrowing impact on other inmates:
She is kept in the infirmary with the other patients for three months. If she does not recover her reason within that period, she is certified by three doctors as insane and then removed to the criminal lunatic asylum. In the mean time the peace and rest of the other sick persons in the infirmary are disturbed by her ravings, and their feelings wrought upon by the daily sight of a demented fellow creature.Footnote 158
Examples taken from individual convict and local prisons illuminate the day-to-day negotiations and processes involved in removing prisoners to asylums, which were more complex and less clear cut than the legislation would indicate, involving delays and disputes between prison and asylum officers about the destination of prisoners, or uncertainly concerning their mental state. Catherine Murray, described as a ‘prostitute’, was imprisoned in Mountjoy Prison after she was found guilty of larceny in 1878, following several previous convictions for being drunk and disorderly, and was moved several times between Mountjoy and Dundrum Asylum. During a spell in Mountjoy between March and October 1881 she was reported to be unwell, unfit for strict cellular confinement, badly behaved and violent, showing symptoms of unsoundness of mind and insanity. Murray was removed once again to Dundrum in April 1882.Footnote 159 Convicted of murder and sentenced to penal servitude for life, Denis Flanagan was taken from Kilkenny Prison to Mountjoy in December 1887. Two months later he was transferred to Dundrum after attempting suicide. Kilkenny’s Governor reported that Flanagan had a severe head wound and, though he spoke rationally, ‘from his general conduct and other circumstances I believe him to be suffering from suicidal mania and have no doubt that he will repeat the attempt on his own life at the first opportunity’.Footnote 160 Other removals took longer, though it was unclear in many cases precisely when the prisoner was first suspected of suffering mental disorder. Thomas Kearney, sentenced to five years for wounding, spent eighteen months in Belfast Prison, before being removed to Dundrum; Patrick Sheridan, serving five years for robbery with violence, was moved from Mountjoy to Dundrum over two years after he was committed, having been ‘under observation while mental state worsened’.Footnote 161
In her study of criminal lunacy in Warwickshire, Janet Saunders noted how ‘not only offenders with the less spectacular or obvious mental disorders, but also fairly severely disordered “lunatics” and the obviously mentally deficient were being sent to prison’.Footnote 162 It was then the onset of spectacular or violent behaviour that was likely to prompt transfers of these prisoners, even though this kind of behaviour might be dealt with for lengthy periods before certification was turned to as a last resort.Footnote 163 One man, serving eighteen months for burglary, was sent to the asylum towards the end of his sentence after sixteen months in prison. He had displayed strange behaviour and had been depressed, but it was the onset of excitement and then violence that finally prompted his removal.Footnote 164 One case committed to Mountjoy Prison in 1875 attracted the attention of a Commission into Dundrum’s management, that, among other issues, was investigating the use of inappropriate restraints.Footnote 165 Christina Foster, imprisoned for arson, became insane and was transferred to Dundrum in July of that year, where, after violent outbursts, she was placed in a specially made refractory dress. This subdued her violent outbursts and she was moved back to Mountjoy a year later. In October 1876 she was readmitted to Dundrum, and, after a period of quiet marked by depression, in February 1877 Christina again became violent. She was repeatedly placed in seclusion in the restraining dress, before she was finally removed to Belfast Lunatic Asylum in April 1880, presumably on the expiration of her sentence.Footnote 166
Liverpool Borough Prison has a particularly rich collection of records that, together with local asylum archives, reveal complex histories of conviction, imprisonment and institutional confinement, as well as the importance of locale in a setting shaped by mass migration from Ireland to a port city experiencing in turn prosperity and severe economic downturns and extreme poverty.Footnote 167 Despite the insistence of alienists and advocates of specialised asylum treatment that prisons were inappropriate places for the care and treatment of the insane, these prisoner patients were often unwelcome in asylums, and in the Lancashire asylums the problem was also one of scale. Already in 1854 the Committee of Visitors at Lancaster Asylum despaired at the ‘rapid influx of admissions’, including many vagrant lunatics, via the port of Liverpool, that were filling up Lancashire’s asylums with chronic and incurable cases. They also regretted the lack of a separate asylum for criminal lunatics: ‘the inconvenience and evils of their confinement and association with the ordinary inmates of our Asylums, are still suffered to exist’.Footnote 168 By 1862 Lancaster Asylum held twenty-four criminal patients though the asylum superintendent, John Broadhurst, insisted that only four or five of these were suitable for removal to the criminal lunatic asylum then about to open at Broadmoor.Footnote 169
