



Hoarding disorder is a highly debilitating psychiatric illness that poses a profound public health burden.1, Reference Tolin, Frost, Steketee, Gray and Fitch2 Up to 25% of deaths by house fire are attributable to hoarding,Reference Harris3 and hoarding-related clutter in homes increases fall risk, health code violations and difficulty with self-care, especially among older adults, who are disproportionately affected.Reference Tolin, Frost, Steketee, Gray and Fitch2, Reference Frost, Steketee and Williams4–Reference Ayers, Saxena, Golshan and Wetherell7 Over 50% of individuals with hoarding disorder have co-occurring depression or a chronic anxiety disorder.Reference Frost, Steketee and Tolin8 Executive dysfunction, particularly impairments in visual categorisation, learning and memory, is a prominent feature of hoarding disorder and may also affect functioning (summarised in Mackin et al Reference Mackin, Vigil, Insel, Kivowitz, Kupferman and Hough9).
Treatment for hoarding disorder
Effective treatment options for hoarding disorder are limited. Although there is a role for pharmacological treatment,Reference Brakoulias, Eslick and Starcevic10 the current standard of care based on the published evidence is cognitive–behavioural therapy (CBT), which varies in implementation (e.g. number of sessions, individual versus group, inclusion of home visits) and is dependent on access to trained mental health providers.Reference Tolin, Frost, Steketee and Muroff11, Reference Williams and Viscusi12 Currently published studies are small (range 6–58 participants), and suggest that with CBT, hoarding symptoms improve by 20–30% on average (range 12–37%) (see Mathews et al Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13 and Tolin et al Reference Tolin, Frost, Steketee and Muroff11). A recent meta-analysis indicates that individual and group CBT are similarly effective;Reference Tolin, Frost, Steketee and Muroff11 however, by definition, group CBT allows for the treatment of more individuals within a given timeframe, making it the preferable choice when access to treatment providers is limited.
Because clinician-delivered CBT tailored for hoarding disorder is not widely available,Reference Muroff, Steketee, Himle and Frost14 additional treatment options are needed, and factors such as lack of recognition of hoarding disorder as a medical (psychiatric) condition, poor insight into illness, stigma and shame may make community-based approaches an inviting alternative.Reference Koenig, Leiste, Spano and Chapin15 Of the few previously studied alternatives, group peer-facilitated therapy (G-PFT) with a CBT-based workbook appears to be the most effective, with improvement rates similar to group psychiatrist-led CBT (G-CBT) (summarised in Mathews et al Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13). However, to date, no prospective, randomised clinical trials directly comparing G-PFT with G-CBT have been published.
Predictors of treatment response
In addition, studies examining predictors of treatment response have been limited to a few demographic and clinical variables (e.g. gender, less severe pre-treatment hoarding severity, co-occurring anxiety or depressive symptoms and in one study, treatment adherence).Reference Tolin, Frost, Steketee and Muroff11, Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13, Reference Muroff, Steketee, Frost and Tolin16 None of the variables examined in previous studies were consistently found to predict treatment outcome. Given its chronic nature and high degree of functional impairment,Reference Tolin, Frost, Steketee, Gray and Fitch2 there continues to be a pressing need to identify predictors of treatment response for hoarding disorder. Such predictors might include, in addition to demographic factors, clinical variables such as neurocognitive function and psychiatric status, and treatment-related factors such as treatment adherence.
This study was a randomised, controlled non-inferiority trial aimed at formally evaluating the effectiveness of G-CBT and G-PFT and identifying predictors of treatment response. We hypothesised that G-CBT and G-PFT would be similarly effective and that both would lead to clinically meaningful improvement, as well as that individual characteristics (e.g. age, psychiatric symptoms and pre-treatment cognitive function including visual learning, memory and sustained attention) and treatment adherence would be associated with treatment response.Reference Mackin, Vigil, Insel, Kivowitz, Kupferman and Hough9
Method
Study procedures
The study took place at the University of California, San Francisco and the Mental Health Association of San Francisco. It was approved by the University of California, San Francisco Institutional Review Board (#13-12100), and was prospectively registered at Clinicaltrials.gov (trial registration identifier: NCT02040805). Study procedures, which were designed to maximise generalisability and to be implemented by community agencies and individuals in a real-world setting, are described below and in the Supplementary Methods, available at https://doi.org/10.1192/bjo.2018.30. Further details about the academic/community collaborative partnership and study design have previously been published.Reference Uhm, Tsoh, Mackin, Gause, Chan and Franklin17
Recruitment and screening
Participants were recruited through advertisements, mental health clinics and senior centres throughout the San Francisco Bay Area, and through outreach by the Mental Health Association of San Francisco. Potential participants gave verbal consent and were screened for hoarding symptoms via telephone and online self-report questionnaires. To increase specificity of these measures in identifying hoarding disorder, two or more of the following were required for inclusion: Saving Inventory, Revised (SI-R) score of ≥42,Reference Frost, Steketee and Grisham18 University of California, Los Angeles Hoarding Symptom Scale (UHSS) score of ≥20Reference Saxena, Ayers, Dozier and Maidment19 and Clutter Image Rating Scale score of ≥12.Reference Frost, Steketee, Tolin and Renaud20 Those who met screening criteria subsequently provided written informed consent for all ensuing study procedures. All pre-treatment assessments were completed before randomisation. Eligible participants were stratified by gender and randomised by computer in a 1:1 ratio in blocks of five, to either G-CBT or G-PFT, by a member of the research team who was blind to clinical status.Reference Uhm, Tsoh, Mackin, Gause, Chan and Franklin17
Clinical interviews were completed at baseline only, and neuropsychological assessments and self-report questionnaires (Supplementary Methods and Supplementary Table 1) were completed pre- and post-treatment.Reference Uhm, Tsoh, Mackin, Gause, Chan and Franklin17 Group facilitators were blinded to the neurocognitive and psychiatric status of participants, other than the required diagnosis of hoarding disorder.
