


The Mediterranean diet has consistently been demonstrated to have a beneficial influence on health and longevity( Reference Martinez-Gonzalez, Bes-Rastrollo and Serra-Majem 1 – Reference Sofi, Abbate and Gensini 3 ). Two meta-analyses conducted by our group in 2008 and in 2010 clearly showed a significant protection for greater adherence to the Mediterranean diet on mortality and morbidity from several causes( Reference Sofi, Cesari and Abbate 2 , Reference Sofi, Abbate and Gensini 3 ). However, since the publication of the earliest meta-analysis further studies have been published, making an update of the literature necessary. In addition, despite the vast amount of literature available, one main issue remains yet to be solved: how can we define one's adherence to the Mediterranean diet?
Over the past years, several attempts for estimating adherence to the Mediterranean diet have been done, mainly through the creation of diet quality indices( Reference Bach, Serra-Majem and Carrasco 4 , Reference Kourlaba and Panagiotakos 5 ). The usefulness of these measures, the most common of which is certainly the Mediterranean dietary score created by Trichopoulou et al.( Reference Trichopoulou, Costacou and Bamia 6 ), has been assessed in several longitudinal studies in association with different health outcomes( Reference Sofi, Abbate and Gensini 3 ). Although significant associations between such scores and mortality have been found in different populations, the clinical application of such scores is not easy to obtain since studies evaluating different cohorts with different dietary behaviours present different cut-off values for consumption of food groups and the quantification of each food component is not always available. To the best of our knowledge, no studies have been conducted that attempt to review and analyse altogether the studies investigating the Mediterranean diet score in relation to health outcomes, with the aim of proposing an adherence score that could be used not only as an epidemiological tool but also at an individual level.
Hence, the aims of the present study were to: (i) perform an updated systematic review and meta-analysis on studies investigating adherence score to the Mediterranean diet and health status, due to the high number of studies that have been published since the release of the earliest meta-analysis; and (ii) obtain from all of the available cohort studies the cut-off value for consumption of each food group, in order to propose a questionnaire for estimation of adherence to the Mediterranean diet based on descriptive data of the literature.
Methods
Updated systematic review
The databases MEDLINE (source: PubMed, 1966 to June 2013), Embase (1980 to June 2013), Web of Science, The Cochrane Library (source: The Cochrane Database of Systematic Review, 2013, issue 6), Clinicaltrials.org and Google Scholar were systematically reviewed and updated using a literature search strategy. Relevant keywords relating to the Mediterranean diet in combination as MeSH (Medical Subject Headings) terms and text words (‘Mediterranean diet’, or ‘diet’ or ‘dietary pattern’ ‘Mediterranean’, or ‘adherence’ or ‘score’ and their variants) were used in combination with words relating to health status (‘health’, or ‘mortality’ or ‘morbidity’, or ‘cardiovascular diseases’, or ‘neoplastic diseases’, or ‘cancer’, or ‘neoplasm’, or ‘degenerative diseases’, or ‘Alzheimer's disease’, or ‘Parkinson's disease’, or ‘cerebrovascular disease’, or ‘stroke’, or ‘outcome’, or ‘prospective’, or ‘follow-up’, or ‘cohort’ and their variants). The search strategy had no language restrictions and was supplemented by manually reviewing the reference list of all retrieved articles.
Two investigators (F.S., A.C.) assessed potentially relevant articles for eligibility. The decision to include or exclude studies was hierarchical and initially made on the basis of the study title, then of the study abstract and finally of the complete study manuscript. We included studies that assessed in a prospective way the possible association between a Mediterranean dietary score and health outcomes, as already reported in the previous meta-analyses( Reference Sofi, Cesari and Abbate 2 , Reference Sofi, Abbate and Gensini 3 ). Two researchers independently completed searches, study identification, data abstraction and tabulation, and discordances were resolved by discussion. Outcomes of interests were overall mortality, mortality from and/or incidence of cardio- and cerebrovascular diseases, mortality from and/or incidence of cancer, as well as incidence of neurodegenerative diseases.
Literature-based adherence score to the Mediterranean diet
All cohort studies that investigated the association between adherence to the Mediterranean diet and health outcomes were collected. We summarize all the amounts chosen as cut-offs for determining adherence to the Mediterranean diet, together with the author, year of publication, cohort analysed, country of the cohort, number of subjects investigated and the age of subjects, according to sex, in Tables 1 and 2.