Irish patients were perceived as a particular problem, associated as they were with violence, drink, vagrancy, disease, prostitution and high levels of crime as they circulated between prisons and lunatic asylums across England and Ireland, accounting for a large proportion of the inmates of English prisons and asylums, especially in port cities and the northern counties. By 1859 around 14 per cent of prisoners in England were Irish-born.Footnote 170 In 1875 it was claimed that 13 per cent of the 446 Irish admissions to Prestwich Asylum were sent from the police courts and gaols of the district.Footnote 171 The large number of Roman Catholic prisoners at Portsmouth’s public works prison prompted Frederick Richard Falkiner, Recorder of Dublin from 1876 to 1905, to conclude they were ‘probably Irishmen’.Footnote 172 In the late 1870s the Wakefield Justices estimated that about 16 per cent of their prisoners were Irish-born, and at least an equal number were English-born of Irish parentage.Footnote 173 Of the 6,707 Roman Catholic prisoners committed to Liverpool Prison in 1868, 53 per cent were born in Ireland. A small number were repatriated, as in 1874 when an Irish male prisoner, sent back from Rainhill Asylum to Liverpool Prison before the expiration of his sentence, was subsequently transferred to Mountjoy Prison in Dublin, but for the most part Irish prisoner patients remained in Lancashire’s asylums and prisons.Footnote 174
Drawing on the minutes of Liverpool Prison’s visiting committee, annual reports and asylum casebooks, the transfers of individuals moving between the prison, Liverpool’s Rainhill Asylum and other local asylums can be traced.Footnote 175 One such individual was Mary Leonard, who was found guilty of burglary at the Liverpool Assizes in December 1868 and sentenced to seven years’ penal servitude. After removal to Millbank Prison in London (presumably to confirm her mental state), she was taken to Broadmoor in 1873, and in 1876 at the expiration of her sentence transferred to Rainhill.Footnote 176 She was noted to be noisy, incoherent and excitable, and had hallucinations of sight and hearing, believing ‘that people enter her room at night and stab her, that poison is put into her food. Says her room is set on fire at night.… Has delusions of an exotic kind and uses obscene language.’ Mary Leonard died in Rainhill almost three years after her admission.Footnote 177 Irishwoman Catherine Nolan’s misdemeanors were noted in the Liverpool prison records in April 1896, when she assaulted a warder and damaged twelve panes of glass. She was handcuffed and put on a no. 1 punishment diet for seven days.Footnote 178 A month later she was admitted to Rainhill Asylum, where she was noted to be dangerous to others and intemperate. ‘She is subject to outbreaks of violence which usually occur at the menstrual period. At times she is violent, destructive, & abusive.’Footnote 179 A year later Catherine Nolan was still described as dangerously excitable, delusional and prone to attack those around her: ‘Cannot be left a moment alone owing to her violence.’ She continued in this state until October 1898, when her death was recorded as a result of tuberculosis of the lungs and intestines.Footnote 180 As the number of admissions to Rainhill increased in the late nineteenth century, its Superintendent, Dr Rogers, despaired at the continual presence of the criminal class ‘as they not only give much trouble and interfere with the discipline, but their presence and intercourse have also an injurious and demoralizing effect on the younger patients’.Footnote 181
Liverpool Prison, as shown in Chapter 3, was notable for its very high proportion of female inmates, many of whom were Irish and likely to be described as turbulent, prone to drunkenness, violent and as prostitutes.Footnote 182 In 1868, 69 per cent of Irish-born prisoners were women.Footnote 183 Frances Holden, a thirty-three-year-old single Irish woman, committed on numerous occasions to Liverpool Prison on charges of prostitution, was transferred to Rainhill in July 1873. She claimed that she had been in prison thirty-three times and that ‘her child was an officer’ there. On admission to the asylum, she was described as suffering from mania and that she was ‘at one time … very excited and at others more depressed’. Her behaviour was described as delusional, volatile and destructive. In October 1876 Holden was removed ‘unimproved’ to Lancaster Asylum.Footnote 184 In the case of both male and female prisoners, it was largely violent and disruptive behaviour – rather than a precise medical diagnosis – that prompted removal from the prison to asylum. It was also the case that many of these prisoners became permanent residents at Rainhill, which created long-term problems in terms of the institution’s management, resources and ability to admit new cases.
