


The need to understand why some people die by suicide and what can be done to prevent it is as acute now as it has ever been. Targeted strategies may contribute to a critical reduction in suicide,1 but suicide remains one of the three leading causes of death among those aged 15–44 and there are indications that for each adult who dies by suicide there may be more than 20 others attempting suicide.2 Although epidemiological and associated clinical research on suicide abounds,Reference Nock, Borges, Bromet, Cha, Kessler and Lee3, Reference Woodford, Spittal, Milner, McGill, Kapur and Pirkis4 one potentially relevant issue that has received virtually no attention internationally is that some individuals who die by suicide are reported missing to the police whereas other individuals are not.Reference Gibb and Woolnough5 This is despite the fact that risk of suicide is a key consideration for investigators when adults are reported missing.6
Suicide by missing persons
Official figures on the proportion of individuals who die by suicide who are reported missing remains unknown in the UK. A single study conducted in Queensland, Australia found a rate of 2.5%,Reference Sveticic, Too and De Leo7 but is unlikely to be applicable to the UK because of significant geographical and cultural differences. NewissReference Newiss8 examined fatal missing person cases reported to both the UK charity Missing People and the police and, consistent with national suicide rates,9 found most of those who were reported missing and died by suicide were male with an average age of 42 years. A quarter of the individuals who died by suicide and were reported missing were known to be under stress because of family or relationship issues and some had experienced a critical life event such as a death or the departure of a loved one.Reference Newiss8 Similarly, an earlier Australian study, comparing missing persons who had completed or attempted suicide with those who had run away and those who had been subject to foul play, found those who had attempted suicide were more likely to be male, aged between 41 and 65 years, single, without children, have depression and with a previous history of suicide attempts or threats and a number of acute and chronic stressors in their lives. In most cases the disappearance of the individual was considered out of character and in almost 80% the person reporting to the police suggested suicide as a possible motive, suggesting that family members and friends might be aware of the missing person's suicidal intentions.Reference Foy10
Comparing missing and non-missing person suicides
However, neither of the above studies were able to compare missing-person suicides with suicides where individuals were not reported missing. In the only international study that has allowed comparisons Sveticic et al Reference Sveticic, Too and De Leo7 found that compared with other suicides, individuals who were reported missing in Queensland, Australia were more likely to: be institutionalised and to have communicated their suicidal intent but be less likely to live alone, have a physical illness and/or alcohol problems. They were also more often found in natural outdoor locations and more frequently utilised motor vehicle exhaust gas toxicity, jumping from height or drowning and less frequently hanging as their method of suicide. However, as articulated by the authors themselves, the true number of missing people who died by suicide is likely to have been underrepresented in the study because of inconsistencies in Queensland police recording procedures and subsequent identification of the cases.
Consequently, beyond this cursory information, we know virtually nothing about why some individuals who die by suicide are reported missing and, critically, whether we can learn anything to inform practical action in terms of prevention and response. Therefore, two key questions arise: what percentage of individuals who die by suicide are reported missing in the UK and do those who are reported missing differ in any way from other individuals who die by suicide? This research represents the first UK study and only the second study worldwide to address this issue. We aimed to assess the rate of suicides that become reported as missing and to compare suicides by individuals reported missing to police in Scotland with suicides of people not reported missing in order to assess whether specific epidemiological, sociodemographic or circumstantial characteristics distinguish these groups and may have preventative or operational utility.
Method
Data were obtained from Grampian Police, Scotland (now Police Scotland North-East Division) sudden death reports where the cause of death was catalogued as suicide or undetermined and where the ‘date of death’ occurred between 1 January 2002 and 31 December 2004. Police Scotland North-East Division serves around 580 000 people11 over 8551 km2 and is a mixture of urban and rural communities in the North East of Scotland.12
It is widely acknowledged that some undetermined deaths are suicides and that to base research on suicide verdicts alone can result in bias. Similarly, to include all undetermined deaths as possible unproven suicides can be equally misleading.Reference Linsley, Schapira and Kelly13 Consequently, in contrast to previous research on suicide and missing persons,Reference Sveticic, Too and De Leo7 all undetermined deaths within the 3-year time period were reviewed and only those which were independently assessed and then collectively agreed by us to most likely be suicides were included in the final sample. Reasons for inclusion were a communication of suicidal intent (for example in the form of a suicide note or comment made to a friend or relative), evidence of psychiatric illness (in particular depression or suicidal tendencies), salient events (for example loss of employment, financial difficulties, failed relationship, anniversaries) and the specific circumstances of the death (for example significance of location found, method employed). Suicides related to people within secure accommodation (such as prison, psychiatric hospital) were excluded from the analyses as true freedom of choice regarding the method and location of suicide was constrained. Under this criterion, five people were excluded (four males in prison and one female in psychiatric care). The final sample comprised 160 individuals of these 18 (11.3%) were recorded as undetermined deaths. Ethical approval for this research was provided by the University of Teesside School of Science and Technology Ethics Committee, where E.M was an MSc student at the time the data collection was undertaken.
