



In 1990, Jenkins identified an urgent need for a system of indicators to enable clinicians to monitor and evaluate mental healthcare.Reference Jenkins1 One reason identified for not routinely using standard outcome measures was the lack of appropriate instruments.Reference Slade, Thornicroft and Glover2 In 1998, Wing et alReference Wing, Beevor, Curtis, Park, Hadden and Burns3 developed the Health of the Nation Outcome Scales (HoNOS), an instrument covering symptoms, functioning, relationships and environmental issues,Reference Laugharne, Eaves, Mascas, Psatha, Dinnis and Trower4,Reference Kisely, Campbell, Cartwright, Cox and Campbell5 which could be used routinely in the UK National Health Service to measure progress toward the target set by the UK Department of Health ‘to improve significantly the health and social functioning of mentally ill people’.6 Since then, the HoNOS and its adaptations for children and adolescents (HoNOSCA) and for those aged >65 years (HoNOS65+), have been officially adopted in England, Australia, New Zealand and other European countries.Reference Lovaglio and Monzani7–Reference James, Painter, Buckingham and Stewart10
Gowers et alReference Gowers, Harrington, Whitton, Lelliott, Beevor and Wing11 developed the HoNOSCA as a set of scales to be used in Child and Adolescent Mental Health Services.Reference Gowers, Bailey-Rogers, Shore and Levione12 The HoNOSCA has been widely used.Reference Laugharne, Eaves, Mascas, Psatha, Dinnis and Trower4,Reference Hanssen-Bauer, Gowers, Aalen, Bilenberg, Brann and Garralda13–Reference Brann, Alexander and Coombs19 It was designed to be brief, have a similar structure to the HoNOS and provide a broad, quantitative measure of severity to measure a range of behavioural, symptomatic, social and impairment domains in children and adolescents and it has been found to have sound psychometric properties.Reference Gowers, Harrington, Whitton, Lelliott, Beevor and Wing11,Reference Pirkis, Burgess, Kirk, Dodson and Coombs20,Reference Brann, Coleman and Luk21
In Australia, the National Outcomes and Casemix Collection (NOCC) was introduced ‘to provide a suite of measures that support clinical practice and comparisons across services and different consumer populations’.Reference Brann, Alexander and Coombs19 This saw the implementation of a range of outcome measures to routine clinical practice across age groups. At the core of the NOCC was the family of clinician-rated HoNOS. A review of NOCC22 identified a measurement gap for infants and pre-schoolers.
The Australian Child and Adolescent Mental Health Information Development Expert Advisory Panel (CAMHIDEAP)23 provides advice to the Australian government on mental health information development in Australian child and adolescent mental health services. Several members of CAMHIDEAP participated in a collaborative international review of the interrater reliability of HoNOSCA.Reference Hanssen-Bauer, Gowers, Aalen, Bilenberg, Brann and Garralda13 This study also involved participants from the UK, Denmark, Norway and New Zealand. CAMHIDEAP members, including Dr Peter Brann, Dr Tim Coombs and Dr Sally Merry as the New Zealand representative, commenced conversations with the other participants in the HoNOSCA interrater reliability study about the development of a measure for infants and pre-schoolers, i.e. the Health of the Nation Outcome Scales for Infants (HoNOSI).24 Australia and New Zealand, through the CAMHIDEAP, commenced the measure development work, with the initial mapping of domains undertaken by Dr Sally Merry. The CAMHIDEAP had formed a working group to look broadly at routine outcome measures in the very young and supported by the results of the review of the NOCC, took ownership of the HoNOSI initiative, developing and refining a measure suitable for sector consultation and field trialling.
Face validity testing25 showed that the HoNOSI was perceived to fill a much needed gap in infant mental health outcome measurement for the 0–47 month age group (infants and pre-schoolers). Following subsequent concurrent validity testing,Reference Brann, Culjak, Kowalenko, Dickson, Coombs and Burgess26 the CAMHIDEAP Working Group identified the need to test the interrater reliability of the HoNOSI.
Aims
This HoNOSI field trial was designed to examine interrater reliability, exploring the degree of agreement among different raters when rating the same case vignettes with the HoNOSI.