As penal policy in England and Ireland shifted away from reforming and redeeming prisoners towards punishing and deterring repeat offenders in the 1860s and 1870s, prison medical officers were even more likely to transfer troublesome and violent prisoners, typically those with protracted prison careers, characterised by recommittals to prison and repeated breaches of prison discipline and punishments. They were also keen to rid themselves of inmates who were diseased and sick, and prisoners suffering general paralysis of the insane (GPI) were particularly liable to removal. Notably difficult patients, they required extra staff and nursing care and had high mortality rates.Footnote 185 These cases were unwelcome in prisons and in asylums, and the movement of prisoners with GPI from Liverpool Gaol to Rainhill and other local asylums reflected what was observed to be a remarkable rise in the disease in Lancashire asylums in the latter decades of the century.Footnote 186 By 1896 most of Rainhill’s deaths were cases of GPI, and in that year eighty-nine men and nineteen women in the asylum were afflicted with the condition.Footnote 187 These included John Murphy, a thirty-five-year-old married Irish labourer, transferred from Liverpool Prison to Rainhill in December 1896. Typifying cases of general paralysis, he was reported to be ‘very noisy and violent and has marked grandiose delusions’, and he remained ‘in a very restless and exalted state’. Murphy died in Rainhill in January 1899.Footnote 188
Catherine O’Brien, a thirty-year-old Irish woman imprisoned for stealing, was described by her husband on her removal to Rainhill in April 1876 as addicted to drink. Her husband also commented that, while his wife was prone to take things, she did not intend to steal them, a likely indication of one of the commonly reported symptoms of GPI, a tendency to hoard other people’s belongings.Footnote 189 Dr Henry Maudsley commented critically in 1875 on six ‘well-marked’ cases of GPI admitted to the West Riding Asylum, ‘after having undergone the whole or the greater part of their punishment in gaol for larceny’, that might easily have been diagnosed at the time of imprisonment ‘by any medical man who had even the most rudimentary knowledge of the symptoms of general paralysis’.Footnote 190 In one case a barrister recognised the disease during the trial, ‘yet this unfortunate man remained in gaol for five months before being sent to the asylum; he underwent the punishment of a criminal for five months after a hopeless disease of the brain had begun to make its fatal progress’.Footnote 191 The prisoner had become violent and excited in prison, was put into a strait jacket and confined in a padded room during the last three weeks of his imprisonment, after which he was sent to the asylum.Footnote 192 While the Lunacy Commissioners expressed concern that such cases were being removed to asylums given the burden they placed on the institutions, they were also frustrated at the lack of care in diagnosing them in the first place.
