



Introduction
Anomalous aortic origin of a coronary artery affects approximately 0.4–0.7% of the general population, predisposing patients to sudden cardiac death and acute myocardial ischaemia. Reference Cheezum, Liberthson and Shah1–Reference Davis, Cecchin, Jones and Portman3 Concomitant cardiac surgery, such as replacement of the aortic or mitral valve, in patients with coronary anomalies can result in damage or compression of these vessels due to the anatomic proximity of these structures, leading to ischaemic events in the perioperative or postoperative period. The literature has remained divided on the impact of anomalous aortic origin of a coronary artery on rates of postoperative ischaemia following replacement of the aortic valve via transcatheter and surgical interventions. Several small, single-centre studies have reported increased rates of ischaemic events following aortic valve replacement, necessitating high rates of reintervention and resulting in variable effects on long-term morbidity and mortality. Reference Baldonado, Greason and Crestanello4–Reference Naito, Petersen, Reichenspurner and Girdauskas6 In contrast, others have reported no significant postoperative complications, ischaemia, or early mortality in anomalous aortic origin of a coronary artery patients after aortic valve interventions. Reference Liebrich, Tzanavaros, Scheid, Voth, Doll and Hemmer7 Furthermore, there have been few publications that elucidate the short-term and long-term outcomes of mitral valve replacement in patients with anomalous aortic origin of a coronary artery. Reference Doty8–Reference Fabozzo, Rossi, Facci, Bottio and Gerosa12
To date, there have been no large studies assessing the risk of postoperative complications, ischaemia, or reintervention in patients with unrepaired coronary anomalies who undergo surgical replacement of the aortic or mitral valves. Consequently, this project was initiated to bridge this knowledge gap and ascertain whether modification of the surgical technique is required for reimplantation of the anomalous coronary or to protect the aberrant course of the vessel. Secondarily, this study aimed to elucidate whether the anatomy of the anomalous coronary artery impacted postoperative course in this patient population.
Patients and methods
Study design
This was a single institution, retrospective cohort study designed to compare postoperative outcomes after surgical aortic or mitral valve replacement between patients with normal coronary anatomy and those with unrepaired anomalous aortic origin of a coronary artery. Cohort matching was implemented using balancing score strategy to ensure similarity between the cohorts and minimise possible selection bias.
Patients
We identified 29,655 adults who underwent aortic (n = 25,441) or mitral valve (n = 6,203) replacement at Cleveland Clinic from January 2005 to January 2022. Among them, coronary anomalies were diagnosed preoperatively or intraoperatively in 105 patients. We confirmed the presence of anomalous aortic origin of a coronary artery in 55 patients. After exclusion, including prior or concomitant intervention on the anomalous coronary artery relative to the valve surgery of interest, we identified 29 patients with an unrepaired anomalous coronary artery and 29,550 with normal coronary origin (non-anomalous aortic origin of a coronary artery) (Figure 1).

Figure 1. Consort diagram depicting inclusion and exclusion criteria and the creation of a balancing-score-matched cohort. AV = aortic valve; MV = mitral valve; CABG = coronary artery bypass graft; AAOCA = anomalous aortic origin of coronary artery.
Patients with anomalous coronaries had a mean age of 67 ± 14 years, and 48% of this cohort was female. At the time of valve surgery, concomitant operations included septal myectomy (10%), atrial myxoma removal (3.4%), and repair of congenital heart defects (21%). One patient (3.4%) underwent aortic anulus enlargement during valve surgery. The mean age of patients with normal coronary anatomy was 68 ± 14 years, and 37% of these patients were female. The incidence of concomitant procedures at the time of aortic or mitral valve replacement was 1.8% for septal myectomy, 0.13% for removal of atrial myxoma, and 2% for CHD repairs. Aortic anulus enlargement was performed in 804 (2.7%) patients at the time of the index valve operation.