Participants were financially compensated for completing the assessments, although they were not compensated for participating in the treatment groups. As a post hoc follow-up, symptom severity and functional assessment were also re-assessed in randomised individuals who agreed to re-contact at least 3 months (range 3–25 months) after the end of their assigned treatment groups (longitudinal assessment) (Supplementary Methods).
Inclusion/exclusion criteria
To maximise generalisability, inclusion criteria were deliberately broad. Individuals were eligible for participation if they met the screening criteria listed above and DSM-5 criteria for hoarding disorder,1 assessed with the Structured Interview for Hoarding Disorder.Reference Nordsletten, de la Cruz, Pertusa, Reichenberg, Hotopf and Hatch21 Participants were excluded if they had known intellectual disability, moderate to severe dementia (scores of ≤17 on the Montreal Cognitive AssessmentReference Nasreddine, Phillips, Bedirian, Charbonneau, Whitehead and Collin22), were unable to actively participate in treatment (e.g. because of acute medical conditions, high suicide risk or actively disruptive psychotic or behavioural symptoms) or had received individual or group CBT or peer-facilitated therapy for hoarding in the previous year. Concurrent participation in other forms of treatment (e.g. medication management, Clutterers' Anonymous, psychotherapy for non-hoarding symptoms) was allowed and was tracked during the course of treatment. Participants were not excluded based on co-occurring psychiatric illness, active substance use, psychosis or suicidal ideation (unless, as noted, they were actively disruptive or deemed to be at high risk of suicide).
Interventions
The interventions were based on published manualised treatments for hoarding disorderReference Steketee and Frost23–Reference Shuer and Frost26 and modified for this study based on input from our community partners (Supplementary Methods and Uhm et al Reference Uhm, Tsoh, Mackin, Gause, Chan and Franklin17). Groups were composed of 8–12 participants. G-CBT groups met weekly for 16 sessions over 20 weeks and were led by postdoctoral-level psychologists. Two 30-minute home visits were conducted in the G-CBT group, one after week 3 and the other after week 15. G-CBT participants were assigned (but not required to accept) clutter buddies (individuals who were available to provide encouragement and maintain accountability for treatment adherence) from within the group. G-PFT groups met weekly for 15 sessions over 20 weeks and were led by trained peer facilitators who had lived experience of hoarding. G-PFT participants did not receive home visits and were encouraged to identify (but were not assigned) clutter buddies. Peer facilitators checked in with each group member by telephone between each session.
Assessments
The primary outcome was hoarding symptom severity, assessed by the SI-R,Reference Frost, Steketee and Grisham18 with hoarding-related functional impairment as a secondary outcome, assessed by the Activities of Daily Living Scale in Hoarding Disorder (ADL-H).Reference Frost, Hristova, Steketee and Tolin27 Hoarding-related beliefs were assessed by the Saving Cognition Inventory.Reference Steketee, Frost and Kyrios28 Symptoms of depression, anxiety and attention-deficit hyperactivity disorder were assessed by the Beck Depression Inventory, Second Edition,Reference Beck, Steer, Ball and Ranieri29 the Beck Anxiety InventoryReference Beck, Epstein, Brown and Steer30 and the Swanson, Nolan, and Pelham Rating Scale,Reference Swanson, Schuck, Mann, Carlson, Hartman and Sergeant31 respectively.
Neurocognition was assessed by standard neuropsychological measures, which are detailed in the Supplementary Methods. Neurocognitive domains of particular interest included sustained visual attention (Conners’ Continuous Performance Test IIReference Conners32), visual memory and learning (Brief Visuospatial Memory Test, Revised)Reference Benedict33) and visual spatial processing and problem solving (Block Design subtest of the Wechsler Adult Intelligence ScaleReference Wechsler34). For all measures, scaled scores were used in the analyses.
