This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
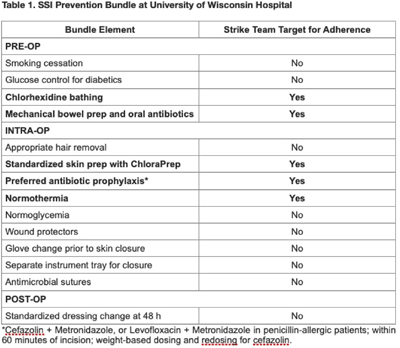
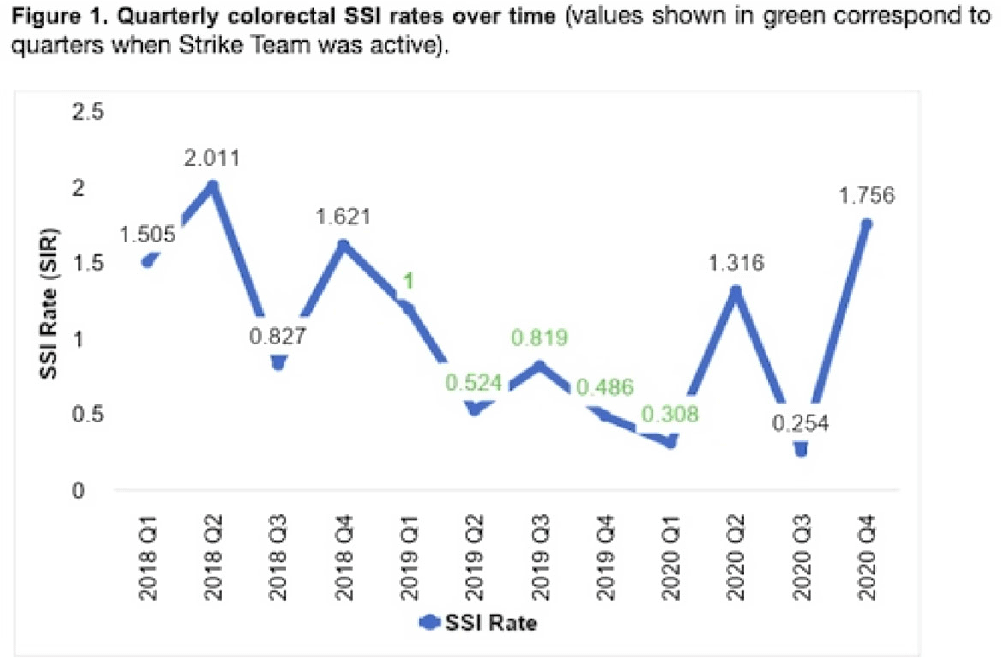
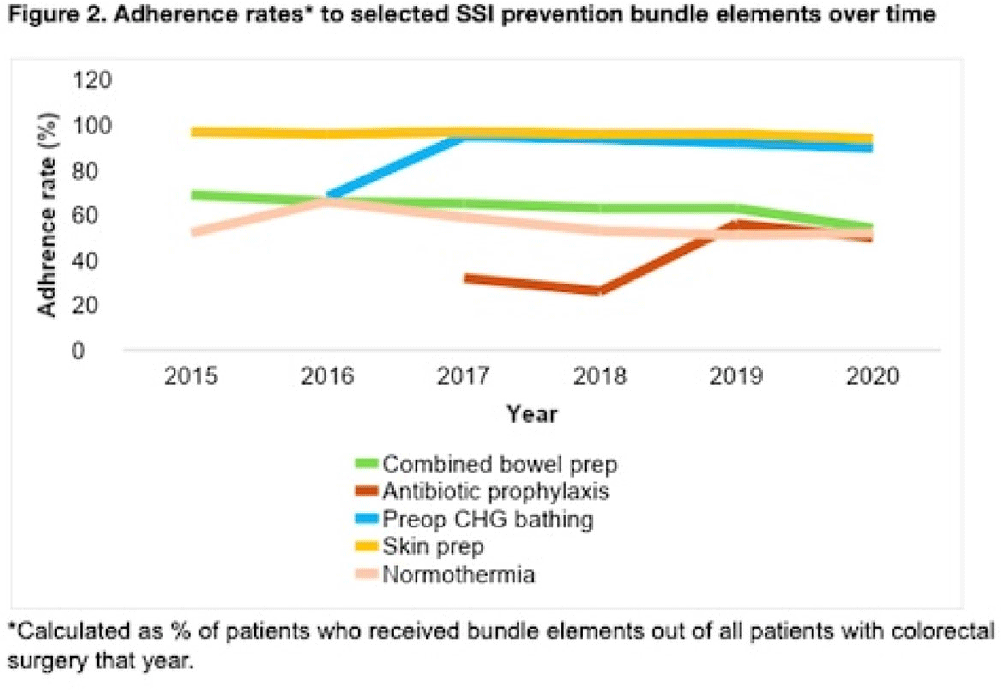
Background: Surgical site infections (SSIs) incur up to $10 billion annually due to their excessive morbidity. SSI prevention bundles have had variable success in colorectal surgery. For example, at the University of Wisconsin Hospital, a 505-bed regional referral center, SSI rates have remained high despite the introduction of a 14-element SSI prevention bundle in 2016. To aid in the implementation of this complex bundle, the hospital started Strike Teams in 2019. We have described the impact of Strike Teams on colorectal SSI rates in our tertiary-care hospital. Methods: A Strike Team with key stakeholders from colorectal surgery (ie, surgeon, OR director, nurses, surgical technicians), anesthesia, pharmacy, infection prevention, and infectious disease was formed, supported by the hospital’s executive leadership. The Strike Team met monthly throughout 2019 to review each SSI case, discussed barriers to adherence for the SSI prevention bundle elements with implementation difficulties (Table 1), and proposed actionable feedback to increase adherence. The latter was disseminated to frontline clinicians by the teams’ surgical leaders during everyday clinical practice. The Strike Team was paused in 2020 due to resource reallocation in response to the COVID-19 pandemic. Monthly and quarterly SSI surveillance was conducted according to CDC guidance. Results: Colorectal SSI rates before, after, and during Strike Team activity are shown in Fig. 1. Adherence rates to the bundle elements targeted by the Strike Team are shown in Fig. 2. Conclusions: Adherence to the preferred antibiotic prophylaxis increased, although adherence to other bundle elements of focus did not change significantly. SSI rates decreased below our expectation while the Strike Team was active in our hospital, although SSI reduction was not sustained. Further research should study the effectiveness of Strike Teams as a long-term implementation strategy for SSI prevention in colorectal surgery.