Data
Preoperative patient characteristics, details of the operation, and postoperative morbidity data were abstracted prospectively for quality reporting by independent registry nurses and entered in the Cardiovascular Information Registry. Other Cleveland Clinic electronic medical record databases were also queried. Preoperative echocardiogram images were reviewed to measure the aortic or mitral valve anulus diameter prior to replacement. All data used for this study were approved for use in research by Cleveland Clinic’s Institutional Review Board with patient consent waived (IRB #22-1262, approved on 6/20/2023).
Endpoints
Operative morbidities, ischaemia events and mortality
Operative mortality and major morbidities were defined in accordance with the Society of Thoracic Surgeons National Adult Cardiac Database, and these definitions encompassed mortality during the index surgery, reoperation for any reason, deep sternal wound infection, permanent stroke, renal failure, and prolonged ventilation. Reference Fernandez, Shahian and Kormos13
Time-related coronary intervention and mortality
Long-term follow-up data on coronary intervention were acquired via manual chart review of subsequent outpatient visits, hospitalisations, and procedural interventions, as well as direct patient contact via telephone. Median follow-up of the anomalous coronary cohort was 7 years, and 10% had more than 16 years of follow-up. Median follow-up of the matched normal coronary cohort was 6 years, with 10% having more than 14 years of follow-up. Systematic follow-up for vital status was supplemented with Social Security Death Master File (to 2011) and Ohio State Death Registry data.
Statistical analysis
Statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC) and R version 3.6.0 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are summarised as mean ± standard deviation or as equivalent 15th, 50th (median), and 85th percentiles when distribution of values was skewed. Categorical data are summarised by frequencies and percentages. Differences between preoperative and operative characteristics of the two groups are expressed as standardised mean differences (%). Uncertainty time-related events were expressed using 68% confidence bands (equivalent to ±1 standard error). A type I error of 0.05 was used to assess statistical significance.
Balancing score rationale, development, and matching
RATIONALE: There were several differences in patient and procedure variables between the two cohorts (Table E1). We used balancing score matching to reduce bias between the two groups for comparison of outcomes.
MISSING VALUES: We employed fivefold multiple imputation Reference Rubin14 using multivariate imputation by chained equations to impute missing values.
BALANCING SCORE DEVELOPMENT: Because of the very small sample size in the anomalous coronary group and small frequencies in some of the preoperative variables, we developed a balancing score model using logistic regression with the following selected 11 variables as covariates: gender, age, ejection fraction, fractional ventricular shortening, prior cardiac intervention, number of diseased coronary arteries, presence of left main disease, aortic valve replacement, mitral valve replacement, implantation of a bioprosthetic in the aortic position, and date of index surgery (C-statistic = .70). Gender and age were selected as variables to ensure similar demographic characteristics between the cohorts. Ejection fraction and fractional ventricular shortening were included to ensure comparable baseline ventricular function during preoperative evaluation. Other cardiac comorbidities were accounted for via utilisation of variables such as prior cardiac interventions, the number of diseased coronary arteries, and the presents of left main disease. To ensure similarity between the index valve procedures of interest, the type of procedure was included as a variable, as well as the implantation of a bioprosthetic valve for patients who received an aortic valve replacement. The date of the index surgery was incorporated to account for changes in experience, perioperative management, and surgical technique during the time period of the study. The balancing score for each patient was obtained by averaging five balancing scores calculated from five semi-saturated models based on the imputed data sets. Reference Mitra and Reiter15
MATCHING: Using only the balancing score, anomalous coronary artery cases were matched 1:3 to normal coronary anatomy cases using a greedy matching strategy 16 in the logit domain with a caliper width equal to 0.2 times the standard deviation of the logit of the balancing score, Reference Austin17 yielding 87 well-matched controls (Supplemental Figure E1). An absolute value of standard mean difference ≤ 10% is usually interpreted as acceptable matching. Reference Normand, Landrum and Guadagnoli18
Comparison of continuous outcomes used the Wilcoxon rank-sum test, and categorical outcomes the chi-squared test or Fisher’s exact test as appropriate. Survival and freedom from coronary intervention were estimated nonparametrically by the Kaplan–Meier method and compared using log-rank test. Since we have enough frequency of deaths time to event, as a sensitivity analysis, to account for possible association of the outcome among the matched patients, survival comparison was also made by treating the 29 matched clusters (size of 4) as separate strata.