Method
A pilot study with three vignettes was conducted by a panel of CAMHIDEAP Working Group members, along with individuals with expertise in infant mental health or mental health measurement. The pilot study identified that the vignettes were substantially more severe than the real cases in the concurrent validity study. The vignettes’ severity was adjusted to accord with the real cases and two more vignettes were added. The current study used the resulting five vignettes. The age and gender of the vignettes were 4 months (female), 9 months (male), 3 years (female), 3 years (female) and 4 years (male). The vignettes can be found within the full HoNOSI Field Trial Report.25 Presenting problems included perceived agitation, aggressiveness (9 months), a paediatric in-patient referral with feeding problems, sensory underresponsiveness and maternal depression (4 months).
For the current study, participants with expertise in infant and pre-school mental health were asked to rate these vignettes. Ethics and research governance approval was obtained from the relevant ethics committee for participants from the Centre for Perinatal and Infant Mental Health and Child and Youth Mental Health Service in Queensland (HREC Ref: HREC/16/QRCH/424) , and for participants from the Eastern Health Child Youth Mental Health Service in Victoria (HREC Ref: LR19/040). A total of 45 people participated in the study; 26 from Queensland and 19 from Victoria. All participants received a brief online training session on the measure,Reference Brann and Coombs27 covering areas such as the rating rules and inclusion and exclusion criteria. Upon providing consent via the online consent form, the five vignettes were independently rated online. Those making the ratings were presented with the vignette and then the HoNOSI glossary, from which the rater selected their preferred rating. Results were analysed with Stata statistical software, version 16.1 for Windows.28 Interrater reliability was assessed with quadratic weighted kappa. A copy of the vignettes is available from the corresponding author, upon request.
The HoNOSI24 is a 15-item set of scales, rated from 0 to 9, with 0 indicating no problem, 1 indicating a minor problem requiring no formal action, 2 indicating a mild problem, 3 indicating a problem of moderate severity, 4 indicating a severe to very severe problem and 9 indicating not known or not applicable.
The total score is calculated by summing the first 13 scales, which relate to infant mental health status. Missing data is treated as zero in calculating totals. As with the HoNOS family of measures, clinicians typically classify ratings as ‘clinically significant’Reference Burgess, Trauer, Coombs, McKay and Pirkis29 if a problem area is rated as either a Mild, Moderate or Severe to Very Severe problem (i.e. a rating of 2, 3 or 4). A list of HoNOSI scales can be found in Appendix 1.
The strength of agreement between raters was measured against the COnsensus-based Standards for the Selection of Health Measurement INstruments (COSMIN).30 The COSMIN initiative30 was developed to provide guidance on the selection of outcome measures for clinical and research applications.Reference Prinsen, Mokkink, Bouter, Alonso, Patrick and de Vet31 The COSMIN includes a methodology for assessing the interrater reliability of measures,30,Reference Mokkink, Prinsen, Patrick, Alonso, Bouter and de Vet32 a taxonomy and definitions of measurement properties,Reference Mokkink, Terwee, Patrick, Alonso, Stratford and Knol33 checklists for assessing the methodological qualityReference Mokkink, de Vet, Prinsen, Patrick, Alonso and Bouter34 and criteria for good measurement properties.Reference Prinsen, Mokkink, Bouter, Alonso, Patrick and de Vet31 For measures constructed with ordinal ratings (i.e. the rating categories indicate the relative ordering of ‘clinical severity’), the gold standard for reporting is the weighted kappa,Reference Mokkink, Prinsen, Patrick, Alonso, Bouter and de Vet32 where reliability is sufficient if κw ≥ 0.7. The standards outlined by Landis and KochReference Landis and Koch35 are commonly used in discussions of reliability and will also be reported to both facilitate comparison and support interpretation.
Results
Of the 45 raters, 39 completed all five vignettes with no missing values. Five raters had a missing rating for one scale with one vignette and one rater had a missing rating for one scale with two vignettes. No HoNOSI scale ratings were rated as 9 (not known/not applicable). In accordance with the rating rules used by the HoNOSCA, all vignettes were able to have total scores calculated.Reference Pirkis, Burgess, Kirk, Dodson and Coombs20 Table 1 shows descriptive statistics and the HoNOSI total score distribution for each of the five case vignettes. The percentiles indicate the total score that occurred at that percentage of the distribution. For example, for Levi, a score of 17 was >10% of the total scores. A score of 18 was >25% of total scores. The 50th percentile is the median score. Percentiles aid in describing the distribution and spread of total scores for each vignette.