Scottish Police Death Reports contain details of the deceased's demographic features, antecedent information, medical history, the circumstances leading up to and surrounding the death and the cause of death as determined by a post-mortem examination. Related to this, most cases of individuals with a suicide verdict detailed a clear joint police/coroner (Procurator Fiscal in Scotland) classification of the suicide method that was used within this study. For open verdicts, and a small number of deaths by suicide, the method was not clearly specified in the report. For these, we discussed and agreed the most logical classification of method. We distinguished overdoses from poisonings on the basis that the latter involved fatal ingestion of chemicals (such as pesticide) whereas the former related to drugs (prescribed or illegal). Where people jumped from buildings or bridges the method was based on the clinical cause of death. On this basis, those dying as a result of impact with a hard surface were classified as a ‘fall from height’ (for example falling from an upper floor window onto a pavement); those jumping into water were classified as ‘drowning’ (i.e. jumping from a bridge into a river), those jumping in front of trains were classified as being ‘hit by a train’. For a small number of individuals it was not possible to determine a suicide method because of the level of decomposition associated with the body.
Distances from the deceased's current address to the location of suicide were calculated using Travelmanager GB Office© CD-ROM (1999). Bivariate analyses (χ2 statistics) were used to compare the individuals in the missing-suicide group with the other-suicide group for sociodemographic, medical and psychiatric variables, past suicidality and stressful life events, as well as suicide methods, locations where bodies were found, who found them and how they were found. Statistically significant differences were identified using a level of significance set at P<0.05.
Results
Prevalence
Of the 160 deaths, 36 (22.5%) were reported missing prior to being located (missing-suicide group) and 124 (77.5%) were not reported missing (other-suicide group). The relative percentage of individuals who died by suicide or by undetermined death that were reported as missing prior to location (88.8%, n = 32 and 11.1%, n = 4, respectively), was virtually identical to the relative proportion of people who died by suicide or by undetermined death in the overall sample (88.9%, n = 142 and 11.3%, n = 18, respectively). Therefore, there is equal representation and no reason to believe there is something distinct about individuals who died by suicide versus undetermined death in terms of whether they were reported missing or not. In the missing-suicide group, 27 (75.0%) were male and 9 (25.0%) were female. Similarly, in the other-suicide group, 98 (79.0%) were male and 26 (21.0%) were female. Thus, there were no differences between those reported missing and those that were not based on gender.
Epidemiological and sociodemographic characteristics
Table 1 presents sociodemographic, medical and psychiatric characteristics, past suicidality and recent stressful life events for the missing-suicide and other-suicide groups. Across all of the characteristics presented the only significant difference identified was that those in the missing-suicide group were more likely to be older than those in the other-suicide group. Importantly, there were no differences in terms of whether they had been in contact with their general practitioner in the past 3 months, whether they had been diagnosed with a mental or physical illness, and whether or not others perceived them to have an undiagnosed mental illness.
Table 1 Characteristics of missing-suicides and other-suicides

P-values in bold denote statistical significance at the P<0.05 level.
a. Where there were individuals with unknown or missing values these individuals were excluded (marital status: 4 (2.5%); employment status: 5 (3.1%); relationship status: 4 (2.5%); living arrangement: 11 (6.9%); diagnosed mental illness: 3 (1.9%); undiagnosed mental illness: 41 (25.6%); contact with general practitioner in past 3 months: 23 (14.4%); drug use: 11 (6.9%); alcohol problems: 105 (65.6%); left a note: 66 (41.3%)).