Funding: None
Disclosures: None
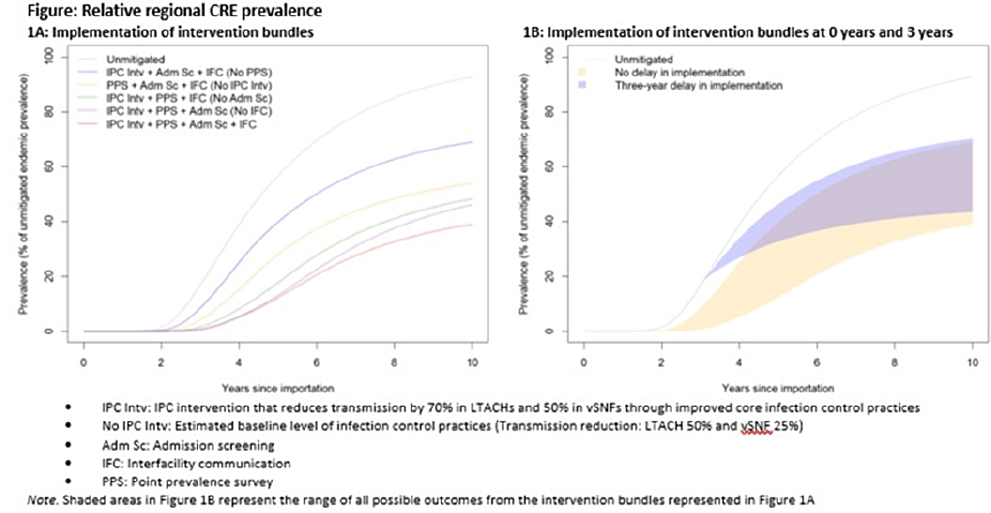
Background: Multidrug-resistant organisms (MDROs), such as carbapenem-resistant Enterobacterales (CRE), can spread rapidly in a region. Facilities that care for high-acuity patients with long average lengths of stay (eg, long-term acute-care hospitals or LTACHs and ventilator-capable skilled nursing facilities or vSNFs) may amplify this spread. We assessed the impact of interventions on CRE spread within a region individually, bundled, and implemented at different facility types. Methods: We developed a deterministic compartmental model, parametrized using CRE data reported to the NHSN and patient transfer data from the CMS specific to a US state. The model includes the community and the healthcare facilities within the state. Individuals may be either susceptible or infected and infectious. Infected patients determined to have CRE through admission screening or point-prevalence surveys at a facility are placed in a state of lower transmissibility if enhanced infection prevention and control (IPC) practices are in place. Results: Intervention bundles that included periodic point-prevalence surveys and enhanced IPC at high-acuity postacute-care facilities had the greatest impact on regional prevalence 10 years into an outbreak; the benefits of including admission screening and improved interfacility communication were more modest (Fig. 1A). Delaying interventions by 3 years is predicted to result in smaller reductions in prevalence (Fig. 1B). Increasing the frequency of point-prevalence surveys from biannually to quarterly resulted in a substantial relative reduction in prevalence (from 25% to 44%) if conducted from the start of an outbreak. IPC improvements in vSNFs resulted in greater relative reductions than in LTACHs. Admission screening at LTACHs and vSNFs was predicted to have a greater impact on prevalence if in place prior to CRE introduction (~20% reduction), and the impact decreased by approximately half if implementation was delayed until 3 years after CRE introduction. In contrast, the effect of admission screening in ACH was less (~10% reduction in prevalence) and did not change with implementation delays. Conclusions: Our model suggests that interventions that limit unrecognized MDRO introduction to, or dispersal from, LTACHs and vSNFs through screening are predicted to slow distribution regionally. Interventions to detect colonization and improve IPC practices within LTACHs and vSNFs may substantially reduce the regional burden. Prevention strategies are predicted to have the greatest impact when interventions are bundled and implemented before an MDRO is identified in a region, but reduction in overall prevalence is still possible if implemented after initial MDRO spread.
Funding: None
Disclosures: None
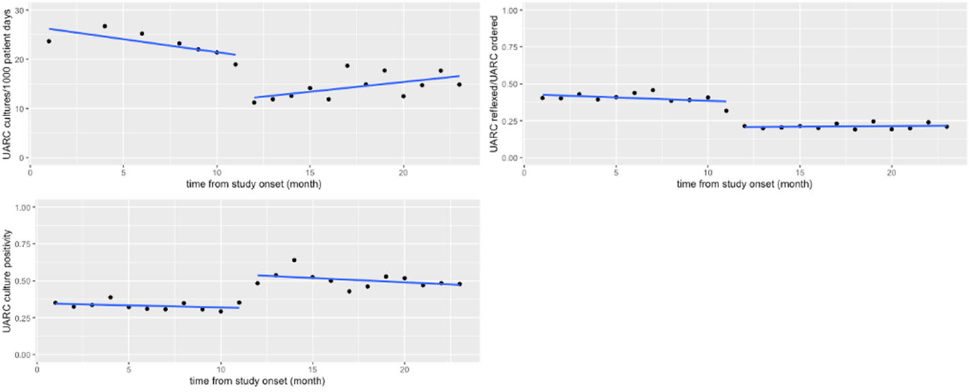
Background: Urinalysis and urine culture are frequently ordered diagnostic tests among hospitalized patients, often for nonspecific symptoms. Diagnostic testing stewardship with urinalysis with reflex culture (UARC) is a practice shown to reduce institutional culture rates by selecting patients who are more likely to have a true infection. Optimal reflex criteria are not well established, and downstream effects, such as antibiotic use, have not been well studied. Methods: We compared outcomes in the preimplementation period (December 2018 – October 2019) and postintervention period (November 2019–October 2020) at an academic medical center. The intervention was changing the UARC reflex criteria. The primary outcomes were urine-culture rate per 1,000 patient days, urine-culture positivity, antibiotic prescription for suspected urinary tract infection (UTI) and catheter-associated urinary tract infection (CAUTI) rate per 1,000 Foley catheter days. Analysis was performed using interrupted time-series negative binomial regression or Poisson regression where appropriate. Results: We detected a significant decrease in the rate of cultures performed (32.5 cultures per 1,000 patient days before the intervention vs 8.6 cultures per 1,000 patient days after the intervention; P = 0.10). Fig. 1 summarizes these results graphically. In an adverse events analysis, of 646 patients in the postintervention period, 130 patients were reviewed for the outcome of sepsis secondary to a urinary tract infection, with only 1 patient meeting criteria for this diagnosis. Conclusions: Changing the UARC reflex criteria resulted in the expected decrease in rate of cultures performed with increase in culture positivity, and the stricter criteria appeared to more effectively identify true UTIs. Minimal adverse events were associated with the UARC criteria change, demonstrating that these criteria are also safe. We detected a significant change in antibiotic prescriptions, but much of the decrease occurred during the preintervention period, which likely reflected educational and stewardship interventions performed at that time. Although the intervention affected culture performance, which does decrease institutional costs, continued provider education is needed to influence clinical outcomes.
Funding: None
Disclosures: None
Background: The impacts of health inequities on healthcare access, utilization, and outcomes have been highlighted by the COVID-19 pandemic, but these issues have been ongoing, yet understudied, in infectious disease epidemiology. Health inequities affect access to care, quality of care, and health outcomes in all healthcare settings. One healthcare setting that has yet to be fully studied in the context of health inequities is nursing homes. Nursing homes have a host of facility and population-specific issues that differ from other healthcare settings, making the impacts of health inequities likely unique and imperative to understand. The impacts of health inequities on nursing homes are unclear, and they likely have downstream effects on trends in morbidity, mortality, and transmission of multidrug-resistant organisms (MDROs) and other pathogens. Method: Here, we present a descriptive analysis, integrating multiple datasets relating to nursing home facility factors (data from the CMS Provider of Services and the CDC NHSN), nursing-home staffing trends (data from the CMS Payroll-Based Journal data), and social vulnerability (data from the CDC Social Vulnerability Index). We conducted a spatial analysis of nursing-home locations and the social vulnerability of the area. Results: Investigations of facilities and health inequities are best conducted in small spatial geographies. Analyses with less detailed spatial geographies miss high levels of heterogeneity in social vulnerability. Figure 1 provides an example, showing that analyzing nursing homes at a smaller spatial scale (ie, healthcare service area or HSA) shows heterogeneity in poverty levels that might be overlooked at a rough spatial scale, like Hospital Referral Regions (HRR). The poverty level associated with a nursing home will differ greatly depending on the geography of the analysis. Conclusions: These findings highlight that health inequities affect the quality and quantity of care of in nursing homes and that research conducted at larger geographical scales may overlook important mechanistic factors. This work will inform epidemiological models for disease transmission in nursing homes, accounting for the impacts of health inequities on transmission. Abating health inequities in all healthcare settings is a necessity to improve public health for the entire United States.