Results
Anatomy and origin of the anomalous coronary artery
Of the 29 patients with unrepaired anomalous aortic origin of a coronary artery, 21 (72%) underwent replacement of the aortic valve, and 8 (28%) replacement of the mitral valve (Table 1). Mean age 67 years. The most prevalent anomalous coronary arteries were left circumflex (n = 19, 66%) and right coronary (n = 9, 31%). The anomalous left circumflex artery most frequently arose from the right coronary sinus (n = 14, 49%) or right coronary artery (n = 5, 17%). The anomalous right coronary arteries most commonly arose from the left coronary sinus (n = 6, 21%), followed by the suprasinus region (n = 2, 6.9%) and non-coronary sinus (n = 1, 3.4%). In 1 patient (3.4%), an anomalous left anterior descending artery arose from the right coronary sinus. No patients had an anomalous left coronary artery. Slit-like orifices and acute angulation of the anomalous artery were not observed within this cohort of AAOCA. Course of the anomalous vessel was interarterial in 3 patients (10%) and transseptal in 1 (3.4%).
Table 1. The demographic, preoperative, and procedural information from the index surgery before and after cohort matching between patients without anomalous aortic origin of a coronary artery (non-AAOCA group) and patients with AAOCA. This also characterises the anatomy and origin of the anomalous coronary artery within the AAOCA cohort

SD = standard deviation; AAOCA = anomalous aortic origin of coronary artery.
* Valve type was not specified for every patient within the full cohort. The sum of the valves does not equal the total consequently.
** Surgical and percutaneous aortic valve replacement are presented as mutually exclusive.
a Number of patients with data available.
Anomalous versus normal coronary anatomy groups
Prior to matching, patients with normal coronary anatomy had fewer cardiac and non-cardiac comorbidities at the time of the index valve surgery than their counterparts with anomalous aortic origin of a coronary artery. Within the normal coronary anatomy group, 21,122 patients (71%) and 6,195 patients (21%) had replacement of the aortic and mitral valves, respectively (Table 1). In the mitral position, bioprosthesis was most commonly used, and mechanical valves and homografts were implanted less frequently. Within the unrepaired coronary anomaly cohort, surgical aortic valve replacement was performed in 21 patients (72%), while surgical mitral valve replacement occurred in 8 patients (28%).
Preoperative anulus diameter in the matched cohorts
The native aortic anulus diameter was 22 ± 3 mm and 20 ± 4 mm among patients with anomalous coronaries and normal coronary anatomy (P = .051). Similarly, the native mitral anulus was 29 ± 7.2 mm and 28 ± 7.1 mm for the anomalous and normal coronary origin cohorts, respectively (P = .7). An aortic and mitral prosthesis-anulus index was created to determine if oversizing or undersizing of the implanted prosthetic valve contributed to postoperative complications or reintervention in either cohort. Within the anomalous coronary artery patients, the mean aortic prosthesis-anulus index was 1.07, and the mean mitral prosthesis-anulus index was 1.16. In the matched cohort, the prosthesis-anulus index was 1.15 ± 0.22 and 1.09 ± 0.32 for the aortic valve anulus and mitral valve anulus, respectively.
Outcomes of anomalous coronary artery versus matched normal coronary anatomy
Operative morbidities, ischaemia events, and mortality
The presence of an unrepaired coronary anomaly did not extend the operative time or cardiopulmonary bypass time during valve replacement (Table 2). Patients with coronary anomalies had a mean of 85 ± 30 min of myocardial ischaemia time and 110 ± 37 min of cardiopulmonary bypass time. Those with normal coronary anatomy had a mean myocardial ischaemia time of 78 ± 31 min and mean cardiopulmonary bypass time of 100 ± 39 min. One patient had an incidentally diagnosed anomalous circumflex arising from the right coronary experienced incidental laceration, requiring primary repair during the valve surgery. When comparing the two cohorts, there were no statistically significant differences in the occurrence of complications during hospitalisation, including initiation of mechanical circulatory support, atrial fibrillation, sepsis or wound infections, stroke, or renal failure (Table 2). Reoperation after the index surgery for any reason due to a complication occurred in 3 patients (3.4%) in the matched group and 1 patient in the anomalous coronary artery group (3.4%).