Depression was the most prevalent clinical diagnosis across both the missing-suicide (42.9%, n = 15) and other-suicide (40.2%, n = 49) groups. There were also no differences in terms of indications of suicidality. The three most common life events occurring in the lives of the missing-suicide group were: relationship breakdown/problems (30.6%, n = 11), physical health problems (19.4%, n = 7) and financial problems (16.7%, n = 6). There were, however, no significant differences between the missing-suicide and other-suicide groups in terms of the occurrence of specific stressful life events.
Suicide methods
Method was unknown for eight (5%) individuals. All of these were undetermined deaths and there was equal representation from the missing-suicide and other-suicide groups. These individuals were excluded from the analysis of methods. In line with Scottish national suicide statistics (2017),16 the most common method used across both the missing-suicide and other-suicide groups was hanging/ligature strangulation (59.2%) followed by overdose/poisoning (11.2%). Those in the missing-suicide group were no more likely to have died by hanging/ligature strangulation (50.0%, n = 16) than those in the other-suicide group (61.7%, n = 74) (Fig. 1). Drowning appears to occur at a higher frequency for those reported missing and who had taken their own life than for those in the other suicide group, however, sample sizes were too small for meaningful analysis (n = 9 v. n = 3).
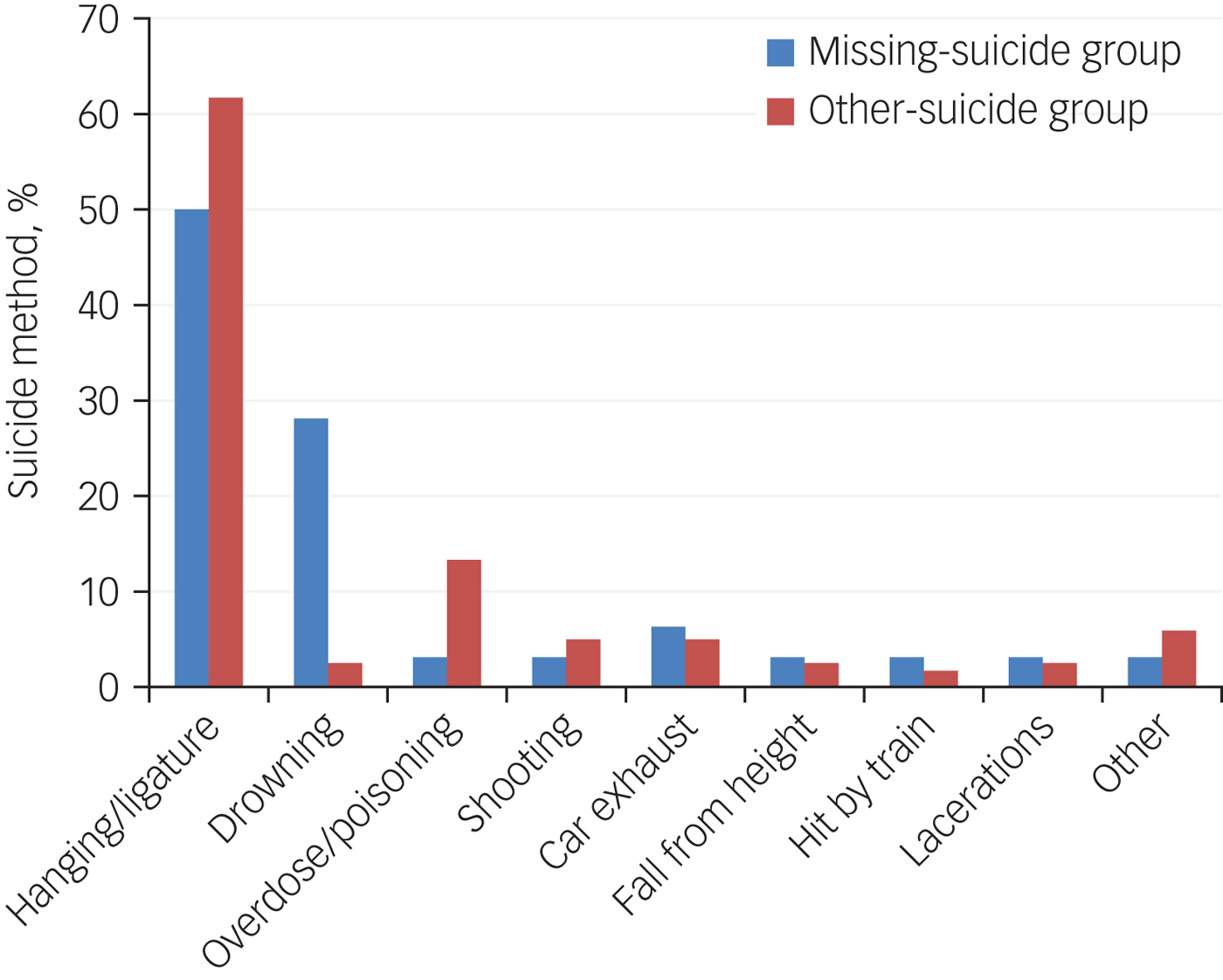
Fig. 1 Suicide methods employed in the missing-suicide and other-suicide groups.