Funding: None
Disclosures: None

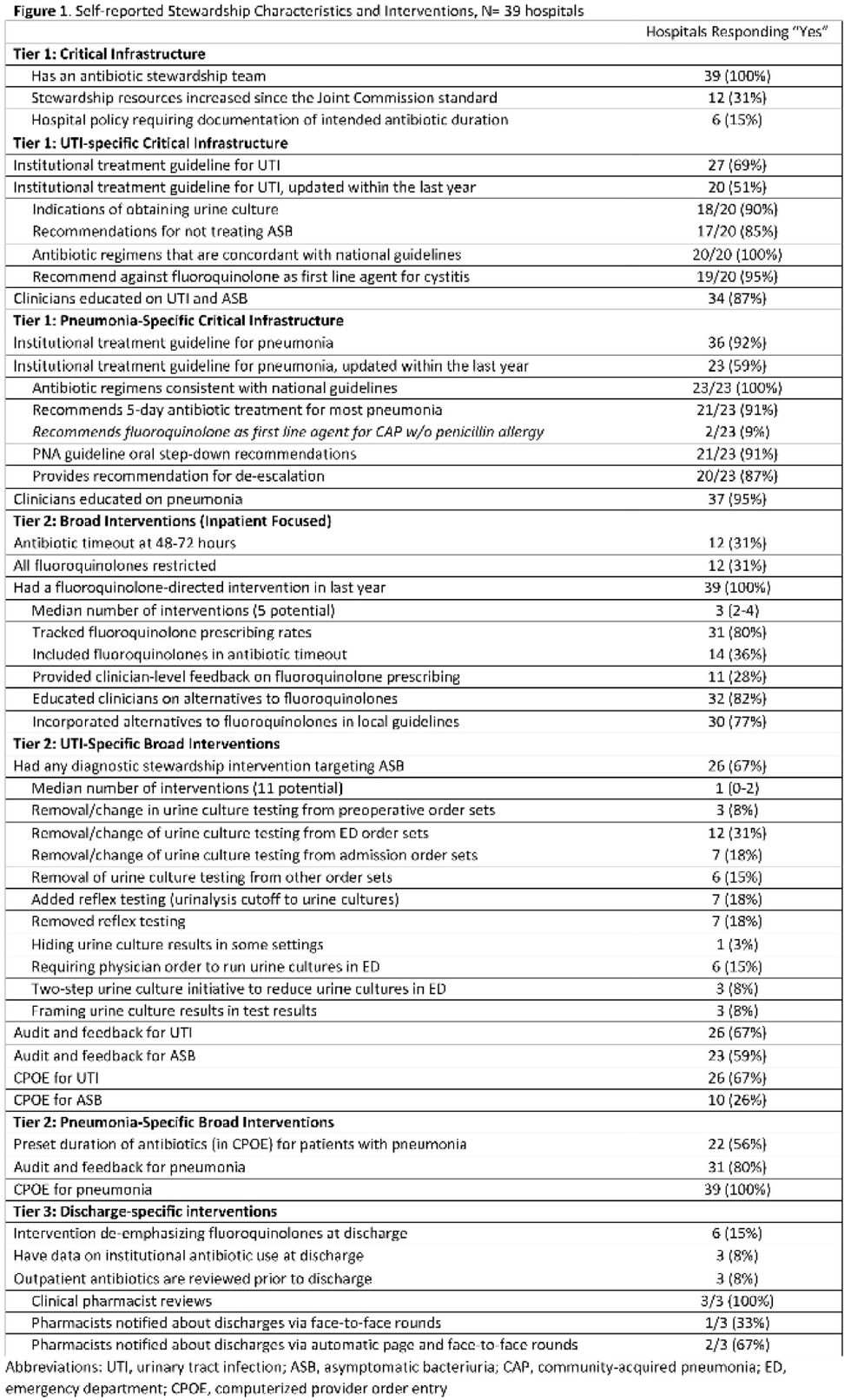
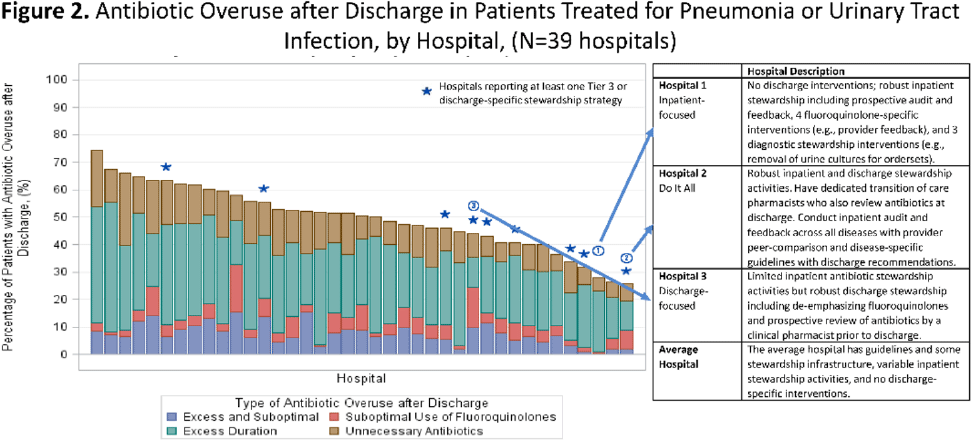
Background: Antibiotics are frequently prescribed–and overprescribed–at hospital discharge, leading to adverse-events and patient harm. Our understanding of how to optimize prescribing at discharge is limited. Recently, we published the ROAD (Reducing Overuse of Antibiotics at Discharge) Home Framework, which identified potential strategies to improve antibiotic prescribing at discharge across 3 tiers: Tier 1–Critical infrastructure, Tier 2–Broad inpatient interventions, Tier 3–Discharge-specific strategies. Here, we used the ROAD Home Framework to assess the association of stewardship strategies with antibiotic overuse at discharge and to describe pathways toward improved discharge prescribing. Methods: In fall 2019, we surveyed 39 Michigan hospitals on their antibiotic stewardship strategies. For patients hospitalized at participating hospitals July 1, 2017, through July 30, 2019, and treated for community-acquired pneumonia (CAP) and urinary tract infection (UTI), we assessed the association of reported strategies with days of antibiotic overuse at discharge. Days of antibiotic overuse at discharge were defined based on national guidelines and included unnecessary therapy, excess duration, and suboptimal fluoroquinolone use. We evaluated the association of stewardship strategies with days of discharge antibiotic overuse 2 ways: (1) all stewardship strategies were assumed to have equal weight, and (2) strategies weighted using the ROAD Home Framework with tier 3 (discharge-specific) strategies had the highest weight. Results: Overall, 39 hospitals with 20,444 patients (56.5% CAP; 43.5% UTI) were included. The survey response rate was 100% (39 of 39). Hospitals reported a median of 12 (IQR, 9–14) of 33 possible stewardship strategies (Fig. 1). On bivariable analyses, review of antibiotics prior to discharge was the only strategy consistently associated with lower antibiotic overuse at discharge (aIRR, 0.543; 95% CI, 0.335–0.878). On multivariable analysis, weighting by ROAD Home tier predicted antibiotic overuse at discharge for both CAP and UTI. For diseases combined, having more weighted strategies was associated with lower antibiotic overuse at discharge (aIRR per weighted intervention, 0.957; 95% CI, 0.927–0.987). Discharge-specific stewardship strategies were associated with a 12.4% relative decrease in antibiotic overuse days at discharge. Based on these findings, 3 pathways emerged to improve antibiotic use at discharge (Fig. 2): inpatient-focused strategies, “doing it all,” and discharge-focused strategies. Conclusions: The more stewardship strategies reported, the lower a hospitals’ antibiotic overuse at discharge. However, different pathways to improve discharge antibiotic use exist. Thus, discharge stewardship strategies should be tailored. Specifically, hospitals with limited stewardship resources and infrastructure should consider implementing a discharge-specific strategy straightaway. In contrast, hospitals that already have substantial inpatient infrastructure may benefit from proactively incorporating discharge into their existing strategies.