Table 1 Values of components of adherence score to the Mediterranean diet among men (g/d)

SENECA, Survey in Europe on Nutrition and the Elderly: a Concerted Action; FINE, Finland, Italy, the Netherlands, Elderly study; EPIC, European Prospective Investigation into Cancer and Nutrition; WHICAP, Washington Heights-Inwood Columbia Aging Project; ULSAM, Uppsala Longitudinal Study of Adult Men; SUN, Seguimiento Universidad de Navarra; GGPSG, Gerontological and Geriatric Population Studies in Gothenburg; EPICOR Study, Italian Section of the European Prospective Investigation into Cancer and Nutrition; NLCS, Netherlands Cohort Study; NOMAS, Northern Manhattan Study; VIP, Västerbotten Intervention Program; G, Greece; A, Australia; S, Spain; B, Belgium; D, Denmark; F, France; H, Hungary; I, Italy; N, The Netherlands; P, Portugal; Sw, Switzerland; Swe, Sweden; Ge, Germany; No, Norway; OM, overall mortality; Al, Alzheimer's disease; C, cancer; St, stroke; CBVD, cerebrovascular disease; n.d., not determined.
*Mean values.
Table 2 Values of components of adherence score to the Mediterranean diet among women (g/d)
SENECA, Survey in Europe on Nutrition and the Elderly: a Concerted Action; EPIC, European Prospective Investigation into Cancer and Nutrition; SWLHC, Scandinavian Women's Lifestyle and Health Cohort; WHICAP, Washington Heights-Inwood Columbia Aging Project; SUN, Seguimiento Universidad de Navarra; GGPSG, Gerontological and Geriatric Population Studies in Gothenburg; EPICOR Study, Italian Section of the European Prospective Investigation into Cancer and Nutrition; NLCS, Netherlands Cohort Study; NOMAS, Northern Manhattan Study; VIP, Västerbotten Intervention Program; G, Greece; A, Australia; S, Spain; B, Belgium; D, Denmark; F, France; H, Hungary; I, Italy; N, The Netherlands; P, Portugal; Sw, Switzerland; Swe, Sweden; Ge, Germany; No, Norway; OM, overall mortality; Al, Alzheimer's disease; C, cancer; St, stroke; CBVD, cerebrovascular disease; n.d., not determined.
*Mean values.
Due to the wide distribution of median consumption of some food groups in the included studies (e.g. see legumes, whose consumption ranges from 2 to 75 g/d), data were logarithmically transformed and back-transformed for data presentation. Median (or mean) values for consumption of food groups composing the Mediterranean diet adherence score were weighted for the number of subjects enrolled in each study. This was because of the large variability in terms of subjects analysed and because the sample size of the study was found to be the most significant contributor to the robustness of results in our previous meta-analysis( Reference Sofi, Abbate and Gensini 3 ). After that, we calculated the mean value of all of the weighted medians and the 2 sd for each food group. In order to provide meaningful estimates for clinical practice we finally rounded the resulting numbers close to the 2 sd values for each measure, by obtaining three categories of consumption for each food group.
Statistical analysis
We used RevMan version 5·0·18 for Macintosh and IBM SPSS Statistics version 18·0 for Macintosh to pool and analyse results from the individual studies. The methods and results of all the recent identified cohort prospective studies were added to the previous table and data were formally combined( Reference Sofi, Abbate and Gensini 3 ). Pooled results are reported as relative risk (RR) and are presented with 95 % confidence interval with two-sided P values using a random-effects model (DerSimonian and Laird method) and the general variance-based method. A P value less than 0·05 was considered statistically significant. We used, when available, the results of the original studies from multivariate models with the most complete adjustment for potential confounders; the confounding variables included in this analysis are shown in Table 3.