Suicide locations
Across the whole sample, 104 people (65.0%) were found at their own residence, 38 (23.8%) in a natural outdoor location (such as beaches, woods, rivers, parks and golf-courses) and 18 (11.3%) in other locations (for example place of work, railway line, hotel room). There were no significant differences between the missing-suicide group and other-suicide group in terms of whether they were located in rural (44.4% (n = 16) v. 34.7% (n = 43)) or urban (55.6% (n = 20) v. 65.3% (n = 81)) areas. In the other-suicide group, the most common location of death was the person's home address (75.6% (n = 93) v. 30.6% (n = 11) in the missing-suicide group, χ2 = 24.98, d.f. = 1, P<0.001); one individual was excluded from this analysis as the individual was of no fixed abode). In contrast, in the missing-suicide group people were more likely to be found in natural outdoor locations (63.9% (n = 23) v. 12.1% (n = 15), χ2 = 41.33, d.f. = 2, P < 0.001) .
Distances travelled
Those in the missing-suicide group were significantly more likely to have travelled/be found a distance away from their place of residence than those in the other-suicide group (72.2% (n = 26) v. 41.9% (n = 52), χ2 = 10.243, d.f. = 1, P<0.001, one person was excluded from this analysis as the individual was of no fixed abode). Distances travelled by those in the missing-suicide group and the other-suicide group ranged from 0.00 km to 904.00 km and 805.00 km, respectively. The mean distance travelled by those in the missing-suicide group (32.05 km, s.d. = 156.51) was greater than the other-suicide group (12.99 km, s.d. = 80.11) but was not statistically significant. However, across the whole sample 97.5% were located no more than 60 km from their place of residence and for four people (2.5%) involved distances considerably larger than this (one person was in the missing-suicide group (found at 904 km) and three were in the other-suicide group (found at 268 km, 276 km and 805 km)). When these individuals are excluded from the analysis, the missing-suicide group (n = 35) travelled a mean distance of 7.14 km (s.d. = 10.67) and were found significantly further from their place of residence than the other-suicide group (n = 120) who travelled a mean distance of 2.07 km (s.d. = 7.79, t(153) = 3.095, P = 0.001).
Who they were found by
The other-suicide group were more likely to be found by someone within their social or daily living network (82.3%, n = 102) (i.e. a family member, friend, work colleague, community support worker, postman, housekeeper) than the missing-suicide group (16.7%, n = 6, χ2 = 54.716, d.f. = 1, P<0.001). In contrast, the missing-suicide group were more likely to be found by individuals in official search or public protection roles (36.1% (n = 13) v. 4.0% (n = 5) (i.e. the police, medical staff or search and rescue personnel), χ2 = 28.756, d.f. = 1, P<0.001) or members of the public (47.2% (n = 17) v. 13.7% (n = 17), χ2 = 18.724, d.f. = 1, P<0.001).
How they were found
The other-suicide group were more likely than the missing-suicide group to be found as a result of someone inadvertently coming across the body (73.4% (n = 91) v. 44.4% (n = 16), χ2 = 10.550, d.f. = 1, P<0.01) or as a result of family/friends actively searching (13.7% (n = 17) v. 0.0% (n = 0), χ2 = 5.522, d.f. = 1, P<0.05) (Fig. 2). In contrast, the missing-suicide group were more likely to be found as a result of an active police search (52.8% (n = 19) v. 3.2% (n = 4), χ2 = 55.657, d.f. = 1, P<0.001). It is of note that despite being recorded as missing to police and actively searched for, 44.4% (n = 16) of the missing-suicide group were not found as a result of the police search but were found inadvertently by someone coming across the body.