Table 1 Distribution of Health of the Nation Outcome Scales for Infants total score for the five vignettes

All of the possible HoNOSI ratings (0, 1, 2, 3, 4) were utilised for each of the 15 scales in at least one vignette. This demonstrates that the full range of possible scores were used in these vignettes and would contribute to the interrater reliability estimate.
Interrater reliability was assessed by quadratic weighted kappa (κw) estimates (Table 2). The COSMIN standard for acceptable interrater reliability (κw ≥ 0.7)Reference Prinsen, Mokkink, Bouter, Alonso, Patrick and de Vet31 was exceeded by 10 of the 15 scales and by the total score. From Table 2, it can be seen that scales 7 and 15 were within 0.01 of the standard. Scales 11 and 14 were within 0.08 of the standard. The confidence intervals for those four scales are wide and overlap the standard. Scale 2 had a very wide confidence interval and was clearly lower than the standard.
Table 2 Interrater reliability quadratic weighted kappa estimates for vignettes
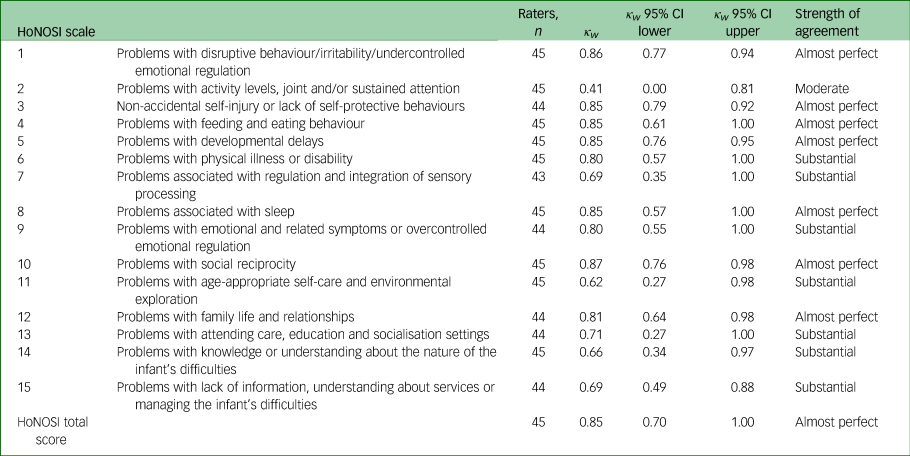
HoNOSI, Health of the Nation Outcome Scales for Infants.
The Landis and Koch Strength of Agreement criteriaReference Landis and Koch35 is shown in the rightmost column. Scale 2 (activity/attention) is only Moderate in agreement (0.41–0.60). However, seven of the scales and the total score have Almost Perfect agreement (0.81–1.00), whereas the remaining seven have Substantial agreement (0.61–0.80).
Discussion
This study was designed to test the interrater reliability of the HoNOSI. Results show that the level of interrater reliability for the total score was Almost Perfect when measured against the benchmarks outlined by Landis and KochReference Landis and Koch35 and that it also well exceeds the COSMIN standard for interrater reliability.Reference Mokkink, Prinsen, Patrick, Alonso, Bouter and de Vet32 The majority of individual scales clearly met the COSMIN criteria and applying the commonly used Landis and KochReference Landis and Koch35 descriptors, seven scales and the total score had Almost Perfect agreement and seven scales had Substantial agreement between raters.
COSMIN guidelines describe what constitutes a sufficient level of agreement. Using the COSMIN criteria for good measurement properties, the results of the present study well exceed the criteria for interrater reliability, where reliability is rated as either sufficient (κw ≥ 0.7), insufficient (κw < 0.7) or indeterminate (where κw is not reported. Scales 7 (problems associated with regulation and integration of sensory processing), 11 (problems with age-appropriate self-care and environmental exploration), 14 (problems with knowledge or understanding about the nature of the infant's difficulties) and 15 (problems with lack of information, understanding about services or managing the infant's difficulties) were classed as insufficient in terms of reliability (Table 2), although they are close to the arbitrary cut-off (κw ≥ 0.7).