The frequency with which General Paralytics are convicted of larceny and similar offences, and their mental state unrecognised even after a considerable stay in gaol, and who are brought to the asylum either as criminal lunatic or as ordinary cases, some time after their discharge from gaol, is very discreditable to the administration of the law, and deserves more attention, with a view to remedy, than it has received.Footnote 193
Prison medical officers’ diagnosis of ‘real’ or ‘genuine’ insanity in these and other cases would typically follow prolonged periods of disruptive behaviour by inmates, and the destruction of prison property, suggesting that removal to an asylum was prompted by concerns about management rather than careful judgement, detailed diagnosis or consideration of the prisoners’ best interests, bringing into question the claims of prison medical officers to be making decisions on the basis of their expertise in psychiatry. Prison doctors’ descriptions of such patients at the point of removal refer to prisoners experiencing ‘delusions’, or to the ‘irritability’ or ‘excitability’ that prompted destructive behaviour; they were less likely to come up with a clear diagnosis or to use labels current in psychiatric practice outside of prisons.Footnote 194 This kind of approach magnified the assertions of asylum doctors that prisoners were better off being moved and treated in the asylum by experts in mental disorder, but also confirmed their anxieties about the removal of particularly disruptive patients and their impact on routine and management.
By the late nineteenth century, many asylums in England and Ireland were overcrowded and overstretched, struggling to accept new patients and to effectively maintain regimes of moral management that were based on regularity and order, enhanced diet, work therapy and occupation.Footnote 195 They were reluctant to take in insane criminals who were regarded as troublesome, likely to contribute to high mortality rates and who would be a poor and potentially alarming influence on other patients. In 1887, referring to the practice of reclassifying criminal lunatics as pauper patients at the end of their sentences, the Commissioners in Lunacy described how those removed to county asylums
are a far more dangerous class than those to whom the term is now legally applicable, and if I might devise a name for them, I would call them ‘Lunatic Criminals’; implying that they were ‘criminals’ first and ‘lunatics’ afterwards. It is by this class that murderous assaults are generally committed.Footnote 196
In addition to concerns about the type of illnesses they brought into the institution and the high mortality rates, there was also the risk of escape.Footnote 197 The Superintendent of Somerset County Lunatic Asylum, Dr Charles Medlicott, spoke of the ‘contaminating effect’ of such admissions, arguing that in most cases ‘it is not fair to saddle a criminal who has become insane on our ordinary pauper lunatics’, as ‘the anxiety and responsibility is endless with a class like that, and the restraint that ought to be exercised in their cases is utterly incompatible with the liberty we wish to give to others where we know that there is a possibility of restoration to reason’.Footnote 198
Turf Wars and Claims of Expertise between Prisons and Asylums
Such challenges to the maintenance of order and institutional wellbeing blighted prisons and asylums throughout the second half of the nineteenth century. At the same time both asylum doctors and prison medical officers continued to assert their unique authority and ability to treat mentally ill offenders, though prison doctors’ claims were more likely to be based on ability to recognise, diagnose and manage insanity rather than to treat it. Aside from what appeared to be at times intractable legal and practical issues in reaching decisions on the accommodation of ‘prisoner patients’, in particular instances discussions on where to place the lunatic prisoner evolved into disputes between prison doctors and the prison commissioners and asylum doctors and lunacy commissioners and inspectors. Prison doctors were lambasted in some of these high-profile cases, for their lack of expertise, knowledge and judgement, as well as their resistance to transferring cases, and it was argued that prisoners whose mental and physical condition had worsened in prison would have fared better had they been removed to the specialist care available in the asylum.