Funding: None
Disclosures: None
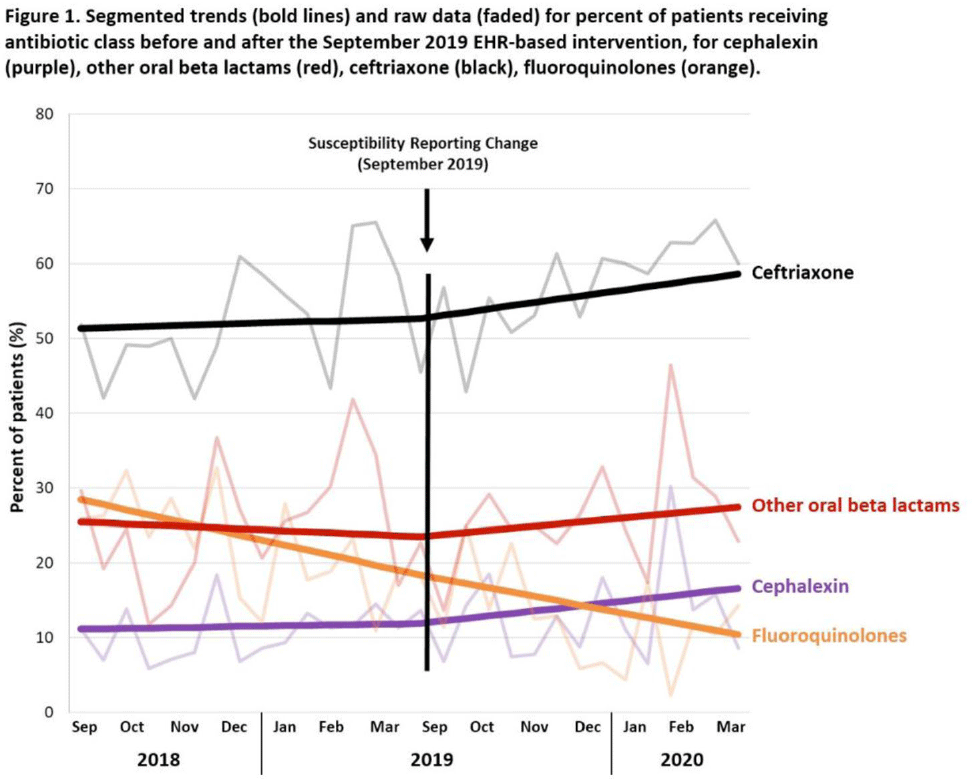
Background: Urinary tract infections (UTIs) are common in the inpatient, observation, and emergency department settings. Although many UTI-causing pathogens are susceptible to oral β-lactams, these agents are not tested directly, and susceptibility is extrapolated from other agents. To improve the use of these agents, the University of North Carolina Medical Center (UNCMC) added cephalexin to the susceptibility profile generated with urine culture results in the electronic health record (EHR). We evaluated prescribing trends of cephalexin, other oral β-lactams, fluoroquinolones, and other antibiotics for UTIs in the inpatient setting, before and after the susceptibility reporting change. Methods: An interrupted time-series analysis was conducted. Among 1,491 patients who had positive urine cultures with susceptibilities and received at least 1 antibiotic with a listed UTI indication during their inpatient stay at UNCMC, we measured the weekly prevalence (%) of patients who received each antibiotic group: cephalexin, other oral β-lactams (amoxicillin-clavulanate, cefdinir, cefuroxime), fluoroquinolones (levofloxacin, ciprofloxacin), and ceftriaxone. The study comprised a preintervention period (September 2018–March 2019) and a postintervention period (September 2019–March 2020). The prevalence of each antibiotic or group was plotted over time, and segmented linear regression was used to estimate the impact of the intervention on each antibiotic groups’ time trend. Results: At study baseline in September 2018, the weekly prevalence of antibiotic use was 11% for cephalexin, 26% for other oral β-lactams, 51% for ceftriaxone, and 29% for fluoroquinolones. Fluoroquinolone use decreased steadily throughout the study period, by 11% during the 7-month preintervention period (95% CI, −17% to −5%) and by 8% (95% CI, −13% to −3%) after the intervention (P for trend deflection, .70). In contrast, during the preintervention period, trends were flat for cephalexin, ceftriaxone, and other oral β-lactams (all P for nonzero preintervention slope were >.40). During the postintervention period, use increased for ceftriaxone (6%; 95% CI, 3%–9%). Post-intervention use also increased for cephalexin (5%; 95% CI, −3% to 12%) and other oral β-lactams (4%; 95% CI, −8%, 15%), but these trends were imprecise and not statistically significant at α = .05. Fig. 1 displays trends and raw data for each antibiotic group. Conclusions: The urine culture susceptibility reporting change was associated with small increases in cephalexin and ceftriaxone use, coincident with continued decreasing use of fluoroquinolones, for hospitalized patients with positive urine cultures and a listed UTI indication. Low-resource EHR-based interventions may confer considerable benefit for antimicrobial stewardship efforts in this clinical setting, and larger real-world studies are needed to replicate and contextualize these findings.