It is only scale 2 (Problems with activity levels, joint and/or sustained attention), with κw < 0.5, that was found to be insufficient according to the COSMIN criteria, although assessed as a moderate level of agreement according to the guidelines provided by Landis and Koch.Reference Landis and Koch35 Aside from scale 2, the other 14 HoNOSI scales and the total score showed a reasonable amount of variability between vignettes. The study had sufficient power to test the null hypothesis at the interrater reliability estimate of 0.5.
The HoNOSI has links with the HoNOS family of measures, especially the HoNOSCA.Reference Gowers, Harrington, Whitton, Lelliott, Beevor and Wing11 The HoNOSI estimates are stronger than those obtained with those measures.Reference Hanssen-Bauer, Gowers, Aalen, Bilenberg, Brann and Garralda13,Reference Pirkis, Burgess, Kirk, Dodson, Coombs and Williamson15 Although the HoNOSCA covers different developmental stages in its use across ages 4–18 years, the HoNOSI, with a much a narrower age range, covers developmental shifts of arguably greater magnitude. Although the interrater reliability was Substantial to Almost Perfect for the majority of the scales and the total score, it would be wise to establish whether this overall acceptable estimate hides less acceptable interrater reliability for different age groups. The lower estimate for attention may reflect a differential functioning of the scale for different age groups. It is possible that the scale can be applied very reliably for 9-month-olds and 3-year-olds, but less so for 18-month-olds.
Vignettes have been found to be a valid tool when measuring the quality of clinical practice.Reference Peabody, Luck, Glassman, Jain, Hansen and Spell36 They remain a key method when wanting to ensure that raters are exposed to exactly the same stimuli. However, vignettes are not the same as clinical practice, and the HoNOSI may perform better or worse with real cases. Although the vignettes covered ages from 4 months to 4 years, there were only five presentations assessed. The middle age group was not covered. Evaluating the HoNOSI in routine clinical practice would supplement the vignette approach by ensuring that a greater range of presentations could be examined. Furthermore, the question of whether the HoNOSI has differing reliability between, for example, infants and pre-schoolers, could be examined with larger sampling.
It is anticipated that future research could explore HoNOSI psychometric properties with respect to other domains and consumer attributes, including the specific nature of presenting problems, diagnostic categories and developmental differences. With regard to the rapid maturation that occurs in this age range, conceptualising and assessing test–retest reliability will be an important task. A face validity study25 and concurrent validity field trialReference Brann, Culjak, Kowalenko, Dickson, Coombs and Burgess26 have now been completed. There are other psychometric properties (e.g. sensitivity to change) yet to be investigated. However, the interrater reliability findings are sufficiently encouraging to support the further exploration of the HoNOSI. The HoNOSI is promising, and the very young have been excluded from the routine outcome measurement framework for too long. Whether it proves to be useful in this endeavour requires further exploration of reliability, validity and feasibility and this may be best achieved by examination in routine clinical practice.
A final caveat: if the HoNOSI continues to demonstrate good enough psychometric properties in future research, it will still share one common feature with other routine outcome measures. Measured change cannot specify the cause of the change. The HoNOSI, HoNOSCA and similar measures identify change but do not independently specify whether this is clearly maturational, treatment-initiated or a result of alteration in the child's environment. Understanding the source of any change, positive or negative, remains the clinical task at an individual level and a research and policy task at the aggregate level. Hopefully, the HoNOSI will facilitate routine dialogue about mental health outcomes for our relatively overlooked infants and pre-schoolers.
Data availability
The data that support the findings of this study are available from the corresponding author, G.C., upon reasonable request.
Author contributions
All authors contributed to the conception and design of the study. P. Burgess conducted the analysis. G.C. prepared the final manuscript. All authors reviewed and approved the final version of the manuscript.
Funding
The study was undertaken by the Child and Adolescent Mental Health Information Development Expert Advisory Panel (CAMHIDEAP), supported by the Australian Mental Health Outcomes and Classification Network (AMHOCN). CAMHIDEAP and AMHOCN have been funded by the Australian Department of Health through a contract with the Health Education and Training Institute.
Declaration of interest
None.
Appendix 1: Health of the Nation Outcome Scales for Infants (HoNOSI) – list of scales



 Open access
Open access
eLetters
No eLetters have been published for this article.