Treatment-related measures
Beliefs about treatment and treatment preferences were assessed with questions developed for this study (Supplementary Fig. 1). Homework completion was assessed weekly and a group evaluation (Supplementary Figs 2 and 3) was completed bi-weekly throughout treatment. Continuing support after the end of treatment was assessed at the longitudinal evaluation (Supplementary Fig. 4).
Analyses
All analyses were conducted with SAS software version 9.4. Standard methods were used to summarise and describe the collected data, including the number who met the criteria for clinically significant change (SI-R change ≥14 points)Reference Frost, Ruby and Shuer35, Reference Gilliam, Norberg, Villavicencio, Morrison, Hannan and Tolin36 and functional remission (SI-R reduction ≥14 points and post-test SI-R of <42).Reference Gilliam, Norberg, Villavicencio, Morrison, Hannan and Tolin36, Reference Frost and Hristova37 All participants who provided baseline data, whether or not they completed the treatment, were eligible for inclusion, although only participants with complete outcome data for any given measure were included in the analyses for that measure.
Treatment drop-outs were defined as individuals who completed fewer than 60% of the sessions. To test for evidence of effects of non-completion, we re-estimated and tested our models of non-inferiority and predictors of treatment response, using only participants who completed treatment (completers-only analysis). In a similar way, sensitivity analyses were conducted to examine the effects of including/excluding participants who dropped out of treatment before the third session and later re-joined a group (n = 12). Post-treatment assessments were obtained, when possible, on all participants, and particularly for individuals who attended at least one group.
A one-tailed t-test for non-inferiority comparing the mean post-treatment SI-R scores between G-PFT and G-CBT groups, with a margin of equivalence of 5 points, was used. This margin represents half of the minimal change score that was determined to represent noticeable and meaningful improvement from a patient and healthcare provider's perspective (SI-R change ≥10 points or 15% improvement from a mean SI-R baseline of 65) (R. Frost, personal communication, 2013, and based on our prior work).Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13 The margin was set at 2.5 for the ADL-H, using a similar approach (e.g. 15% improvement from baseline total score divided by two). Effect sizes for the SI-R and ADL-H were computed as mean change divided by the s.d. of the change. The change in SI-R and ADL-H scores by treatment group over time (pre-treatment, post-treatment and longitudinal) was examined by linear mixed models. Testing for individual characteristics that were associated with treatment response was conducted by regression models of change in SI-R scores, incorporating each individual measure (e.g. insurance status, socioeconomic, demographic, clinical and neuropsychological factors) as a covariate. Variables that were associated with SI-R change at P ≤ 0.15 were carried forward into multivariable models.
Results
Pre-treatment characteristics