Table 3 Study characteristics of the recent prospective studies investigating adherence to the Mediterranean diet and health outcomes

ULSAM, Uppsala Longitudinal Study of Adult Men; GGPSG, Gerontological and Geriatric Population Studies in Gothenburg; EPICOR Study, Italian Section of the European Prospective Investigation into Cancer and Nutrition; EPIC, European Prospective Investigation into Cancer and Nutrition; NLCS, Netherlands Cohort Study; NOMAS, Northern Manhattan Study; BDNS, British Diet and Nutrition Survey; SUN, Seguimiento Universidad de Navarra; VIP, Västerbotten Intervention Program; SWLHC, Swedish Women's Lifestyle and Health Cohort; NIH-AARP, National Institutes of Health-AARP Diet and Health Study; Swe, Sweden; I, Italy; S, Spain; N, The Netherlands; D, Denmark; F, France; Ge, Germany; G, Greece; No, Norway; OM, overall mortality; St, stroke; C, cancer; CBVD, cerebrovascular disease; M, males, F, females; EI, energy intake; MetS, metabolic syndrome; BP, blood pressure; WC, waist circumference; CRP, C-reactive protein; PA, physical activity; HRT, hormone replacement therapy; TV, television; PSA, prostate-specific antigen.
*Mean values.
Statistical heterogeneity was evaluated using the I 2 statistic, which assesses the appropriateness of pooling the individual study results. The I 2 value provides an estimate of the amount of variance across studies due to the heterogeneity rather than chance. Where I 2 was greater than 50 %, heterogeneity was considered substantial. Small study bias and/or publication bias was appraised by visual inspection of a funnel plot of effect size v. standard error and, analytically, by Egger's test.
Results
Updated systematic review and meta-analysis
The updated search from recent years resulted in the identification of eighteen additional prospective studies published up to June 2013( Reference Sjorgen, Becker and Warensjo 7 – Reference Bosire, Stampfer and Subar 24 ). Characteristics of these recent studies are displayed in Table 3. Of these, seven cohorts presented overall mortality as clinical outcome( Reference Sjorgen, Becker and Warensjo 7 , Reference Tognon, Rothenberg and Eiben 8 , Reference Buckland, Agudo and Travier 10 , Reference van den Brandt 11 , Reference McNaughton, Bates and Mishra 14 – Reference Tognon, Nilsson and Lissner 16 ), eight incidence and/or mortality from cardio- and cerebrovascular diseases( Reference Sjorgen, Becker and Warensjo 7 , Reference Agnoli, Krogh and Grioni 9 , Reference Buckland, Agudo and Travier 10 , Reference Gardener, Wright and Gu 12 , Reference Tognon, Nilsson and Lissner 16 – Reference Misirli, Benetou and Lagiou 19 ), and eight incidence and/or mortality from neoplastic diseases( Reference Buckland, Agudo and Travier 10 , Reference Couto, Boffetta and Lagiou 13 , Reference Tognon, Nilsson and Lissner 16 , Reference Bamia, Lagiou and Buckland 20 – Reference Bosire, Stampfer and Subar 24 ). No updated studies for the incidence of neurodegenerative diseases have been found. On the other hand, one study resulted to be an updated analysis of a study already reported in the previous meta-analyses for the overall mortality outcome, so only the most updated study was added to this updated final analysis( Reference Couto, Boffetta and Lagiou 13 ). Altogether with the studies previously investigated, a total of thirty-five cohort prospective studies were included and entered into the final analysis. This updated analysis determined an increase of the study population up to a total of 4 172 412 subjects analysed.
Meta-analytic pooling under a random-effects model showed the already reported significant association between 2-point increased adherence to the Mediterranean diet and reduced risk of mortality from all causes (RR = 0·92; 95 % CI 0·91, 0·93; P < 0·00001; Fig. 1), with little evidence of statistical heterogeneity across the studies (I 2 = 47 %; P = 0·01). This heterogeneity seems to be determined mainly by the study of van den Brandt( Reference van den Brandt 11 ). After exclusion of this latter study, the statistical heterogeneity disappeared (I 2 = 35 %; P = 0·08), with no modification of the association between adherence to the Mediterranean diet and overall mortality (RR = 0·92; 95 % CI 0·91, 0·93; P < 0·00001).