Many cases were brought to light where mentally disturbed offenders had languished in prison for lengthy periods, as well as of removals of prisoners to asylums who were described as being in a terrible state of mental and physical health, suffering serious abrasions and other injuries, malnourished and in a filthy condition.Footnote 199 In 1846 – in the midst of the Famine – the report of Ballinasloe District Lunatic Asylum complained of the terrible condition of the ‘poor creatures’ transferred from different prisons in the province, ‘in a most wretched and deplorable state, with broken down constitutions, and labouring under cachectic disease’. In one week alone, three were admitted in a dying state, including a twelve-year-old child, ‘labouring under dementia, epilepsy, and dysentery’. Prisoners were often conveyed in open vehicles, exposed to ‘the inclemency of the weather, as well as the gaze of the populace’, tied down with ropes or even chains.Footnote 200 Prison doctors were still being described in the press in 1867 as not being ‘conversant with mental diseases’, leaving the quiet lunatic to ‘mope in hopeless loneliness’; if turbulent ‘he rages in his cell becoming more incurable every hour’.Footnote 201 The Irish Prison Inspectors continued to detail the appalling state of many such prisoners held in city and county gaols in their annual reports, such as the ‘idiotic’ male prisoner discovered in Kilmainham in December 1875, crouched in a corner of his cell, dirty and ‘howling like a wild beast’. The man, who was declared ‘most unfit for penal treatment in a gaol’, had been sentenced to two months’ hard labour for stealing but was incapable of any work. He had been regularly admitted to Loughlinstown Union Workhouse, ‘and it is to be regretted that he cannot be compelled to remain in it or some other asylum, as the criminal prosecution of someone in his state is not attended with advantage’.Footnote 202 In 1885 a complaint was made by the Office of the Inspector of Lunatic Asylums about a prisoner who had been removed from Castlebar Prison; ‘as to Insane prisoner Wm. [?Connot] having had serious abrasions on wrists when received in Dundrum Asylum’. The Lunacy Inspector was requested in future to bring such complaints to their notice and Dundrum’s medical officer, Dr O’Brien, instructed to deal with the alleged injury.Footnote 203
In many instances, prison officers were accused of causing severe harm or the deaths of insane prisoners, as in a case reported by John Charles Bucknill of an epileptic young man twice imprisoned in the borough gaol owing to his uncontrollable violence. ‘I do not know on what principle he was committed to gaol, instead of at once being sent to an asylum. After thirty months’ residence he died in a fit.’Footnote 204 Nicholas Lawless was committed as a dangerous lunatic to Harold’s Cross Prison, south of Dublin, in 1863, at which point the prison surgeon, Dr Ireland, examined Lawless and pronounced him to be mad.Footnote 205 After a few months, Lawless’s family were informed that he had died. While the cause of death was reported as ‘softening of the brain’, it appeared that Lawless had died as a result of a ‘fearful scalding’ when taking a bath. The Irish Times criticised the prison for withholding evidence and more generally the practice of committing lunatics declared dangerous to prison.
In a jail there is no provision for the curative treatment of the lunatic; he cannot be isolated from the society of criminals, reckless, it may be, and cruel. The warders are jailers, not attendants upon lunatics; the governor is the ruler of a prison, not the experienced superintendent of an asylum for the insane. No supervision, of the constant and careful kind required for the management of a man devoid of reason, can be exercised in a jail. The very structure of a jail building is unfitted for the safe keeping of lunatics.Footnote 206
The case of Catherine Kelly centred less on her handling by prison officers than on the lack of judgement concerning the timing of her removal. In March 1888 Kelly was brought from Tullamore Prison, King’s County to Maryborough District Lunatic Asylum, Queen’s County, where she died four days later. Medical Superintendent Dr Hatchell claimed that she had been moved to the asylum in a dying state and that there were marks and bruises on her body. On this occasion the criticism came from the prison rather than lunacy authorities. At the subsequent inquest, the medical member of the General Prisons Board, Dr George P. O’Farrell, concluded that Kelly died of ‘extreme exhaustion’ and that the prison ‘doctor [Dr James Ridley] showed want of judgement in allowing a woman [in such a weak condition] to be removed 18 miles by road’. While Ridley was not accused of wilful neglect, he was criticised by O’Farrell for failing to transfer Kelly to the asylum immediately on reaching a diagnosis of insanity as ‘a few hours often make the greatest difference between safety & danger in the removal of Lunatics’.Footnote 207