Recruitment occurred from April 2014 to January 2016. A total of 632 individuals expressed interest in the study; 414 were clinically assessed and 323 were randomised into G-CBT or G-PFT (Fig. 1). Only 13% of screened individuals and 3% of those clinically assessed were excluded; the remainder declined to participate or were lost to follow-up. Individuals who were screened but not randomised (n = 149) had lower mean hoarding severity scores, poorer insight and were more likely to be male than those who were randomised to treatment (Supplementary Table 2).
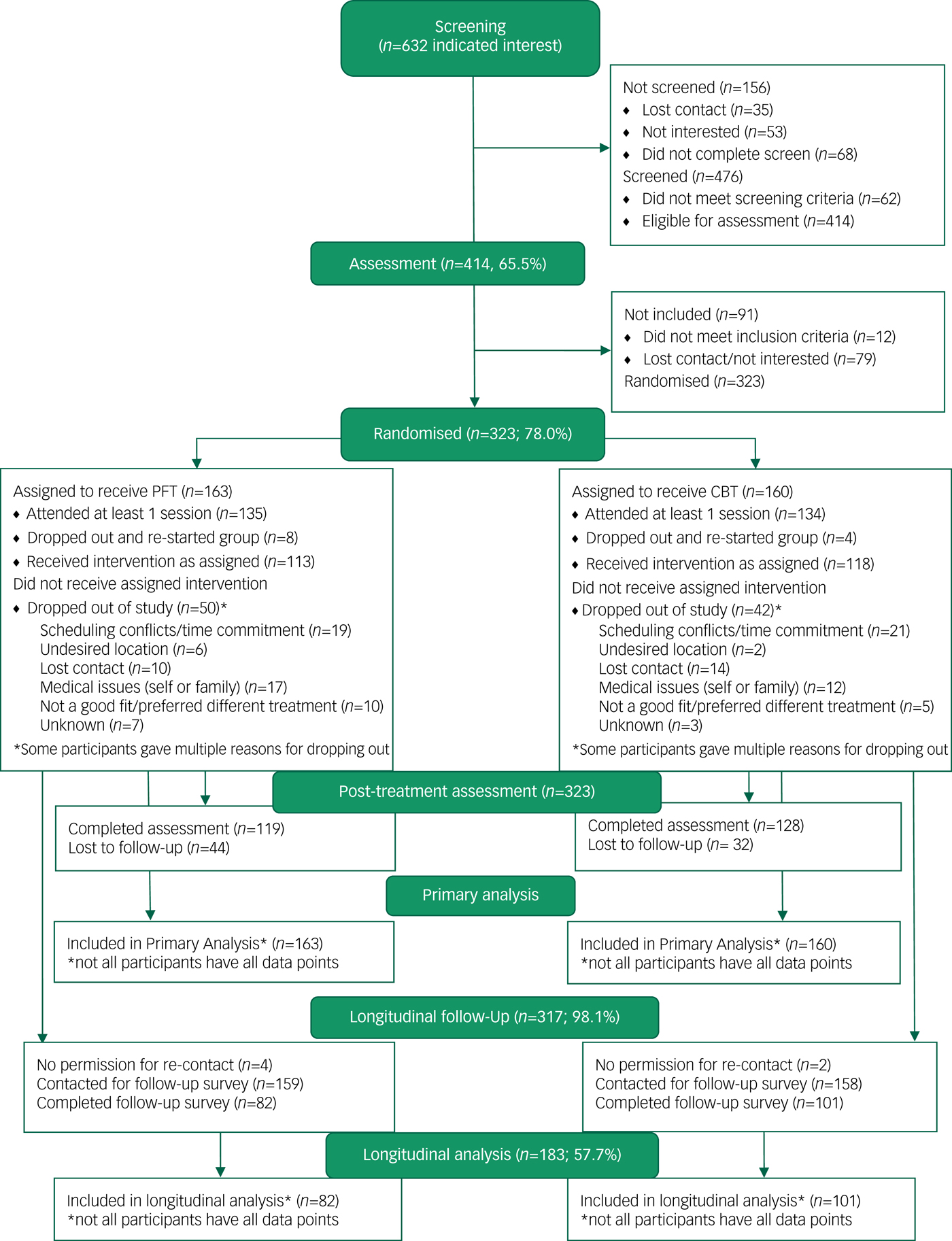
Fig. 1 Study flow diagram. CBT, cognitive–behavioural therapy; PFT, peer-facilitated therapy.
There were no significant differences in baseline characteristics between participants randomised to G-CBT or G-PFT (Table 1). The majority of the sample were female (74.5%), with mean age of 59 years (range 18–89). The ethnic-racial composition was diverse, comprising 59.5% White, 11.3% Asian, 7.6% Black, 1.2% Native American, Native Hawaiian or Pacific Islander and 20.4% multi-racial or other. Further, 9.3% participants reported as Hispanic.
Table 1 Baseline characteristics for G-CBT and G-PFT groups
ADL-H, Activities of Daily Living Scale in Hoarding Disorder; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; CI-R, Clutter Image Rating Scale; G-CBT, group psychiatrist-led cognitive–behavioural therapy; G-PFT, group peer-facilitated therapy; LGBT, lesbian, gay, bisexual and transgender community; MoCA, Montreal Cognitive Assessment; NART, National Adult Reading Test Full Scale IQ; SCI, Saving Cognition Inventory; SI-R, Saving Inventory, Revised; SNAP-IV, Swanson, Nolan and Pelham attention-deficit hyperactivity disorder Rating Scale; UHSS, University of California, Los Angeles Hoarding Severity Scale.
a. One participant in each group reported their gender as other.
b. MoCA data available for 60 participants in the G-CBT group and 80 participants in the G-PFT group.
Participants had moderately severe hoarding, depression and anxiety symptoms at baseline (Table 1). More than half had a current or lifetime history of an additional psychiatric disorder, most commonly major depressive disorder (44.8%) and anxiety disorders (30.5%). Approximately 10% had a moderate to high suicide risk. Most (72%) expressed no strong preference for either treatment. Only one of the ten participants who preferred G-PFT was randomised to G-CBT, whereas 36 out of 77 participants who preferred G-CBT were randomised to G-PFT (χ 2 = 6.72, d.f. = 2, P = 0.04).
Participation in treatment
Of the 323 individuals randomised to treatment, 269 (83%) attended at least one session and 231 (71.5%) completed treatment. There were no significant differences in drop-out rates between G-CBT and G-PFT groups (Fig. 1). Session attendance (per cent of total groups attended) was higher in the G-CBT group (73.3%) than G-PFT group (57.7%) (t = −4.09, d.f. = 245, P < 0.0001), whereas homework completion was similar between groups (54.3% of G-CBT participants and 48.9% of G-PFT participants, t = −1.50, d.f. = 245, P = 0.13). A total of 69% of G-CBT participants and 37% of G-PFT participants had a clutter buddy (χ 2 = 33.11, d.f. = 1, P < 0.0001). Most participants with a clutter buddy (82.5% of G-CBT participants and 83.8% of G-PFT participants) found them to be helpful (χ 2 = 0.03, d.f. = 1, P = 0.86).