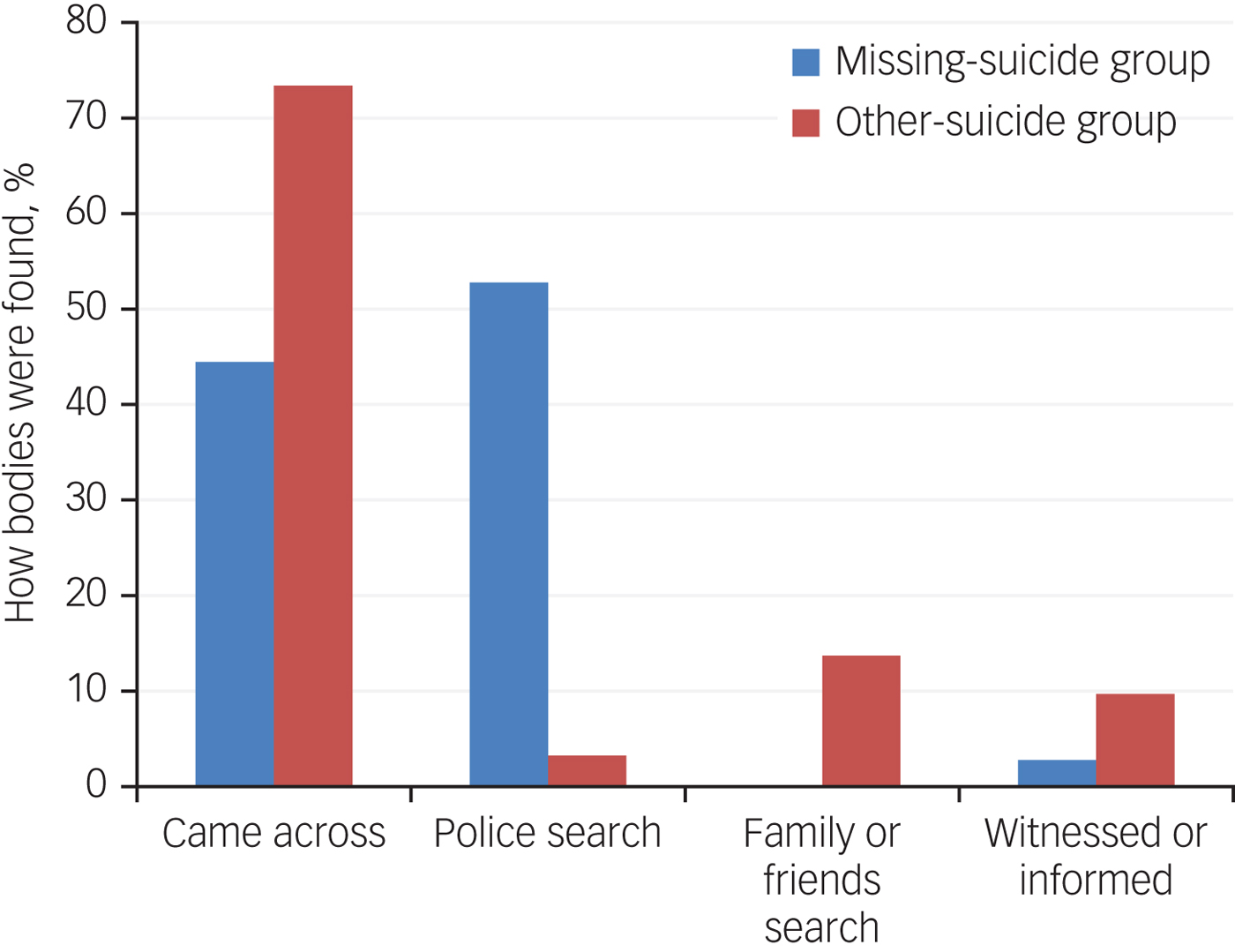
Fig. 2 How bodies were found in the missing-suicide and other-suicide groups.