Revelations and debates about these cases took place against the backdrop of a much broader set of concerns about the high death rates of prisoners in England and Ireland; many prisoners received into custody diseased, exhausted or in a state of insanity died shortly after committal. In 1885 the Prison Commissioners alerted Home Secretary Harcourt to the fact that many prisoners were committed to prison in a ‘moribund condition or suffering from serious disease’, suggesting that many cases were dying in prison whose condition would have been detected had they been medically examined at their committal.Footnote 208 Under Secretary to the Home Office Sir Adolphus Liddell observed that the prison was a place of penal discipline and not ‘the proper scene for a Death-bed, and ought not to be converted into a Hospital for Incurables’.Footnote 209 Concerned about the number of prisoners suffering from feeble health or serious illness, Harcourt demanded more rigorous medical examinations in prison and insisted that, once identified, such cases should be moved to a workhouse or infirmary as appropriate.Footnote 210 In fact, deaths in local prisons declined significantly between the 1860s and 1880s, but still included many cases admitted in an exhausted or dying condition alongside large numbers of lunatic prisoners.Footnote 211
In England and Ireland, often extensive official investigations were conducted into the deaths of prisoners, which highlighted disputes between prison and asylum officers concerning the actions that had been taken and causes of death. The case of Ferdinand Parker, alias Shortlander, investigated by the Home Office in 1885, centred on the issue of the timing of his removal to an asylum after he had begun to refuse food.Footnote 212 Parker had been admitted to hospital in Shepton Mallet Prison in May 1885, on account of his weakness after he declined to eat, declaring the food to be poisoned. By this time the prison surgeon concluded that he was too ill to remove. Though his insanity was said to have commenced on 19 May, he was not certified insane until 5 June. On 11 June he was moved to Somerset and Bath Lunatic Asylum. Examined by the asylum medical officer, Parker was declared to be suffering from mania, was very thin and wasted, and his body scratched and abraded, from what were said to be self-inflicted wounds. He died later that evening after two heart attacks, and the inquest concluded that his death was due to a weak heart and prolonged insufficiency of food. The prison doctors explained that they had been reluctant to force-feed Parker because he had a weak heart, and moreover at times he had taken food.Footnote 213 The Commissioners in Lunacy, however, were convinced that he should have been force-fed, adding that
It is the everyday experience of the Commissioners in Lunacy that insane persons who refuse food may be, by proper means, compelled to take sufficient nourishment to keep up their bodily strength till the violence of this phase of insanity has passed.… They see nothing in the circumstance of the present case to have made such a result impossible.Footnote 214
The Medical Inspector of Prisons, Dr Gover, responded that Parker could not have been safely fed by force, stating that the responsible medical officer in charge ‘was the best judge’. ‘To such an argument it would be quite open to Dr Hyatt [the prison doctor] to reply that the prisoner’s heart was not in a condition to bear the strain of forcible feeding, and that but for the attempt made in the asylum he might possibly now be alive.’Footnote 215
Occasionally these cases were more widely publicised, drawing public attention to the failures of the prison system, as in December 1897 when the Manchester Evening News reported a ‘scandal’ at Strangeways Prison involving Edward Cox, an insane prisoner whose ribs had been broken while he was being restrained.Footnote 216 Cox had arrived at Prestwich Asylum with severe injuries, but, while the asylum doctors claimed that eight of his ribs had been broken, the officers at Strangeways asserted that all due care had been exercised by the prison medical officers and that ‘only one or two ribs’ were fractured. The resulting Home Office inquiry revealed that the prisoner had been admitted to Strangeways in April 1897, and the day before his sentence expired on 9 October he became violently insane, assaulting the prison’s senior medical officer, Dr Edwards.Footnote 217 There was a struggle with five prison officers to move Cox to a padded cell, when the injuries occurred. The discovery of the injuries prompted an extensive investigation into the case with allegations that the prison authorities had withheld relevant information on Cox’s mental and physical condition from the Visiting Committee and the certifying magistrate. The Prison Medical Inspector, Dr Smalley, who was asked to examine Cox, criticised the asylum doctors, claiming that they had exaggerated the extent of the injuries. The Chairman of the Prison Visiting Committee, however, insisted that ‘his [Smalley’s] evidence ought not to outweigh the impartial evidence of the Asylum Surgeons who made careful independent assessments’.Footnote 218 It was agreed by all parties that Cox suffered from delusions and was insane. While it was concluded by the Home Office that no unnecessary violence was used against Cox, the prison was criticised for its poor standards of medical care and delays in examining the prisoner.Footnote 219