Treatment outcomes
Hoarding severity
Post-treatment data were available for 247 individuals (231 treatment-completers; 16 non-completers). G-CBT participants had a 27.7% reduction in SI-R scores (mean post-treatment score 45.9, s.d. = 15.0), whereas G-PFT participants had a 25.6% reduction in SI-R scores (mean post-treatment score 47.8, s.d. = 14.6) (Table 2). The test of non-inferiority indicated that the null hypothesis (i.e. that G-PFT outcomes would be statistically worse than G-CBT outcomes) was rejected (between-group difference 1.82 points, one-sided 95% CI 4.89, t = −1.71, d.f. = 245, P = 0.04), indicating that G-PFT was as effective as G-CBT. A total of 37% of G-CBT and 36% of G-PFT participants had post-treatment SI-R scores of <42, and 55% of G-CBT and 57% of G-PFT participants had ≥14-point reduction in SI-R scores pre- to post-treatment. There was no significant difference in the number of participants who achieved remission (32.8% of G-CBT participants and 29.4% of G-PFT participants, χ 2 = 0.33, d.f. = 1, P = 0.56). There were no differences when treatment-completers only were analysed (data not shown).
Table 2 Pre-treatment, post-treatment and longitudinal scores for G-CBT and G-PFT groups

All numbers are for all participants who were randomised to treatment with one exception: the SI-R results are reported both for all participants and for those who completed treatment. Treatment-completers N = 118 for the G-CBT group and N = 113 for the G-PFT group.
ADL-H, Activities of Daily Living Scale in Hoarding Disorder; BAI, Beck Anxiety Inventory; BDI, Beck Depression Inventory; CI-R, Clutter Image Rating Scale; G-CBT, group psychiatrist-led cognitive–behavioural therapy; G-PFT, group peer-facilitated therapy; N/A, not available; SCI, Saving Cognition Inventory; SI-R, Saving Inventory, Revised.
Functional impairment
The G-CBT group had a 10.5% reduction in ADL-H scores pre- to post-treatment (mean post-treatment score 25.5, s.d. = 10.1), whereas the G-PFT group had a 12.4% reduction in ADL-H scores (mean post-treatment score 26.1, s.d. = 8.7) (Table 2). The test of non-inferiority was significant (between-group difference 1.82 points, one-sided 95% CI 2.67, t = −1.52, d.f. = 245, P = 0.05), again indicating equivalence between the groups.
Predictors of treatment response
Predictors of treatment response were examined at post-treatment only; the longitudinal assessment was not included in this analysis. Variables that were associated with change in either SI-R or ADL-H scores at a P-value of ≤0.15 were included in multivariable models (Supplementary Tables 3 and 4). For highly correlated variables, only the most strongly associated in the univariate analyses were included. In the univariable models, more severe pre-treatment severity and hoarding-related thoughts and beliefs were associated with treatment improvement and more severe anxiety and/or depression were associated with less improvement in both groups (Supplementary Tables 3 and 4). Higher rates of homework completion were associated with improvement for both treatment groups; higher group attendance and finding a clutter buddy helpful were associated with treatment improvement for G-PFT but not G-CBT participants.
The multivariable models for SI-R change included pre-treatment hoarding (assessed with UHSS total score rather than SI-R total score, to avoid circularity), depressive, anxiety and attention-deficit hyperactivity disorder symptoms, hoarding cognitions, mean number of psychiatric diagnoses, homework adherence, group attendance, finding a clutter buddy helpful and treatment preference. The multivariable models for both G-CBT and G-PFT groups accounted for only a small amount of the total variance (adjusted R 2 = 0.08, f(9,115) = 2.17, P = 0.03 for the G-CBT group; adjusted R 2 = 0.05, f(9,103) = 1.59, P = 0.13 for the G-PFT group). For both conditions, pre-treatment UHSS score was the only independent predictor of treatment outcome (β = 0.73, s.e. = 0.29, t = 2.56, d.f. = 1, P = 0.01 for the G-CBT group; β = 0.65, s.e. = 0.29, t = 2.26, d.f. = 1, P = 0.03 for the G-PFT group); higher pre-treatment severity was associated with greater improvement. For the G-PFT but not for the G-CBT group, lower pre-treatment depressive symptoms (β = −0.28, s.e. = 0.15, t = −1.89, d.f. = 1, P = 0.06) indicated a trend for association with improvement. These results did not change when the analyses were repeated in treatment-completers only (data not shown).
Continuing treatment and maintenance of treatment gains
We obtained longitudinal follow-up data ≥3 months post-treatment on 183 of the 323 randomised participants (101 in the G-CBT group and 82 in the G-PFT group). The average time to follow-up was 14.4 months (s.d. = 6.5, range 3–25). Most participants (64%) were re-contacted >1 year after completing treatment. Participants who provided longitudinal data were more likely to be women (χ 2 = 9.3, d.f. = 1, P = 0.002), White (χ 2 = 11.8, d.f. = 1, P = 0.001) and have higher education levels (t = −3.6, d.f. = 182, P = 0.0004) than those who did not. There were no significant differences in pre- or post-treatment SI-R scores between those who provided longitudinal data and those who did not. There were no differences in time to follow-up between groups (G-CBT group: 13.9 months, s.d. = 7.2; G-PFT group: 13.2 months, s.d. = 6.9; t = −0.68, d.f. = 182, P = 0.50).