Table 2. The operative details, postoperative complications, and operative mortality identified in the matched cohort (non-AAOCA) and AAOCA cohort
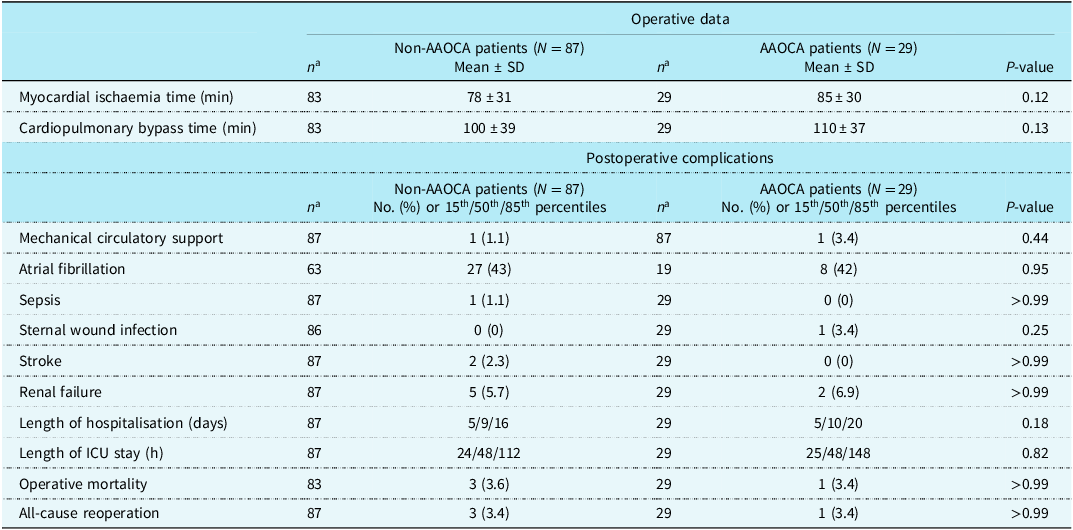
SD = standard deviation; AAOCA = anomalous aortic origin of coronary artery.
Operative mortality was 3.6% among patients with anomalous coronary arteries and 3.4% in those with normal coronary arteries (P > .99).
Time-related coronary intervention and mortality
Long-term surgical or percutaneous coronary reintervention was performed in three patients with an anomalous coronary artery and none of the matched patients (Figure 2). One of these coronary reinterventions involved the anomalous coronary, which occurred 9 years after the index valve surgery to replace the degenerated bioprosthetic valve. During the procedure, an aortic plaque was incidentally noted to be causing severe ostial stenosis of the anomalous right coronary artery which was bypassed by a saphenous vein graft anastomosed to the anomalous right coronary artery. The patient recovered well without any additional complications. The remaining two patients had reinterventions that did not involve the anomalously connected coronary artery. Freedom from coronary reintervention in patients with an anomalous coronary artery was 100% at 30 days, 96% at 1 year, 92% at 2 years, 92% at 5 years, and 83% at 10 years (P[log-rank] = 0.005, Figure 2).

Figure 2. Kaplan–Meier nonparametric estimate of freedom from coronary reintervention in the matched cohort. Red represents the anomalous aortic origin of a coronary artery (AAOCA) group. Blue represents the non-AAOCA (matched) group. Symbols (circles and triangles) are Kaplan–Meier estimate of survival positioned at each reintervention event. Vertical bars indicate a 68% confidence interval equivalent to ±1SE. Numbers below x-axis are the number of patient at risk.