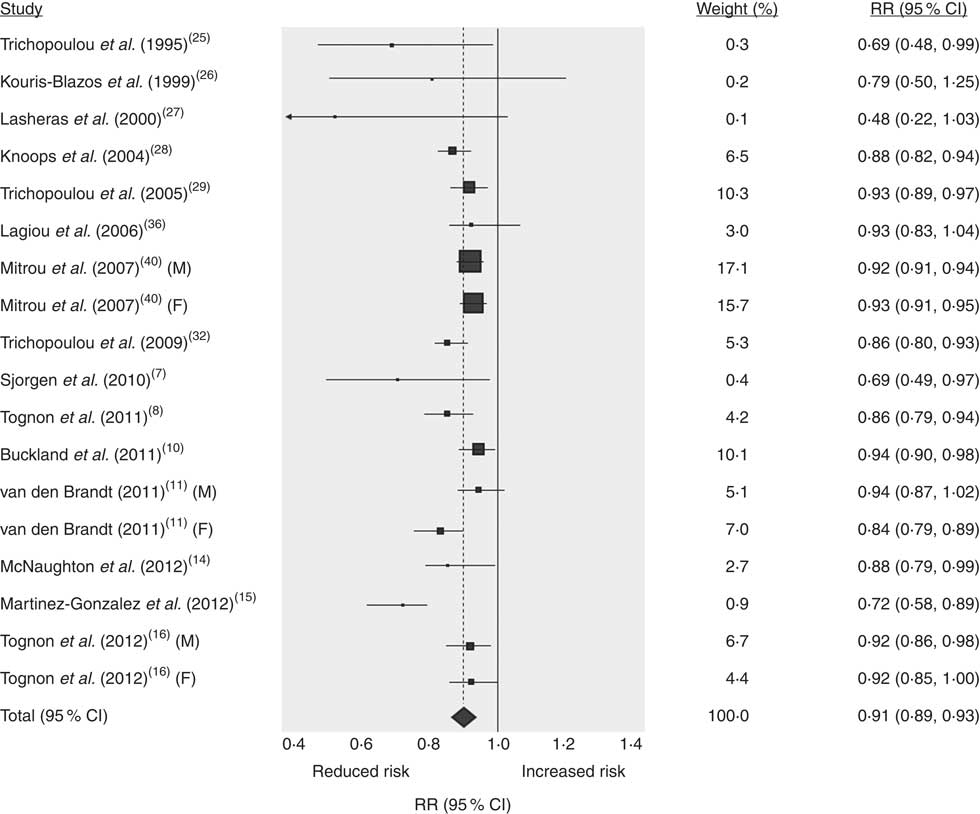
Fig. 1 Forest plot for updated meta-analysis on greater adherence score to the Mediterranean diet (2-point increase) and overall mortality risk. Plotted are the relative risk (RR; represented by ▪, with the symbol size proportional to the weight in meta-analysis) and the 95 % confidence interval (represented by horizontal bars), with the summary measure (represented by - - - - - and ⧫, with the associated 95 % confidence interval indicated by the symbol width) and the line of no effect (——)
Moreover, we found that a 2-point increase of adherence to the Mediterranean diet still remained associated with a reduced risk of mortality from and incidence of CVD (RR = 0·90; 95 % CI 0·87, 0·92; P < 0·00001; Fig. 2), showing no significant heterogeneity across the studies (I 2 = 38 %; P = 0·07). Likewise, among studies investigating mortality and incidence of neoplastic diseases (Fig. 3), a greater adherence to the Mediterranean diet still determined a significant protection, to a similar extent as the previous meta-analysis (RR = 0·96; 95 % CI 0·95, 0·97; P < 0·00001), with evidence of significant heterogeneity across the studies (I 2 = 65 %; P < 0·0 0 1). The heterogeneity seems to be determined by the recent studies investigating breast and colorectal cancer( Reference Buckland, Travier and Cottet 21 – Reference Agnoli, Grioni and Sieri 23 ). After exclusion of these three studies, the statistical heterogeneity disappeared (I 2 = 36 %; P = 0·10), with no modification on the protection of the Mediterranean diet v. neoplastic disease (RR = 0·96; 95 % CI 0·95, 0·97; P < 0·00001).