The linear mixed models analysis incorporating treatment group (G-CBT and G-PFT) and time (pre-treatment, post-treatment and longitudinal) was significant for both SI-R (likelihood ratio χ 2 = 115.5, d.f. = 1, P < 0.0001) and ADL-H (LR χ 2 = 162.1, d.f. = 1, P < 0.0001). For both outcomes, only time significantly contributed to the model (SI-R: f = 250.5, d.f. = 2, P < 0.0001; ADL-H: f = 34.3, d.f. = 2, P < 0.0001); there were no significant differences between G-CBT and G-PFT groups at any time point (Tables 1 and 2). There were no significant differences between SI-R scores immediately post-treatment and at longitudinal follow-up (mean difference −0.45, s.d. = 12.7, t = −0.45, d.f. = 182, P = 0.66), indicating that the treatment gains were generally maintained at 3 months post-treatment or later (Fig. 2). However, mean ADL-H scores were higher at follow-up than post-treatment (difference −2.2, s.d. = 10.5, t = –2.68, d.f. = 182, P = 0.008), indicating that gains in function were not as well sustained. Longer time from post-treatment to longitudinal follow-up was associated with worsening SI-R (r = −0.173, P = 0.03) and ADL-H (r = −0.240, P = 0.01) scores. Higher rates of homework completion were associated with better (lower) longitudinal SI-R scores (β = 10.21, s.e. = 3.66, t = 2.79, d.f. = 1, P = 0.006).
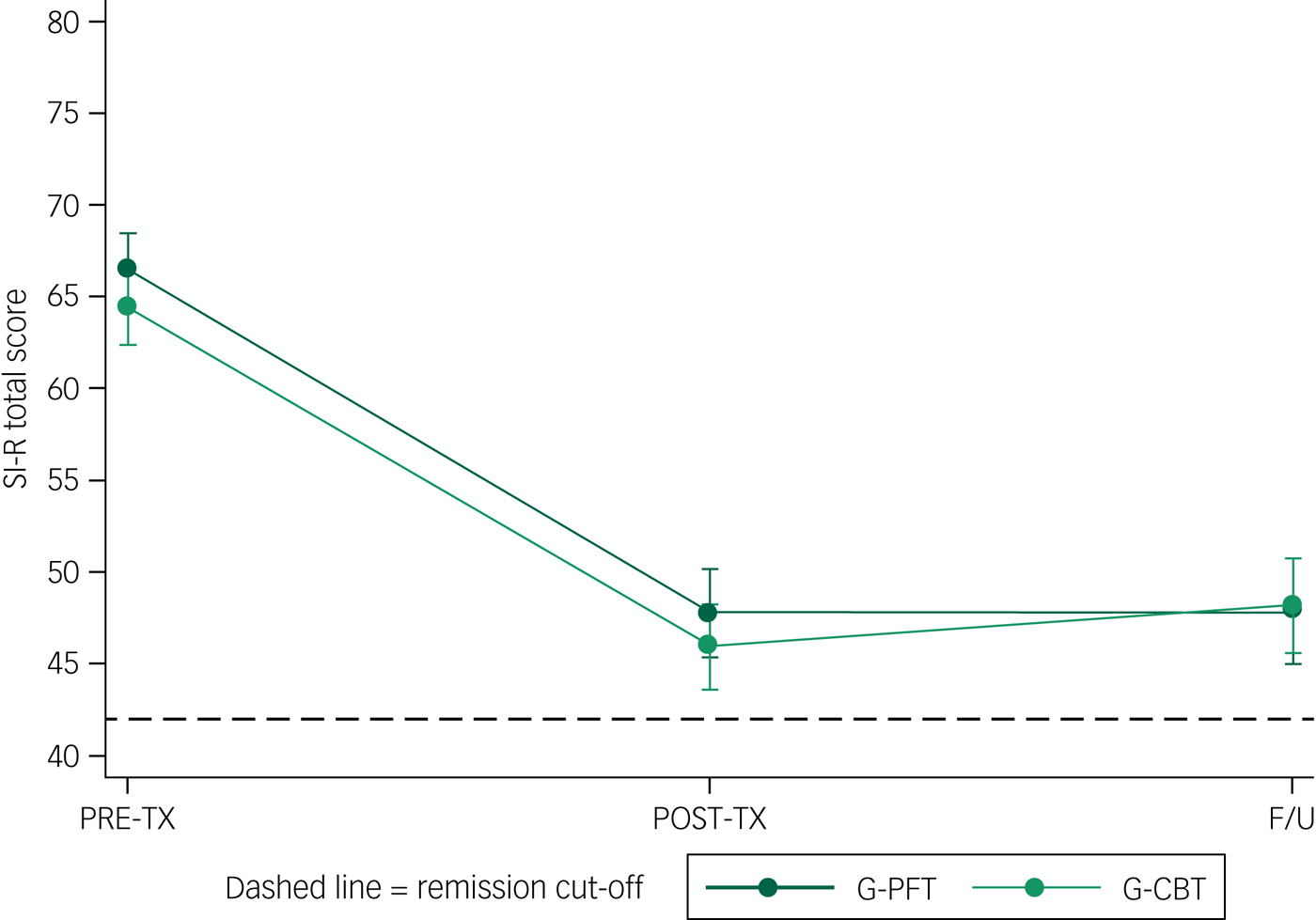
Fig. 2 Hoarding symptom severity scores (SI-R total score) before (PRE-TX), immediately after (POST-TX) and at least 3 months after treatment (longitudinal follow-up, F/U). Dashed line indicates remission cut-off (SI-R < 42). G-CBT, group psychiatrist-led cognitive–behavioural therapy; G-PFT, group peer-facilitated therapy; SI-R, Savings Inventory, Revised.