Funding: None
Disclosures: None
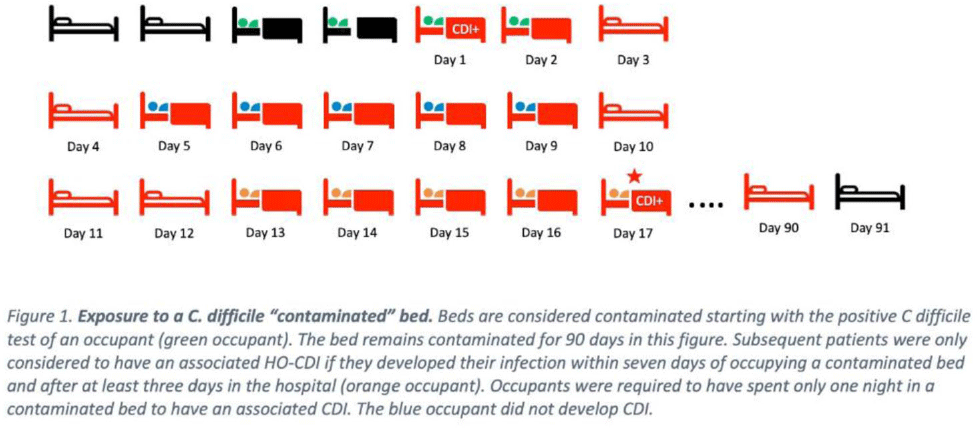
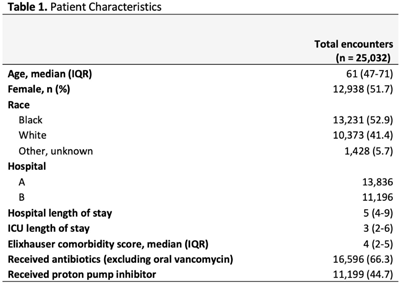
Background: Environmental contamination increases risk for Clostridioides difficile infection (CDI) given that spores can remain on a hospital bed, floor, sink, and light switch despite appropriate cleaning measures. Using real-time asset management software (AgileTrac, GE Healthcare) for beds we examined the risk of a patient developing hospital-onset CDI (HO-CDI) when staying in a hospital bed that had a previous occupant with CDI. Methods: We retrospectively identified all patients in tracked beds from April 2018 to August 2019 to identify hospital-onset CDI (HO-CDI), defined as a positive PCR test for C. difficile in a patient hospitalized for >3 days. A patient was defined as being exposed to a potentially “contaminated” bed if within the preceding 7 days from their HO-CDI diagnosis they resided in a hospital bed that, within the prior 90 days, had held an occupant with CDI (Fig. 1). We used multivariable logistic regression to evaluate the association between being exposed to a contaminated bed and HO-CDI. Model covariates were chosen a priori based on known risk factors for CDI. As a sensitivity analysis, we varied the length of time that a bed could stay contaminated from 90 to 60, 30, 14, and 7 days. Results: We analyzed 25,032 hospital encounters representing 18,860 unique patients; we identified 237 (0.9%) hospital encounters with HO-CDI (Table 1). The Elixhauser comorbidity score, being exposed to a contaminated bed, and receiving antibiotics or a proton pump inhibitor (PPI) during the hospital admission were all associated with HO-CDI in the univariable analysis (Table 2). In the adjusted multivariable model, being exposed to a contaminated bed remained a significant risk factor for HO-CDI (OR, 1.60; 95% CI, 1.22–2.08) even after controlling for known risk factors for CDI including age >65, elevated Elixhauser score, and recent antibiotic or PPI use (Table 2). In the sensitivity analysis in which we adjusted the time a bed was considered contaminated after CDI, being exposed to a contaminated bed remained a risk factor for HO-CDI, with a similar odds ratios as the original model (Table 2). Conclusions: Residing in a hospital bed that contained a previous occupant with CDI is a risk factor for developing HO-CDI. Hospital epidemiologists, infection control personnel, and environmental services staff should consider this association when developing CDI risk mitigation strategies.
Funding: None
Disclosures: None

Background: Although small- and medium-sized hospitals comprise most healthcare providers in South Korea, data on antibiotic usage is limited in these facilities. We evaluated the pattern of antibiotic usage and its appropriateness in hospitals with <400 beds in South Korea. Methods: A multicenter retrospective study was conducted in 10 hospitals (6 long-term care hospitals, 3 acute-care hospitals, and 1 orthopedic hospital), with <400 beds in South Korea. We analyzed patterns of antibiotic prescription and their appropriateness in the participating hospitals. Data on the monthly antibiotic prescriptions and patient days for hospitalized patients were collected using electronic databases from each hospital. To avoid the effect of the COVID-19 pandemic, data were collected from January to December 2019. For the evaluation of the appropriateness of the prescription, 25 patients under antibiotic therapy were randomly selected at each hospital over 2 separate periods. Due to the heterogeneity of their characteristics, the orthopedics hospital was excluded from the analysis. The collected data were reviewed, and the appropriateness of antibiotic prescriptions was evaluated by 5 specialists in infectious diseases (adult and pediatric). Data from 2 hospitals were assigned to each specialist. The appropriateness of antibiotic prescriptions was evaluated from 3 aspects: route of administration, dose, and class. If the 3 aspects were ‘optimal,’ the prescription was considered ‘optimal.’ If only the route was ‘optimal,’ and the dose and/or class was ‘suboptimal,’ but not ‘inappropriate,’ it was considered ‘suboptimal.’ If even 1 aspect was ‘inappropriate,’ it was classified as ‘inappropriate.’ Results: The most commonly prescribed antibiotics in long-term care hospitals was fluoroquinolone, followed by β-lactam/β-lactamase inhibitor (antipseudomonal). In acute-care hospitals, these were third-generation cephalosporin, followed by first-generation cephalosporin and second-generation cephalosporin. The major antibiotics that were prescribed in the orthopedics hospital was first-generation cephalosporin. Only 2.3% of the antibiotics were administered inappropriately. In comparison, 15.3% of patients were prescribed an inappropriate dose. The proportion of inappropriate antibiotic prescriptions was 30.6% of the total antibiotic prescriptions. Conclusions: The antibiotic usage patterns vary between small- and medium-sized hospitals in South Korea. The proportion of inappropriate prescriptions exceeded 30% of the total antibiotic prescriptions.
Funding: None
Disclosures: None

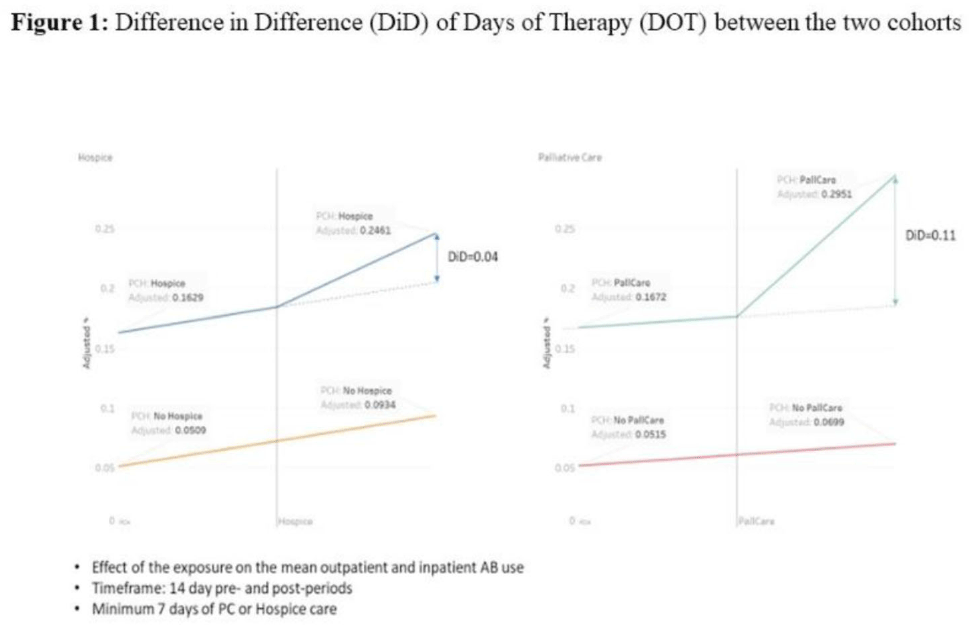
Background: Antibiotic use during end-of-life (EOL) care is an increasingly important target for antimicrobial stewardship given the high prevalence of antibiotic use in this setting with limited evidence on safety and effectiveness to guide antibiotic decision making. We estimated antibiotic use during the last 6 months of life for patients under hospice or palliative care, and we identified potential targets (ie time points) during the EOL period when antimicrobial stewardship interventions could be targeted for maximal benefit. Methods: We conducted a retrospective cohort study of nationwide Veterans’ Affairs (VA) patients, 18 years and older who died between January 1, 2014, and December 31, 2019, and who had been hospitalized within 6 months prior to death. Data from the VA’s integrated electronic medical record (EMR) were collected including demographics, comorbid conditions, and duration of inpatient antibiotics administered, along with outpatient antibiotics dispensed. A propensity-score matched-cohort analysis was conducted to compare antibiotic use between patients placed into palliative care or hospice matched to patients not receiving palliative care or hospice care. Repeated measures ANOVA and repeated measures linear regression methods were used to analyze difference in difference (D-I-D) of days of therapy (DOT) between the 2 cohorts. Results: There were 251,822 patients in the cohort, including 23,746 in hospice care, 89,768 in palliative care, and 138,308 without palliative or hospice care. The median days from last discharge to death was 9 days. The most common comorbidities were chronic obstructive pulmonary diseases (50%), malignancy (46%), and diabetes mellitus (43%). Overall, 18,296 (77%) of 23,746 hospice patients, and 71,812 (80%) of 89,768 palliative care patients received at least 1 antibiotic, whereas 95,167 (69%) of 138,308 who were not placed in hospice or did not receive palliative care received antibiotics. In the primary matched cohort analysis that compared patients placed into hospice or palliative care to propensity-score matched controls, entry into palliative care was associated with a 11% absolute increase in antibiotic prescribing, and entry into hospice was associated with a 4% absolute increase during the 7–14 days after entry versus the 7–14 days before entry (Fig. 1). The stratified cohorts had very similar balanced covariates as the overall cohort. Conclusions: In our large cohort study, we observed that patients receiving EOL care had high levels of antibiotic exposure across VA population, particularly on entry to hospice or during admissions when they received palliative care consultation. Future studies are needed to identify the optimal EOL strategies for collaboration between antimicrobial stewardship and palliative care.