Fig. 2 Forest plot for updated meta-analysis on greater adherence score to the Mediterranean diet (2-point increase) and cardiovascular incidence and/or mortality risk. Plotted are the relative risk (RR; represented by ▪, with the symbol size proportional to the weight in meta-analysis) and the 95 % confidence interval (represented by horizontal bars), with the summary measure (represented by - - - - - and ⧫, with the associated 95 % confidence interval indicated by the symbol width) and the line of no effect (——)

Fig. 3 Forest plot for updated meta-analysis on greater adherence score to the Mediterranean diet (2-point increase) and cancer incidence and/or mortality risk. Plotted are the relative risk (RR; represented by ▪, with the symbol size proportional to the weight in meta-analysis) and the 95 % confidence interval (represented by horizontal bars), with the summary measure (represented by - - - - - and ⧫, with the associated 95 % confidence interval indicated by the symbol width) and the line of no effect (——)
Literature-based adherence score to the Mediterranean diet
Characteristics of the studies included for this analysis are reported in Tables 1 and 2 for men and women, respectively. For the purpose of this analysis some studies previously included in the updated meta-analytic analysis were excluded, due to the lack of information on amount of consumption for the different food groups composing the adherence score.
We were able to collect data from twenty-four cohort studies for men( Reference Sjorgen, Becker and Warensjo 7 – Reference Couto, Boffetta and Lagiou 13 , Reference Martinez-Gonzalez, Guillen-Grima and De Irala 15 – Reference Bamia, Lagiou and Buckland 20 , Reference Trichopoulou, Kouris-Blazos and Wahlqvist 25 – Reference Martinez-Gonzalez, Garcia-Lopez and Bes-Rastrollo 35 ) and twenty-six for women( Reference Tognon, Rothenberg and Eiben 8 – Reference Couto, Boffetta and Lagiou 13 , Reference Martinez-Gonzalez, Guillen-Grima and De Irala 15 – Reference Couto, Sandin and Lof 22 , Reference Trichopoulou, Kouris-Blazos and Wahlqvist 25 – Reference Lagiou, Trichopoulos and Sandin 36 ). It is interesting to note that values of consumption for food groups composing adherence score to the Mediterranean diet resulted to be, in some cases, different across the studies. For instance, between two cohorts of subjects coming from the same continent (e.g. Spain and Greece) the median consumption of some food groups varied from 90 to 187 g/d (e.g. cereals for men between Martinez-Gonzalez et al.( Reference Martinez-Gonzalez, Garcia-Lopez and Bes-Rastrollo 35 ) and Buckland et al.( Reference Buckland, Agudo and Travier 10 )). More interestingly, vegetable consumption showed a wide variability even between two cohorts of subjects coming from the same country (e.g. vegetables: 75 g/d v. 239 g/d for Sjorgen et al.( Reference Sjorgen, Becker and Warensjo 7 ) and Tognon et al.( Reference Tognon, Rothenberg and Eiben 8 ), respectively).
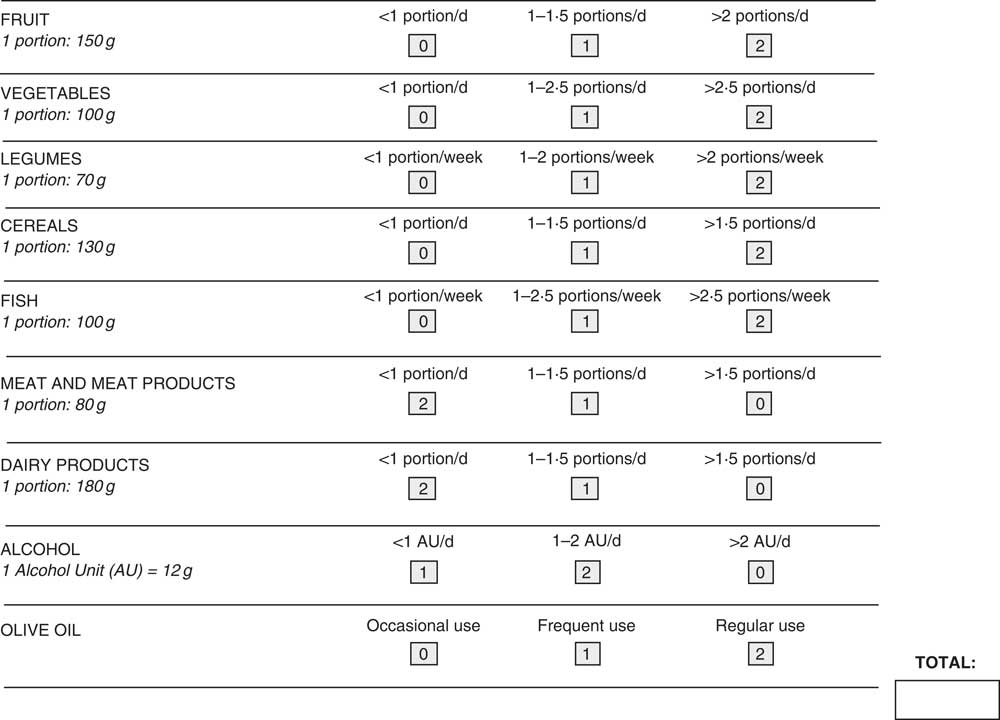
We utilized such data for proposing an adherence score based on literature data. To this aim, we weighted all the median (or mean) values for the sample size of each study population and then we calculated the mean value of all the weighted medians. Hence, we calculated the 2 sd value and we rounded the number close to the ±2 sd, determining three different categories of consumption for each food group (e.g. for cereals: weighted mean = 162·7 (sd 34·6) g/d that determined three different categories <130 g; 131–200 g; >200 g). For food groups typical of the