The remission rate for the longitudinal follow-up was 32.8% for the G-CBT group and 29.4% for the G-PFT group (χ 2 = 0.33, d.f. = 1, P = 0.56). There were no statistically significant differences between those who remitted and those who did not, for gender, age, pre-treatment hoarding severity or cognitions, psychiatric comorbidity, treatment completion, group attendance rates or homework completion rates (data not shown). A total of 28 of the 54 participants who achieved remission at post-treatment no longer met remission criteria at longitudinal follow-up, whereas 24 of the 109 participants who did not meet criteria for remission at post-treatment did meet these criteria at longitudinal follow-up.
Of the 176 participants who provided data about ongoing support after treatment, 71.2% continued to receive either formal or informal help for hoarding after the treatments ended. Of these, 71% remained in contact with members of their treatment group, 31% remained in contact with their clutter buddies, 23% attended hoarding support groups (including drop-in groups), 17.5% received formal treatment for hoarding disorder(e.g. by a psychiatrist or psychologist) and 5% had worked with a professional organiser. Further, 38% continued to receive help with hoarding from family and/or friends. Of the 87 who remained in contact with a clutter buddy or treatment group member, or received help from a support group or professional, 83 (95.4%) were still in contact or receiving help from these sources at least 3 months after treatment. There were no significant differences in time to longitudinal follow-up between those who were still in contact or receiving help at longitudinal follow-up and those who were not (t = 1.008, d.f. = 182, P = 0.32).
Of those who continued to receive support with hoarding behaviours post-treatment, only ongoing help from family and/or friends was significantly associated with maintenance of gains. Individuals who received such help had mean longitudinal SI-R scores of 43.9 (s.d. = 13.3), whereas those who did not had mean scores of 50.2 (s.d. = 4.7; t = 2.89, d.f. = 175, P = 0.004, N = 177). A total of 48% of those who met remission criteria at post-treatment and ≥3 months later and 61.8% of those who remitted only at longitudinal follow-up, compared with 26% of those who did not meet criteria for remission at either time point and 21.3% of those who met remission criteria only at post-treatment, received help from family and friends (χ 2 = 12.63, d.f. = 3, P = 0.006). No other post-treatment interventions were associated with treatment-response patterns.
Discussion
In this randomised clinical trial of 323 treatment-seeking individuals with hoarding disorder, G-PFT was as effective as G-CBT in reducing hoarding symptom severity, and treatment gains were maintained for at least 3 months. Although effective, the availability of trained mental health professionals who can provide CBT for hoarding disorder is limited,Reference Muroff, Steketee, Himle and Frost14 and access to care remains a substantial impediment for many individuals and families. Previous small studies have demonstrated the efficacy of peer-facilitated treatment under idealised conditions,Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13, Reference Frost, Ruby and Shuer35, Reference Frost, Pekareva-Kochergina and Maxner38 but this study is the first, and to our knowledge, the only randomised clinical trial to directly compare peer-facilitated treatment to clinician-led treatment. Our finding that community-based peer-facilitated groups were as effective in treating hoarding disorder as groups led by trained mental health professionals represents a potential paradigm shift, and has important implications for treatment providers, for individuals with hoarding disorder and their families, and for policymakers.