Survival between the anomalous coronary and normal coronary anatomy patients at 30-days, 1-year, 5-years, 10-years, and 16 years were 97% versus 99, 86% versus 93, 83% versus 80, 59% versus 53, 42% versus 34%, respectively (P[log-rank] = 0.8, Figure 3). Note that a sensitivity analysis of survival comparison yielded a similar results (P = .8).

Figure 3. Kaplan–Meier nonparametric estimate of survival in the matched cohorts. Red represents the anomalous aortic origin of a coronary artery (AAOCA) group. Blue represents the non-AAOCA group. Symbols (circles and triangles) are Kaplan–Meier estimate of survival positioned at each deaths event. Vertical bars indicate a 68% confidence interval equivalent to ±1SE. Numbers below x-axis are the number of patient at risk.
Discussion
Principal findings
Comparison of surgical aortic and mitral valve replacements in patients with unrepaired anomalous aortic origin of a coronary artery to those with normal coronary anatomy yielded comparable rates of postoperative complications, coronary reintervention, and mortality, regardless of the anomalous coronary variant. Our cohort primarily encompassed patients with lower risk coronary anomalies, such as an anomalous left circumflex or anomalous right coronary. The diameter of the aortic and mitral valve anuli was similar between patients with and without aberrant coronary anatomy, and there was no significant oversizing or undersizing of the implanted prosthetic valves relative to the preoperative diameter. Reoperation was rare in both cohorts, and only one patient required reintervention on the anomalous coronary artery.
Anomalous aortic origin of a coronary artery is uncommon in patients who undergo surgical aortic valve replacement or mitral valve replacement at a high-volume center. Presumably, high-risk anomalous coronary artery variants or those presenting with ischemic symptoms in the preoperative setting were repaired prior to or concomitantly with surgical replacement of the aortic or mitral valve, resulting in exclusion of these patients from our study.
The American Heart Association/American College of Cardiology guidelines for repair of anomalous aortic origin of a coronary artery provides a class I recommendation for surgical intervention in patients with ischaemic symptoms or diagnostic testing that is positive for ischaemia, regardless of which coronary is anomalous. Reference Stout, Daniels and Aboulhosn19 Surgical repair is a class IIa recommendation for patients with an anomalous left coronary artery from the right sinus in the absence of ischaemia. Similarly, surgical intervention is a class IIa recommendation for patients with an anomalous right coronary after from the left sinus with ventricular arrhythmias. If no ventricular arrhythmias are present in this patient population, surgical repair is a class IIb recommendation, and continued observation is also a feasible management plan. These guidelines reflect prior studies showing increased risk of symptomatic ischaemia for the anomalous left main compared to the anomalous right coronary artery. There is also an elevated risk of ischaemia and sudden cardiac death if a slit-like orifice or intramural course is present. Patients are most at risk for ischaemic events and sudden cardiac death during periods of high cardiac output or aortic wall tension. The presence of coronary artery disease may exacerbate symptoms and ischaemic events in this patient population, regardless of the anatomy of the anomalous coronary artery.
There has been limited discussion in the literature to date regarding the utility of repairing anomalous coronary arteries at the time of aortic or mitral valve replacement. Valve replacement in this patient population poses a risk for intraoperative or postoperative injury to the anomalous vessel via inadequate myocardial protection, suture ligation, laceration during an oblique aortotomy at the level of the noncoronary sinus, or compression by the prosthetic valve. Reference Doty8,Reference Gaudino, Di Franco and Arbustini20 To minimise these risks, some recommend undersizing the aortic prosthesis, avoiding stented valves, and utilising sutureless valve implantation techniques. Reference Yokoyama, Takagi, Mori and Aoyagi9 Reference Botta, Amodio and Pagano,10 Gruber et al. presented a case report of a mitral valve replacement in a patient with an anomalous retroaortic left coronary artery that originated from the right coronary artery. Reference Gruber, Duffy and Hamdan11 Postoperatively, the patient developed 100% occlusion of the anomalous left main coronary artery requiring percutaneous reperfusion. Similarly, Fabozzo et al. published a case report detailing a mitral valve repair with a complete prosthetic ring in a patient with an anomalous left circumflex. Reference Fabozzo, Rossi, Facci, Bottio and Gerosa12 In the immediate postoperative period, the patient developed ventricular tachycardia and haemodynamic instability in the setting of mechanical occlusion of the anomalous circumflex by the annular ring.