Mediterranean diet (fruit, vegetables, cereals, legumes and fish) we gave 2 points to the highest category of consumption, 1 point for the middle category and 0 point for the lowest category. Conversely, for food groups not typical of the Mediterranean diet (meat and meat products, dairy products) we gave 2 points for the lowest category, 1 point for the middle category and 0 point for the highest category of consumption. For alcohol, we used the categories related to the alcohol unit (1 alcohol unit = 12 g of alcohol), by giving 2 points to the middle category (1–2 alcohol units/d), 1 point to the lowest category (<1 alcohol unit/d) and 0 point to the highest category of consumption (>2 alcohol units/d). Finally, we introduced olive oil as part of the proposed score due to its importance in the typical Mediterranean diet and the beneficial effect of its consumption on health and longevity (2 points = regular use; 1 point = frequent use; 0 point = occasional use). The final adherence score comprised nine food categories with a score ranging from 0 point (lowest adherence) to 18 points (highest adherence). Since no relevant differences for proposed food categories across men and women were obtained, a single score was computed for both sexes (Fig. 4).
Discussion
In the present study we conducted an updated meta-analysis on the association between adherence to the Mediterranean diet and health outcomes, with the additional purpose of proposing an adherence score, based on data from the literature, that can be used also at an individual level and not only in an epidemiological setting.
Greater adherence to the Mediterranean diet has long been reported to be protective against the occurrence of chronic degenerative disease( Reference Martinez-Gonzalez, Bes-Rastrollo and Serra-Majem 1 ). Two previous meta-analyses conducted by our group reported the Mediterranean diet to be the optimal diet for preserving a good health status( Reference Sofi, Cesari and Abbate 2 , Reference Sofi, Abbate and Gensini 3 ). Moreover, recently, the protective role of the Mediterranean diet has been also demonstrated in a dietary intervention study conducted in Spanish middle-aged subjects. Over a follow-up period of 4·8 years, subjects following the Mediterranean diet reported to have a protection of 30 % v. the occurrence of CVD in a primary prevention setting( Reference Estruch, Ros and Salas-Salvadó 37 ).
We decided to update the meta-analysis previously published by our group because many studies have been released in the last 3 years. This updated analysis was conducted with the same methods used for the previous meta-analysis( Reference Sofi, Abbate and Gensini 3 ) and allowed us to add eighteen prospective studies to the final analysis( Reference Sjorgen, Becker and Warensjo 7 – Reference Bosire, Stampfer and Subar 24 ). Hence, we were able to extend the evidence to an overall study population of more than 4 000 000 subjects and to other countries such as Italy and Scandinavian countries( Reference Sjorgen, Becker and Warensjo 7 – Reference Agnoli, Krogh and Grioni 9 , Reference Tognon, Nilsson and Lissner 16 , Reference Couto, Sandin and Lof 22 , Reference Agnoli, Grioni and Sieri 23 ). From this updated analysis we could report that a 2-point increase in adherence score to the Mediterranean diet is actually protective v. the occurrence of overall mortality, incidence and/or mortality from cardiovascular and neoplastic causes, with again similar results compared with the previous analyses (−8 % for overall mortality, −10 % for CVD and −4 % for cancer).