The sample size, which is five times larger than the largest previously published CBT study,Reference Tolin, Frost, Steketee and Muroff11, Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13 the racial, ethnic, and sociodemographic diversity of the sample, and the study protocol, which was deliberately designed with our community partners to make the implementation of treatment feasible by providers in a community-based practice setting, maximises our confidence in the robustness and generalisability of the findings. Although there was a risk of decreasing treatment response, as we had comparatively few sessions (15 or 16, compared with a previously published range of 13–35), large group sizes (8–12, compared with a previously published range of 6–8), few or no home visits and somewhat less intensive clinician/facilitator training than has been reported previously,Reference Tolin, Frost, Steketee and Muroff11, Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13 this balance between optimising feasibility and treatment outcomes appears to have paid off. The 25–30% improvement in hoarding symptom severity is consistent with what has been previously reported,Reference Tolin, Frost, Steketee and Muroff11, Reference Mathews, Uhm, Chan, Gause, Franklin and Plumadore13 and was similar across treatment types, despite differences in treatment protocols.Reference Steketee and Frost23–Reference Shuer and Frost26 Although there is still a long way to go in optimising treatment for hoarding disorder, as only one-third of participants achieved symptomatic remission, over 50% had a clinically significant treatment response (≥14 point improvement), suggesting that most individuals received noticeable benefit from treatment.
Predictors of treatment outcome
Contrary to our hypothesis, the only participant-related variable that consistently independently predicted treatment response in multivariable analyses was more severe hoarding symptoms at baseline. In particular, psychiatric symptoms/diagnoses and neurocognitive status were not predictive of treatment outcome, nor were treatment preferences or beliefs about treatment. In fact, the majority of individuals expressed no strong preference for one type of treatment over another. Similarly, there were no treatment-related variables that independently predicted differential responses to G-CBT or G-PFT in multivariable models. Of interest, however, for the G-PFT but not G-CBT group, higher percentage of homework completed, finding a clutter buddy helpful and mean percentage of groups attended were all associated with treatment improvement in univariable analyses. Similarly, receiving ongoing help from family and friends post-treatment was associated with maintenance of treatment gains at ≥3 months of follow-up. Although possibly discouraging from a precision medicine perspective, which aims to tailor appropriate interventions for individuals based on specific characteristics, these findings reinforce the importance of identifying ways to improve treatment adherence and promote ongoing community engagement (both during and after treatment) to maximise effectiveness and promote ongoing maintenance of gains for this chronic disorder.
Limitations
The primary limitation in this study was loss to follow-up. As has been seen in other studies, approximately 30% of participants dropped out of treatment before completion; we obtained post-treatment data on only 16% of drop-outs. Similarly, the longitudinal follow-up was post hoc rather than being planned before study initiation. As a result, participants were assessed at varying time points after treatment, and we obtained follow-up data on only 55% of randomised participants, with substantial differences between treatment groups (n = 82 for the G-PFT group and n = 101 for the G-CBT group).
As with many studies, as participants typically sought out the hoarding treatment, participants in our study may have had a higher awareness of their disorder than those who did not seek out treatment. Individuals who were screened but did not seek treatment had milder hoarding disorder symptoms and/or less insight into their illness, and therefore may not have seen it as problematic, as has been posited in other hoarding disorder-related research.Reference Grisham and Norberg39, Reference Mataix-Cols and Pertusa40 Despite our diverse recruitment approaches, most of the participants in the study were female, as has also been seen in previous studies.Reference Tolin, Frost, Steketee and Muroff11
There were also potential limitations to the study design. First, the outcome variables were dependent on self-report measures rather than objective observations. Second, we made several modifications to the published manuals to fit the needs of our intended population and treatment providers, and did not formally assess treatment fidelity. These changes represent a potential weakness of the study, but also a potential strength. For example, although treatment fidelity may not have been as rigorous as in a more controlled trial, a departure from treatment fidelity not only mimics what might happen in a real-world setting, and thus increases generalisability, but would also tend to bias our results toward the null. As the degree of improvement under the protocol described here was similar to what has been previously reported, and the two treatment types did not significantly differ in outcomes despite the departures from previously published work, we feel confident in the results and in their relevance to a treatment-seeking population of individuals with hoarding disorder.
In conclusion, this study, a collaborative effort between an academic medical centre and a community-based advocacy group, provides empirical support for peer-facilitated treatment, thus offering an alternative form of evidence-based treatment that can substantially increase access to care for this chronic and common disorder. The findings of this study underscore the importance of investing resources in building treatment capacity via community entities, and promoting ongoing community engagement in care to provide an additional avenue for effective evidence-based treatment for individuals who do not have ready access to care by mental health professionals. Additional studies should focus on the role that specific elements of treatment (e.g. assigning clutter buddies) play in increasing adherence and/or treatment response.
Supplementary material
Supplementary material is available online at https://doi.org/10.1192/bjo.2018.30.
Funding
This work was supported through a Patient-Centered Outcomes Research Institute (PCORI) Assessment of Prevention, Diagnosis, and Treatment Options Program Award (number CE-1304-6000). The funder had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript or decision to submit the manuscript for publication.
All statements in this report, including its finding and conclusions are solely those of the authors and do not necessarily represent the views of the PCORI, its Board of Governors or Methodology Committee.







 Open access
Open access
eLetters
No eLetters have been published for this article.