Timescales
In terms of the passage of time between when the person was last seen and when they were found, the missing-suicide group had a mean duration of 33.9 days (s.d. = 108.53) and the other-suicide group a mean duration of 1.25 days (s.d. = 3.41, t(158) = 3.370, P = 0.001). Across the whole sample, 98.1% of individuals were located within 46 days. However, for three people (1.9%; all in the missing-suicide group) the timescale during which they were not located was considerably longer than this (140.97, 348.80 and 555.24 days). After exclusion of these three individuals from analysis, the mean duration of 5.31 days (s.d. = 9.44) in the missing-suicide group (n = 33) was still significantly longer than in the other-suicide group (n = 124, where the mean duration was 1.25 days (s.d. = 3.41, t(155) = 3.942, P<0.001).
Discussion
Almost a quarter of all suicides in the current study were reported missing to the police prior to their location. This is considerably higher than identified in previous research, which found a rate of 2.5%Reference Sveticic, Too and De Leo7 and most likely reflects more robust recording and sampling of police records in the current study. In 2017 there were 680 probable suicides registered in Scotland.14 If police-led searches are activated in approximately 25% of these, we can extrapolate and estimate that the police in Scotland were involved in searching for approximately 170 individuals who died by suicide that year. In the UK over 370 000 incidents of missing people are reported to the police annually.15 The police have to risk assess and respond accordingly to all incidents and risk of suicide is a key consideration for investigators when adults are reported missing.6 It is important to note that some individuals reported missing to the police and who die by suicide may already be dead at the time they are reported, and thus not offer preventative opportunities irrespective of the effectiveness and efficiency of the police response. However, in conversation with P.W. police officers have indicated that using initial evidence-based response parameters (for example geospatial missing persons guidanceReference Gibb and Woolnough5) has allowed them to locate potential suicide victims more efficiently and prevent death at that time. The relatively small number of individuals who die by suicide reported missing to the police, in comparison with the much larger volume of missing people reported overall,15 highlights the critical importance of the police role in risk assessing and responding to potential suicide, and the importance of the development of evidence-based risk assessment and response tools and techniques to facilitate quick response and to maximise the possibility of finding people alive.
Absence of epidemiological or sociodemographic differences
There was no difference between the missing-suicide and other-suicide groups based on gender. In line with existing research and national statisticsReference Sveticic, Too and De Leo7–Reference Foy10 approximately three-quarters of individuals in both the missing-suicide and other-suicide groups were males. Interestingly, people in the missing-suicide group were likely to be slightly older than those in the other-suicide group. In general, risk of suicide increases with age,16 so is possible that this age difference is indicative of an increased concern for older individuals and therefore an increased propensity to report them missing. We found no other differences between those in the missing-suicide and other-suicide groups. This contrasts with Sveticic et al Reference Sveticic, Too and De Leo7 who found differences in terms of: marital status, employment status, living arrangements; physical and mental health; indications of suicidality or experience of stressful life events. However, differences/potential biases in sampling could account for the difference in findings. Consequently, on the basis of these findings, it is argued that health practitioners and emergency responders should not view suicidal individuals who are reported missing as clinically different from suicidal individuals not reported missing.
With 80% of missing adults estimated to have a mental health problemReference Gibb and Woolnough5 and adults with a mental health diagnosis being more vulnerable to going missing on more than one occasion,Reference Woolnough and Gibb17 the role of health practitioners in identifying those at risk of going missing (not necessarily suicidal) remains. Indeed, emerging government strategies have begun to call for healthcare providers to ensure prevention planning takes place for patients at risk of going missing and to agree local protocols on information sharing with police.18 However, the notion that individuals who take their own life who have been reported as missing are epidemiologically or sociodemographically different from those who take their own lives but have not been reported missing does not appear to be the case.
Complex interplay between suicide location and being found
Sveticic et al Reference Sveticic, Too and De Leo7 found individuals who were reported missing and died by suicide more frequently utilised motor vehicle exhaust gas toxicity, jumping from height or drowning and less frequently hanging, whereas we found no significant differences between the missing-suicide and other-suicide groups in terms of suicide method. The relatively small sample size in this study may have prevented differences from reaching significance. Drowning, for example, occurred at a higher frequency in the missing-suicide group but numbers were too small for meaningful analysis. Alternatively, this could be indicative of geographical and/or cultural variation and highlights the importance of studies in different jurisdictions to inform local and global understanding. In contrast to method, location did emerge as an important distinguishing feature. As with existing research there were no significant differences between the two groups in terms of whether they were located in rural or urban areas. But, for the other suicide group the most common location of death was the person's home address, whereas for the missing-suicide group they were more likely to be found in natural outdoor locations.