In our cohort, one patient suffered accidental laceration to a previously undiagnosed retroaortic left circumflex arising from the right coronary during aortic valve replacement. There otherwise was no evidence of compression or suture ligation of the anomalous coronary after valve replacement. Patients with and without an anomalous coronary artery experienced similar hospital courses after surgical replacement of the aortic or mitral valve, as demonstrated by the comparable complication rates, length of hospitalisation, duration in the ICU, all-cause morbidity and mortality, and reintervention rates. The presence of presumed low-risk anomalous coronary artery variants, consisting of the right coronary and circumflex arteries, did not adversely affect the risk of postoperative complications, ischaemic events, or survival after valve replacement in this cohort. Subsequent surgical and interventional coronary reintervention were rare in this patient population.
With careful patient selection, surgical replacement of the aortic or mitral valve is safe and low risk in patients with unrepaired anomalous aortic origin of a coronary artery. We found insufficient evidence to recommend surgical intervention on otherwise benign cases of AAOCA at the time of aortic and mitral valve replacement. Patients who do not meet criteria for AAOCA repair can safely undergo valve operations. Consequently, care should be taken to identify the origin and course of all coronary arteries prior to replacement of the aortic or mitral valve to determine whether concomitant repair of a coronary anomaly would be beneficial at the time of valve surgery. Each patient’s unique coronary anatomy should be taken into consideration to determine whether unroofing, translocation, or bypass grafting is necessary to correct the anomalous course or minimise the risk of future ischaemic events.
Limitations
This study was limited by the relatively small cohort size of patients with unrepaired anomalous aortic origin of a coronary artery who underwent an aortic or mitral valve replacement. The field may benefit from future studies investigating other institutions’ experiences with this patient population. Additionally, it was challenging to account for variations in operative technique or perioperative management of these patients due to the time period investigated and number of surgeons involved in these procedures. Another primary limitation of our study was the absence of non-invasive stress testing data. While our study accounted for self-reported symptoms of possible ischaemia during the timeframe prior to the index valve surgery, it was difficult to ascertain whether these symptoms were the result of the valve dysfunction, anomalous coronary origin, acquired coronary artery disease, or non-cardiac pathologies. Similarly, we lacked more specific ischaemia testing for patients who reported cardiac symptoms on long-term postop follow-up. Therefore, it is challenging to ascertain whether the anomalous coronary artery resulted in ischaemia could have been repaired at the time of valve replacement. Furthermore, both cohorts included patients who were lost to follow-up despite our chart review and attempts at telephone contact, and our follow-up data may be incomplete or truncated as a result.
Conclusions
This study highlighted that aortic or mitral valve replacement in the setting of an unrepaired, low-risk variant of anomalous aortic origin of a coronary artery may be safe and effective in an adult patient population, although publication of additional literature and long-term follow-up data on this patient population is required to confirm these findings. While there was a slightly higher postoperative reintervention rate within patients with anomalous coronary anatomy, these reinterventions were not due to atherosclerotic disease outside the anomalous coronary. Consequently, the presence of a coronary anomaly did not increase the risk of ischaemia or reintervention to address the anomalous coronary artery, further suggesting that aortic and mitral valve replacement are safe and efficacious within this patient population. Furthermore, we emphasised the importance of accurate preoperative diagnosis of the anomalous coronary anatomy to avoid injury at the time of valve surgery. Certain coronary anomalies, such as a retroaortic circumflex arising from the right coronary sinus, could pose considerable challenges during aortic valve replacement if not identified during the preoperative period, underscoring the utility of thorough preoperative workup for all valve surgery candidates.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951124025368.
Acknowledgements
Siddhartha Sahai contributed to the study by calling patients for long-term follow-up.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
The authors declare none.