William Tallack of the Howard Association highlighted the case in a letter to The Times in January 1898, reminding readers there had been a similar occurrence in Strangeways eight years previously, when a prisoner had died of injuries that included a fractured breastbone and a number of broken ribs. That case had never been resolved, and Tallack made a strong argument for full disclosure in the public interest in the case of Cox as ‘a check to the occasional cruelty of warders’ and for the protection of prisoners.Footnote 220
Conclusion
While Dr David Nicolson and a few other individuals served long careers that crossed between prisons and asylums, typically moving from posts as assistant medical officer in an asylum to the prison service, in July 1896 the Journal of Mental Science asserted: ‘Too long have the alienist and the criminologist worked apart.’Footnote 221 Responding to the findings of the Gladstone Report of 1895, it was suggested that this distinction in their spheres of labour was ‘quite unnatural’. Both our prison colleagues ‘and ourselves’ had been remiss, it was concluded, in failing to forge common bases for study and collaboration across institutions of confinement.Footnote 222 Yet a few years later, Dr David Nicolson himself affirmed that ‘Many medical men, including some asylum attendants, who are in every way admirable in their ordinary lunacy work, find themselves not quite at home in the investigation of criminal cases,’ given that the methods of examination were often quite different.Footnote 223
Assertions of expertise – which occasionally flared up in hostile exchanges – took place against the backdrop of prison services still facing the pressures of large numbers of lunatic prisoners. This resulted in part from magistrates’ persistence in directing such cases to prison, though the increase was also likely to have resulted from prison medical officers’ growing willingness to record prisoners as mentally disordered or unfit. Medical Inspector Dr Robert Gover explained how ‘In former times I have no doubt that many prisoners who were insane were dealt with as if they were sane more than now,’ with prison medical officers more willing to send insane prisoners on to the asylum in their own interests.Footnote 224 In 1893 Gover noted that the number of lunatics proportional to the prison population was larger than any year on record, with eighty-one admissions to local prisons during the year.Footnote 225 These ranged from prisoners on very short sentences to those sentenced to ten years’ penal servitude, who were recognised to be insane at or shortly after their reception in prison. Most were quickly certified as insane and moved to asylums. ‘All were unfit for prison discipline, and many must have been unable to understand why they were placed upon their trial, or the meaning of any of the legal proceedings taken. The insanity was very obvious in most cases.’Footnote 226 The Commissioners’ Reports also revealed the persistent messiness of dealing with such cases. Of the eleven cases reported in Liverpool Prison in 1893, three were removed to Rainhill Asylum, one to Whittingham Asylum, one was discharged into the care of friends and the rest taken to local workhouses.Footnote 227
The continued admission of the mentally disordered into prisons took place at a time where there was mounting concern about both the high numbers of criminal lunatics more broadly and the rise in lunacy in the population as a whole in England and even more so in Ireland.Footnote 228 While the alarming rise in the asylum population of Ireland was widely commented on, the Irish General Prisons Board still referred in 1892 to the ‘objectionable and illegal practice prevailing throughout the country, of committing lunatics to gaol, instead of sending them directly to asylums’.Footnote 229 A year later the number of asylum transfers had increased to 92: of these, 72 had been found insane on reception, five were imbecile or weak-minded and three ‘doubtful’.Footnote 230 Limerick alone had transferred thirteen male prisoners and six female to asylums, most of whom were insane when committed. Many such prisoners were suffering from dementia or described as imbeciles, and had been imprisoned with short sentences for begging or vagrancy.Footnote 231