Funding: None
Disclosures: None
Background: On March 5, 2020, the Tennessee Department of Health (TDH) announced the first case of COVID-19 in the state. Since then, hospitals have been overwhelmed by the spike in respiratory infections. Several studies have attempted to describe the impact of the pandemic on antibiotic prescriptions. The NHSN Antimicrobial Use Option offers a platform for hospitals to report their antibiotic usage. The TDH has established access to hospital antibiotic usage data statewide through an existing NHSN user group. We compared the change in the volume of inpatient antibiotic prescriptions before and during the pandemic. Methods: An ecological study was conducted from January 2019 to December 2021. Aggregated facility-level data from the NHSN Antimicrobial Use Option were used to describe antibacterial use among Tennessee hospitals. Data from facilities that had reported at least 1 month of data during the study period were included in this study. The antimicrobial use rate was calculated by dividing the antimicrobial days of therapy (DOT) by the number of 1,000 days present. Overall antimicrobial use rates as well as specific antimicrobial use rates for azithromycin, ceftriaxone, and piperacillin–tazobactam were compared across years. Results: In total, 55 hospitals reported at least 1 month of data into the NHSN Antimicrobial Use Option during the study period. These hospitals had a median bed size of 140 (range, 12–689). Conclusions: We observed a modest increase in overall antibiotic use during the COVID-19 pandemic in Tennessee facilities. This trend appeared to be primarily attributed to agents used for community-acquired respiratory infections, such as azithromycin and ceftriaxone, earlier in the pandemic. However, both of these agents have fallen to prepandemic use levels during 2021. The fact that overall use increased in 2021 suggests that other agents not analyzed may have contributed to this effect. Further analysis may help determine which agents are responsible for this increase in 2021.
Funding: None
Disclosures: None

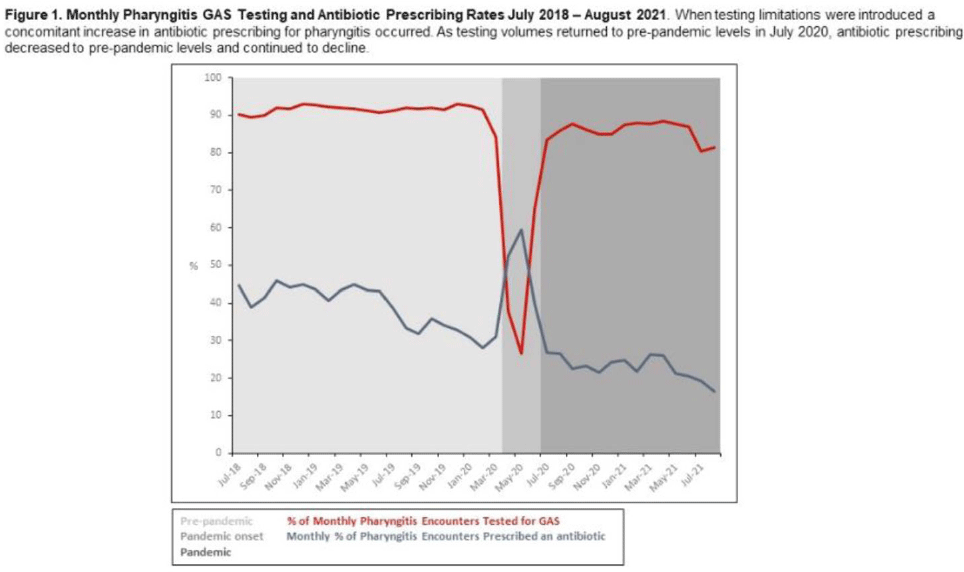
Background: Pharyngitis is 1 of the most common conditions leading to inappropriate antibiotic prescriptions. When personal protective equipment (PPE) was at first constrained during the COVID-19 pandemic, Intermountain Healthcare recommended limiting rapid group A streptococcal pharyngitis (GAS) testing in urgent-care clinics to preserve PPE. Notably, the percentage of pharyngitis encounters prescribed an antibiotic and that underwent GAS testing is a key Healthcare Effectiveness Data and Information Set (HEDIS) measure. We have described our experience with urgent-care pharyngitis encounters and the impact of temporarily reducing GAS testing on antibiotic prescribing before and during the COVID19 pandemic. Method: We identified all urgent care encounters between July 2018 and August 2021 associated with a primary diagnosis of pharyngitis using ICD-10 CM codes and a validated methodology. Pharyngitis encounters were assessed for antibiotic prescriptions ordered through the electronic health record (EHR) and the use of point-of-care rapid GAS tests. Pharyngitis encounters were analyzed monthly. We assessed the percentage of encounters associated with an antibiotic prescription regardless of testing and the percentage of encounters associated with an antibiotic prescription when a GAS test was or was not performed. We examined 3 periods relating to COVID-19 and GAS testing recommendations: the prepandemic period (July 2018–March 2020), the pandemic onset period (April 2020–June 2020), and the pandemic period (July 2020–August 2021). Results: Prior to the pandemic, the monthly percentage of pharyngitis encounters for which rapid GAS testing was performed was nearly 90% (Fig. 1). The average monthly percentage of urgent-care pharyngitis encounters prescribed an antibiotic was 38.9%, and the average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing was 90.4%. This HEDIS measure declined from 90.4% during the prepandemic period to 29.8% in the pandemic onset period when GAS testing was limited. Following resumption of routine testing practices the monthly percentage of urgent-care pharyngitis encounters for which rapid GAS testing was performed returned to levels ≥80% by July 2020 (Fig. 1). The average percentage of monthly pharyngitis encounters prescribed an antibiotic that also underwent GAS testing rose to 87.3% during this period. Conclusions: Limited PPE in our urgent care centers during the initial months of the COVID-19 pandemic was associated with a mandated substantial decline in rapid GAS testing. As testing volume decreased, we noted a simultaneous relative increase of >30% in antibiotic prescribing for pharyngitis. These findings suggest that rapid streptococcal testing promotes appropriate antibiotic prescribing.
