Generalized anxiety disorder (GAD) and Obsessive compulsive disorder (OCD) are common psychiatric disorders. Researchers studying the pathophysiology of these two disorders evaluated the effect of metacognition. However, there is no research examining the metacognition differences of these two psychiatric conditions.
This study was performed to compare the metacognitions in OCD, GAD and healthy controls.
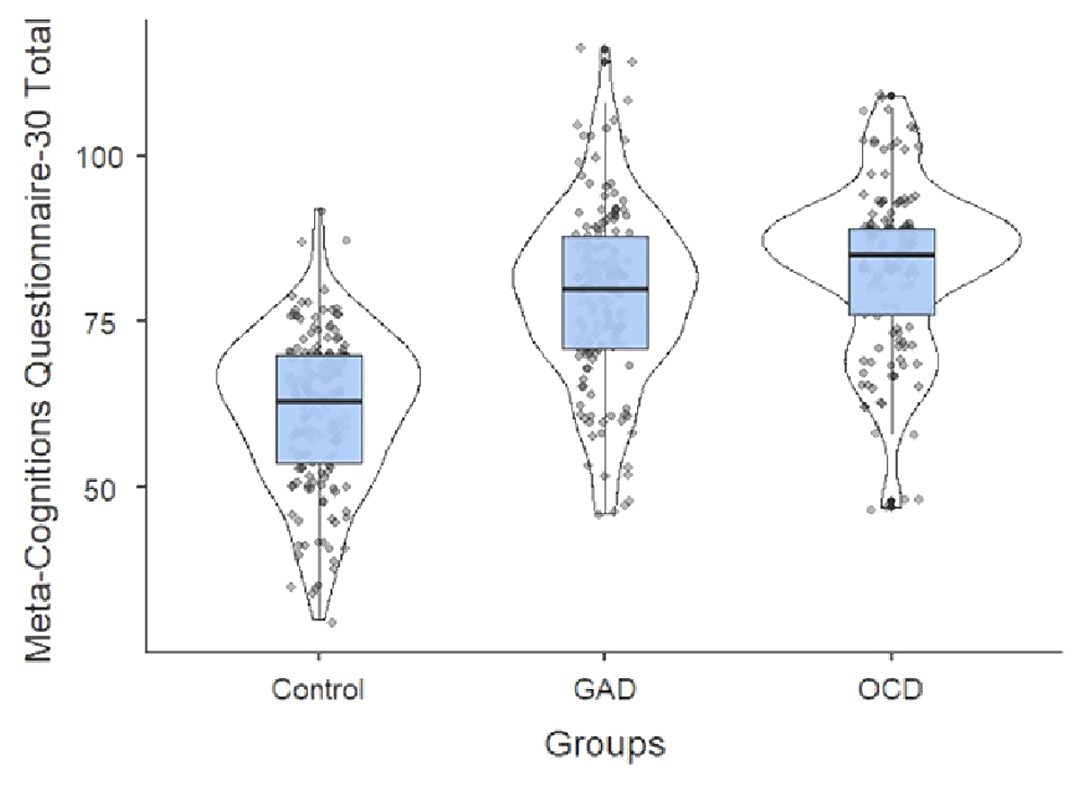
The sample of this study consisted of 158 GAD and 137 OCD patients aged 18-65 years who presented to outpatient psychiatry clinic and applied to the health committee 168 healthy controls without psychopathology. Sociodemographic data form, Meta-Cognitions Questionnaire-30 scale(MCQ-30), Beck Depression Inventory(BDI) and Beck Anxiety Inventory(BAI) were applied to the volunteer participants who met the criteria for participation in the study. The data obtained were evaluated statistically and subjected to statistical analysis.
The mean age was 31.89 ± 10.86 years and was 60.5% (n = 208) women. There was statistical difference between marital status, occupation and income(p <0.05). In addition, there was a statistically significant difference between MCQ-30 total and subscales, BDI and BAI (p <0.001). According to the comparison of OCD and GAD patients, ’positive belief’, MCQ-30 total and BAI scores were found to be statistically different (p <0.05), ’Uncontrollability and danger’, ’Cognitive Confidence’, ’Beliefs about The Need to Control Thoughts’, ’Cognitive Self-Consciousness’, BDI there was no statistical difference between them (p> 0.05).
Our results are contributing to the understanding of the uncertainty of development and maintenance of OCD and GAD. Additionally, metacognitions could be important for the diagnosis and treatment of OCD and GAD.
No significant relationships.
In pandemic conditions, obsessive rituals such as hygiene can be considered adaptive together with the extreme measures that must be followed to avoid contagion by Covid-19, we suggest that the stress the pandemic has caused may result in an increase in the percentage of OCD symptom and severity in the Chilean population at Santiago.
Study OCD symptoms and their severity during a contamination pandemic such as COVID and quarentine, and compare them to national reports of OCD prevalence in Chile. We hypothesize that OCD symptoms would be higher in these stressfull situations.
An online voluntary and annonymous survey was carried out asking about sociodemographic variables and the Y-BOCKS scale, an OCD symptom severity scale version already validated in Chile.