An additional purpose of the present article was to obtain, from the most updated prospective cohort studies, data regarding the amount of consumption for food groups composing the adherence score to the Mediterranean diet in order to propose a literature-based adherence score that can be used to assess adherence to the Mediterranean diet also at an individual level.
Over the last years, research on nutritional science and on its relationship with disease has shifted from the study of single nutrients to the evaluation of food patterns, since subjects do not eat isolated nutrients and because the complex interactions among different nutrients have been reported to be extremely relevant for the healthy aspects of diet. Some attempts for estimating the adherence to the whole diet, and particularly to the Mediterranean diet, have been conducted( Reference Bach, Serra-Majem and Carrasco 4 , Reference Kourlaba and Panagiotakos 5 ). The first and most widely used tool to assess adherence to the Mediterranean diet, created by Trichopoulou et al.( Reference Trichopoulou, Costacou and Bamia 6 ), has been extremely widely used for epidemiological research and is based on the sex-based median amount of consumption of food groups that are characteristic of the traditional Mediterranean diet in the sample investigated. On one hand, this score has many advantages because it helped to introduce the concept of an adherence score to a specific diet and allowed to estimate the association between the adherence score and risk of disease in an epidemiological setting. On the other hand, however, it has the main disadvantage of being widely related to the availability of data coming from a sample population, differing substantially from one cohort to another, even within the same country, and more importantly because it does not give an amount of consumption for food groups composing the score that can be used in everyday clinical practice, at an individual level. This is the reason why other indices have been created. One example is that of Panagiotakos et al.( Reference Panagiotakos, Pitsavos and Arvaniti 38 ) who created a simple questionnaire based on recommendations of the guidelines for a healthy diet and characterized by a few questions used for estimating the frequency of consumption (monthly or daily) of food groups more or less characteristic of the Mediterranean diet. Another example is the questionnaire developed in the PREDIMED study and recently assessed in the SUN (Seguimiento Universidad de Navarra) cohort( Reference Dominguez, Bes-Rastrollo and de la Fuente-Arrillaga 39 ). Both these questionnaires have the advantage of being feasible for assessing adherence to the Mediterranean diet at an individual level but they are not based on data from the literature.
That is why we decided to utilize all the available data coming from the most relevant cohort studies for proposing a new evidence-based score for assessing adherence to the Mediterranean diet.
The approach we used, despite able to obtain all the literature data available in this context, may present some limitations. Different cohorts coming from the same country reported to have different cut-offs of consumption for the adherence to the Mediterranean diet, and even among the same countries the range of consumption within the same food group varied. Moreover, by analysing data it became apparent that the median of consumption was extremely related to the sample size of the population investigated. To date, smaller cohorts had, at the same time, higher consumption and vice versa. Hence, we decided to calculate the mean value of all the food groups by taking into account the sample size of the population, i.e. estimating the weighted medians for consumption of all of the food groups.
Despite all these efforts, some limitations that are intrinsic to the single studies still remain. One of these is the lack of uniformity in data regarding the same food group. Some studies report potatoes together with vegetables, while others include them as a single food group, whereas some others include legumes with nuts and not by themselves, and so on.
Nevertheless, the strength of this proposed adherence score is that food group data come from the most updated and comprehensive review of the literature in this context. If confirmed and validated in other studies, the evidence-based search strategy used for obtaining data from the available studies will hopefully help the transferability of such an adherence score into clinical practice.
Conclusion
We updated the results of our previous meta-analyses by including eighteen cohort prospective studies published in the last 3 years and we were able to show the beneficial effects of a greater adherence to the Mediterranean diet in terms of protection v. overall mortality and occurrence of the most important chronic diseases. In addition, by using data coming from the systematic review we proposed an adherence score based on literature data that can be also feasible for assessment of the adherence to the Mediterranean diet at an individual level.
Acknowledgements
Sources of funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. Conflicts of interest: No conflicts of interest to declare. Ethics: Ethical approval was not required. Authors’ contributions: conception and design: F.S. and G.F.G.; analysis and interpretation of the data: F.S., C.M. and A.C.; drafting of the article: F.S. and R.A.; critical revision of the article for important intellectual content: A.C., C.M., R.A. and G.F.G.; final approval of the article: F.S. A.C., R.A. and G.F.G.; statistical expertise: F.S.