Despite the claims of prison doctors, expertise in psychiatry in the context of criminal justice was still often equated with psychiatrists working outside of prisons. In Ireland it was largely lunacy inspectors and asylum superintendents, including Dr Conolly Norman, Medical Superintendent of Richmond Asylum and Dr Moloney of Swift’s Hospital (St Patrick’s), who were responsible for examining prisoners suspected of being mentally ill. In 1886 the Lunacy Commissioners, as requested by the Secretary of State, compiled a list of persons residing near each English prison who were fitted for the role of examining persons charged with capital offences reported to be of unsound mind or in whose case the defence of insanity was likely to be advanced. The list was largely composed of asylum superintendents. Dr Orange and Dr Gover had been relieved of their duties in this regard, Orange owing to his poor health, Gover because he was over-committed; Du Cane also argued that Gover’s appointment was incompatible with his role as Medical Inspector of Prisons. Dr Henry Bastian, formerly an Assistant Superintendent at Broadmoor, was appointed to deal with cases in the metropolitan area, with a list of reserves including two eminent psychiatrists, Dr George Fielding Blandford and Dr Henry Maudsley, along with Dr Edgar Sheppard, retired Medical Superintendent of Colney Hatch Asylum, for a hefty fee of five guineas for a day’s examination or for providing evidence.Footnote 232
By the late nineteenth century many asylum doctors and some doctors working in the prison service itself argued that prison medical officers needed to be exposed to a period of training in lunacy outside of the prison, in order to deal with those prisoners who required special care. While such views, which were also strongly voiced in evidence given to the Gladstone Committee in 1895, can be construed as pointing to the continuing inadequacy of prison medical officers in dealing with mental disorder, they could also represent recognition of the reality of their roles and ambition to have their increasing experience and knowledge of the field enhanced and given more authority. ‘That candidates for medical appointments should be required to show that they have given special attention to lunacy’ also indicated that their heavy workload in this area of practice was being acknowledged.Footnote 233 The Medical Superintendent of Wakefield Asylum recommended that prison medical officers should spend six months attached to a large county asylum, as ‘the difficulties of diagnosis are very great’. He also argued that the number of medical officers should be doubled in London’s receiving prisons, given the huge workload that often necessitated (over)rapid diagnosis.Footnote 234 By the 1890s, David Nicolson was advocating asylum training and secondments for prison medical officers, at the same time suggesting that while prison doctors could enhance their skill sets, asylum doctors might be uncomfortable with criminal cases.Footnote 235 Nicolson went on to chair a committee of inquiry in Ireland in 1905 examining the issue of ‘borderland’ cases transferred between prisons and asylums, and it was recommended that candidates for appointment as medical officer in convict prisons be required to produce testimony of special experience among the insane in asylums.Footnote 236
During the latter part of the nineteenth century there was growing concern that while ‘sane criminals’ were finding their way into the criminal lunatic asylums of Broadmoor and Dundrum, as well as other asylums, the sanity of many of those imprisoned for their crimes was also being called into question. The Gladstone Report concluded with a memorandum ‘Insanity in Prisons’ that, while denying that the prison system produced mental breakdown, concluded that the number of cases of insanity had greatly increased since the prison system had been centralised twenty years previously. The Medical Inspector of the Prisons Board claimed that the practice of sending insane persons to prison contributed to this increase, while the Commissioners in Lunacy argued that many individuals were only dealt with as lunatics after they had committed an offence and thus found their way into prison, while more cases of insanity were actually being identified in prison.Footnote 237 Prison administrators and prison doctors were increasingly reproached for their failure ‘to realise how slender and impalpable is the border-line between crime and insanity … the proper inmates of an asylum are too frequently treated with the penal discipline of a prison’.Footnote 238 The Report, however, at a point where medical men – working in prison and outside of it – were gaining in professional authority and experience in dealing with criminal offenders, finally opened up the possibility of cooperation between the asylum and prison, ‘which cannot but make for a better understanding of the sources and relationships of crime and insanity’.Footnote 239



 Open access
Open access