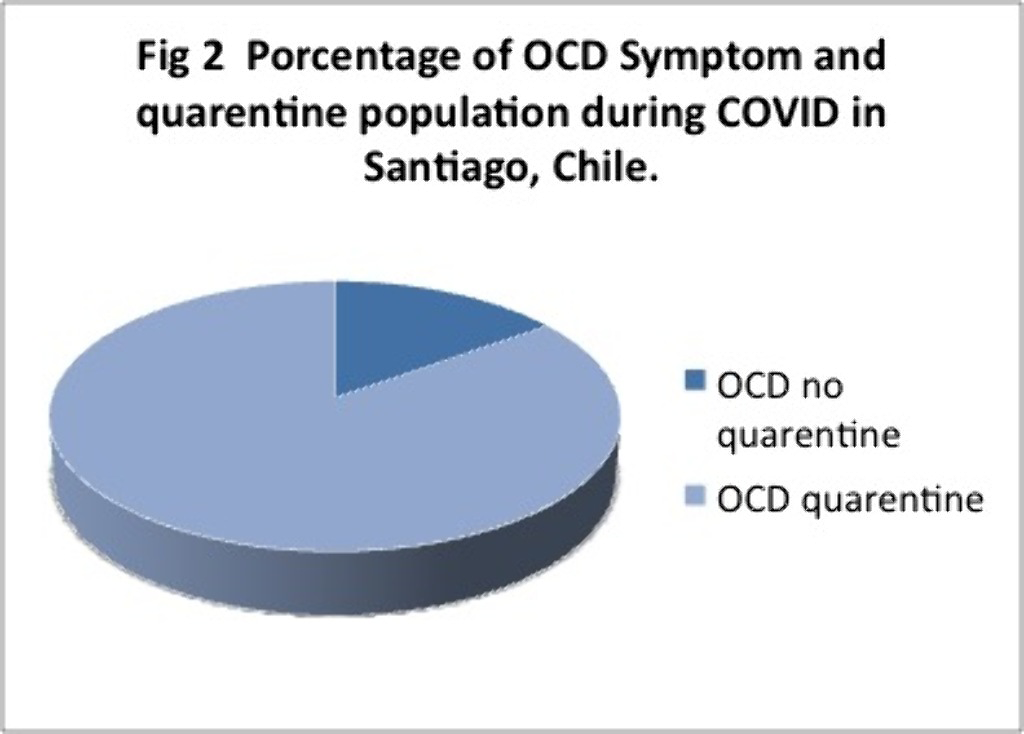
497 completed the survey and Y-BOCKS scale. 241 people which is equivalent to 48% of the sample presented scores that classified them as having OCD.Off these 30% had mild, 12% moderate and 7% severe symptoms. 85% of them were inquarantine for more than 2 months.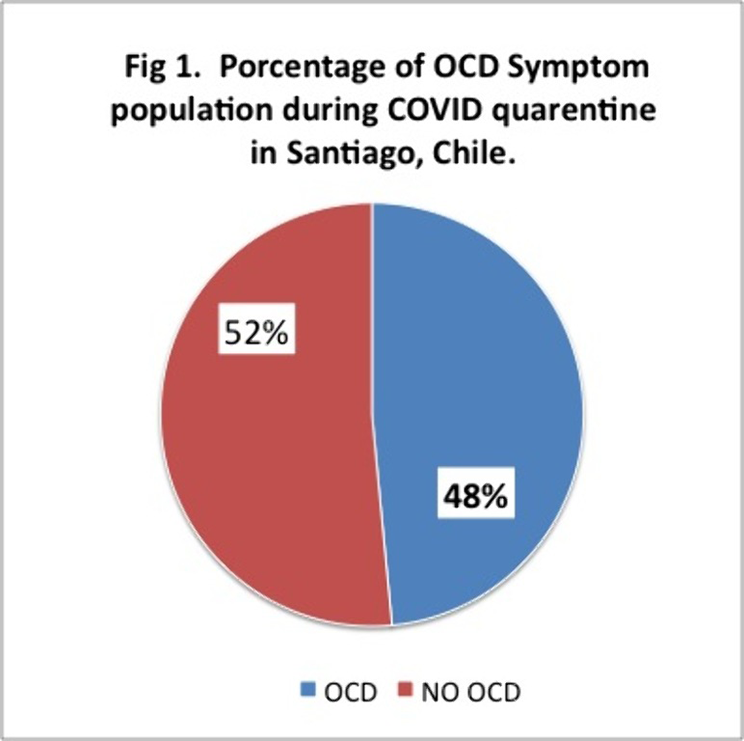
These results are above the 2% of OCD reported at the national level. These percentages may be due to a smaller sample size, but even so, the high percentages of people with symptoms during COVID and those who were in quarentine or lockdown for 2 months or more, stand out. Future analysis and research needs to be made. We ask ourselves wether is Covid, quarentine, or both and of so, how much each pf these contribute to these high percentages of OCD symptoms observed.