Funding: None
Disclosures: None
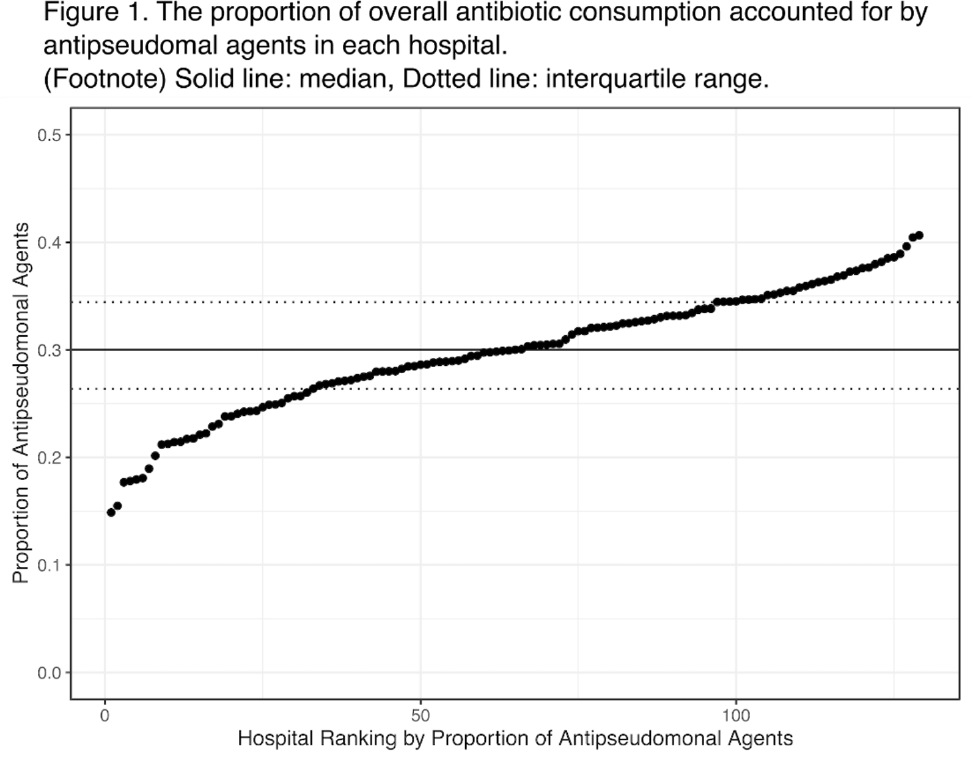
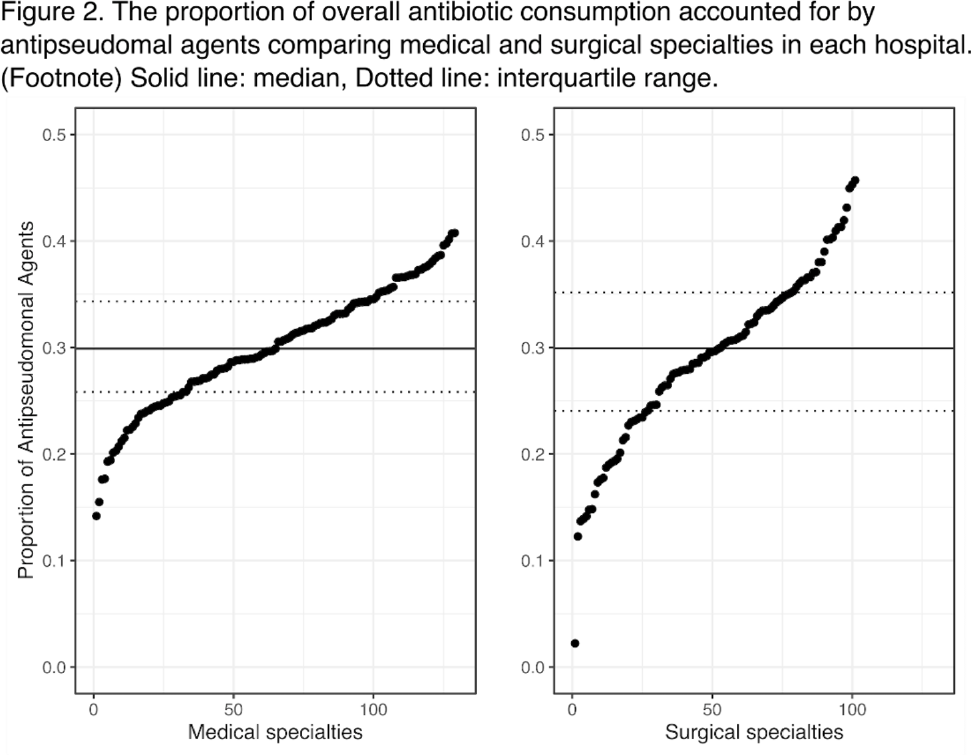
Background: Avoiding unnecessary antipseudomonal coverage is 1 of the most common targets for antibiotic stewardship programs (ASPs), but little is known about the magnitude of facility-level variation in antipseudomonal agent utilization. We aimed to describe the variability in the use of antipseudomonal agents across inpatient settings within a nationwide integrated healthcare system. Method: We analyzed the data from a retrospective cohort of patients who were admitted to acute-care hospitals within the VHA system in 2019. We defined antipseudomonal agents as systemic antibiotics with activity against wild-type Pseudomonas aeruginosa, and we evaluated overall and antipseudomonal antibiotic use among 129 hospitals, according to the agents described in the NHSN Antimicrobial Usage and Resistance Module. We calculated each hospital’s overall and antipseudomonal days of therapy (DOT) per 1,000 days present and the proportion of antipseudomonal agent usage among all antibiotics based on DOT at each hospital. Hospital-level variation was assessed by comparing the proportion of total antibiotic consumption accounted for by antipseudomonal agents. Associations between antipseudomonal proportions and overall antibiotic consumption were also assessed. Results: Among 129 VHA hospitals, the median DOT per 1,000 days present for all antibiotics was 434.4 (IQR, 371.9–487.1), and the median antipseudomonal DOT per 1,000 days present was 127.7 (IQR, 99.8–159.6). The median proportion of total antibiotic consumption accounted for by antipseudomonal agents was 30.0% (range, 14.9%–40.7%; IQR, 26.4%–34.4%) (Fig. 1). We detected only a weak correlation between overall antibiotic consumption and antipseudomonal proportion (Pearson correlation coefficient, 0.396), which suggests that hospitals with higher total antibiotic consumption were not necessarily using more antipseudomonal agents. In a stratified analysis, there was more prominent hospital-level variability in surgical specialties than medical specialties (Fig. 2). Conclusions: We detected high hospital-level variability in the consumption and proportion of antipseudomonal antibiotics among an integrated healthcare system. Although it is plausible that these variabilities originated from case-mix differences among hospitals, including differing rates of P. aeruginosa infections, it may also highlight opportunities for reducing antipseudomonal antibiotic utilization, especially among surgical specialties. Further studies are needed to evaluate the contribution of modifiable patient- and facility-level factors to this variability.