People in the other-suicide group was more likely to be found by someone known to or directly connected to them in some way (i.e. someone within their social or daily living network) than those who were reported missing. Despite the fact that people who report someone missing are likely to be actively out looking for them,Reference Parr, Stevenson and Woolnough19 the individuals in the missing-suicide group were more likely to be found as a result of an active police search or by members of the public. Importantly, just under half of the missing-suicide group were found inadvertently by a member of the public coming across the body rather than as a result of the organised police search. The missing-suicide group were also more likely to have travelled, travelled further and took significantly longer to find than those in the other-suicide group.
Taken together, these findings suggest that there is a complex interplay between the location the suicide took place, who finds the person, how the person is found and the timescales associated with this that distinguishes those who are reported missing and die by suicide from those who are not reported missing. Specifically, those who take their own life but have not been reported missing tend to be found dead at home (or in a location where there is regular foot fall) and someone naturally/inadvertently comes across them as part of daily routines before anyone has considered them as ‘missing’ from their expected social obligations.Reference Payne20 In contrast, those individuals who are reported missing and die by suicide are ‘missed by someone’ as they are not located where they are expected to be.Reference Biehal, Mitchell and Wade21 They are also more likely to be located in natural outdoor locations and harder to find without an organised, systematic police-led search. Hence, immediate cursory searching by family and friends fails to locate them and they are reported missing to police.Reference Parr, Stevenson and Woolnough19 When individuals who are reported missing and take their own life are located in particularly unexpected locations or are well concealed, the police-led search may be inconclusive and the person may subsequently be found inadvertently by a member of the public (often walking a dog) sometime after being reported missing. Just under half of the missing-suicide group in our study were found by members of the public. This is undoubtedly a highly traumatic experience and so we need to increase the rate at which such individuals are located by police and suitably trained professionals.
Methodological challenges and future research
Although the sample within this study was robustly identified and included undetermined deaths, it was relatively small, preventing in-depth analysis of some data, and only related to one region of Scotland. In addition, it is possible that not all suicides in the time frame for this research were captured. Specifically, during the sample time frame a very small number of unresolved missing person cases may have occurred. It is possible that some of these could have been suicides and included in this sample. Although the latter is difficult to overcome, future research with larger sample sizes would be beneficial. Research in different jurisdictions is needed to explore the extent to which the findings presented here might be contextually and/or geographically dependent and explain differences observed between this study and Sveticic et al.Reference Sveticic, Too and De Leo7 As the police are the lead agency for missing people, yet almost 50% of individuals who die by suicide and have been reported missing are located by members of the public, future research should be undertaken to develop tools/techniques to inform police risk assessment of suicide in missing person cases and to support both the investigation and search response in such cases.
While other research speaks of individuals reported missing prior to death,Reference Sveticic, Too and De Leo7 this may not be the case as death may have occurred many hours or even days prior to an individual being reported missing to the police. Importantly, the decision to report someone missing is not made until someone within the individual's social networkReference Payne20 ‘misses’ the individual and feels sufficiently compelled to contact the police and they therefore become reported/recorded as a missing person. The correct language to use, then, is ‘prior to location’ rather than ‘prior to death’.
In conclusion, our study aimed to compare suicides by people reported missing to police in Scotland with suicides by people not reported missing in order to assess whether specific epidemiological, sociodemographic or circumstantial characteristics distinguish these groups. Overall, the findings suggest there is no obvious reason to believe that suicides in individuals that begin as missing person investigations differ from those in individuals not reported missing in terms of epidemiological or sociodemographic characteristics. Instead, observed differences relate to whether the individual is ‘missed’ by someone within their social circle and the circumstances surrounding the death in terms of how difficult they are to find based on a combination of unusualness of location, distance from home and level of concealment.
Acknowledgements
We would like to thank Grampian Police (now North-East Division of Police Scotland) for their assistance with data collection and Professor Julie Mennell for her initial contribution to the design of this study. We also thank Iain Murray, ChooseLife, Aberdeenshire, for a critical reading of a draft of this article.




 Open access
Open access
eLetters
No eLetters have been published for this article.