Funding: None
Disclosures: None
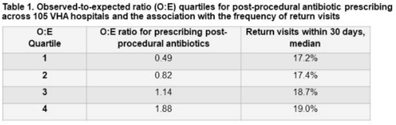
Background: Many urologists continue antibiotics after common urologic procedure beyond the timeframes recommended by professional guidelines. In this study, we sought to evaluate the association between postprocedural antibiotic use and patient outcomes. Methods: We identified all patients who underwent 1 of 3 urologic procedures (transurethral resection of bladder tumor [TURBT], transurethral resection of prostate [TURP], and ureteroscopy) within the Veterans’ Health Administration (VHA) between January 1, 2017, and June 30, 2021. A postprocedural antibiotic was any antibiotic potentially used for a urinary tract–related indication that was prescribed for administration after the day of the procedure. Outcomes were captured within 30 days of the procedure and included (1) return visits, defined as any emergency department or urgent care encounter or hospital readmission, and (2) Clostridium difficile infection (CDI), defined as a positive test for C. difficile and the prescription of an anti-CDI antibiotic. We used log-binomial models with risk adjustment to determine the association between postprocedural antibiotic use and outcomes. We constructed hospital-level observed-to-expected ratios for postprocedural antibiotic use, and we used these models to calculate the probability of each patient receiving postprocedural antibiotics. Results: Overall, we identified 74,629 patients; 98% were male; the mean age was 70 years (SD, 10). Among them, 50% underwent TURBT, 28% underwent TURP, and 23% underwent ureteroscopy. A postprocedural antibiotic was prescribed to 25,738 (35%) cases for a median duration of 3 days (IQR, 3–6). Return visits occurred in 13,489 patients (18%), and CDI occurred in 104 patients (0.1%). Patients exposed to postprocedural antibiotics had 16% more return visits (RR, 1.16; 95% CI, 1.13–1.20) and more than twice as much CDI (RR, 2.22; 95% CI, 1.51–3.26) than patients not exposed to postprocedural antibiotics. In log-binomial risk-adjusted analysis, the risk of return visits did not differ between the 2 groups (RR, 1.00; 95% CI, 0.97–1.04) but the risk of CDI was higher in patients who received post-procedural antibiotics (RR, 1.87; 95% CI, 1.00–3.51). Hospitals (n = 105) varied widely in their observed-to-expected ratios for prescribing postprocedural antibiotics, and the frequency of return visits was similar regardless of the frequency at which postprocedural antibiotics were prescribed (Table 1). Conclusions: Postprocedural antibiotics were prescribed beyond recommended intervals after more than one-third of common urologic procedures, with a large degree of variability across hospitals. The use of postprocedural antibiotics was not associated with fewer return visits but was associated with a nonsignificant increase in CDI risk. Efforts to reduce postprocedural antibiotics are needed.
Funding: Yes
Disclosures: This work was funded, in part, by the Merck Investigator Studies Program. This work was also supported by a Career Development Award (DJL) from the VA Health Services Research and Development Service (CDA 16-204) and by the Iowa City VA Health Care System, Department of Pharmacy Services.
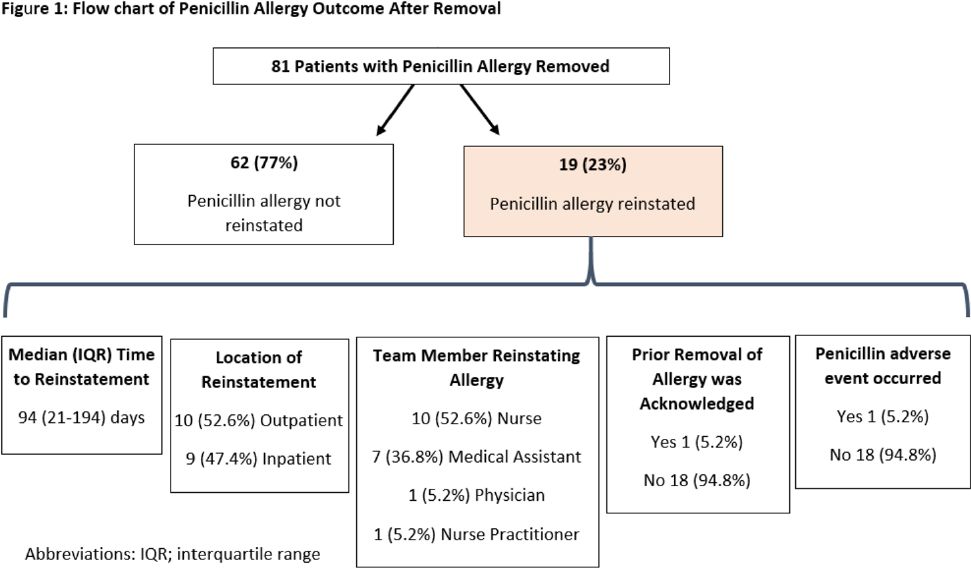
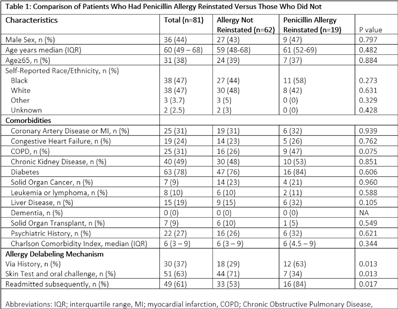
Background: Penicillin allergies are frequently reported and are associated with adverse clinical and antimicrobial stewardship outcomes. Allergy delabeling, either by patient history or skin testing and oral challenge can facilitate removal of penicillin allergy label. However, penicillinallergies are often reinstated in the medical record and data is limited about how and why this occurs. In our center, the departments of allergy and infectious diseases utilize an allergist nurse practitioner for penicillin allergy delabeling. We investigated the prevalence of penicillin allergy reinstatement following removal and associated factors thereof. Methods: We performed a retrospective observational study of patients who previously had penicillin allergy removed by the allergist nurse practitioner between August 2020 and May 2021 (250 days). Patients were followed for a minimum of 8 months and up to 16 months after penicillin allergy removal. We then assessed whether the allergy was reinstated. Clinical characteristics were compared between patients with penicillin allergy reinstated and not reinstated using the χ2 and Mann-Whitney U test. The primary end point was prevalence of penicillin allergy reinstatement following removal. Results: During the study period, 81 patients had penicillin allergy removed, but it was later reinstated in 19 patients (23%) (Fig 1). Median time to reinstatement was 94 days. Allergies were reinstated most frequently by nurses (53%) and medical assistants (37%). Reinstatement occurred in both outpatient (53%) and inpatient (47%) settings. In 18 of 19 cases, there was no acknowledgment that a prior assessment had determined the patient was not allergic to penicillin. Only 1 patient experienced a reaction prompting reinstatement of penicillin allergy. Once the allergy was redocumented, it was subsequently mentioned in a median of 17 notes per patient. Comorbidities did not differ between patients with allergy reinstated versus those without (Table 1). Patients with penicillin allergy reinstated were more often originally delabeled via history rather than skin test followed by oral challenge and were more likely to have been readmitted subsequently. Conclusions: Penicillin allergies were redocumented in almost one-quarter of patients, most frequently by a nonphysician team member and without acknowledgement of prior removal. Patients who undergo skin testing may be less likely to continue to report a penicillin allergy to medical staff compared to those whose allergy is removed based on history. Increased interactions with the healthcare system may have contributed to having the allergy reinstated.
Funding: None
Disclosures: None