



For the general population of children and adolescents, there is support for a positive relation between physical activity and indicators of physical, psychological and cognitive health.(Reference Poitras, Gray, Borghese, Carson, Chaput and Janssen1) Thus, it is tempting to assume that physical activity should have the same positive associations for children and adolescents with congenital heart disease (CHD). Of the children born with a CHD, 3–5% have an isolated valvular aortic stenosis, with 80% of the patients being male. Valvular aortic stenosis is a complex and lifelong disease often requiring repeated interventions, particularly in patients with neonatal treatment(Reference Hill, Ginde, Rios, Frommelt and Hill2,Reference Kjellberg Olofsson, Berggren, Soderberg and Sunnegardh3) , and residual or acquired abnormalities of the left heart structure might affect cardiovascular capacity.(Reference Kipps, McElhinney, Kane and Rhodes4) For the growing individual, this uncertainty regarding future operations and the timing of treatment might affect many aspects of life. Physical activity may be a complicated issue with physical and emotional barriers such as restricted cardiovascular capacity(Reference Schaan, Macedo, Sbruzzi, Umpierre, Schaan and Pellanda5) and overprotective parents.(Reference Bar-Mor, Bar-Tal, Krulik and Zeevi6) Conflicting advice from the patient’s cardiologist may also hinder engagement in physical activities(Reference Caterini, Campisi and Cifra7) as restrictions have traditionally been recommended to prevent sudden cardiac death(Reference Takken, Giardini, Reybrouck, Gewillig, Hovels-Gurich and Longmuir8) In the modern era, the perceived risk for sudden cardiac death in children and adolescents with valvular aortic stenosis has decreased, probably due to a more active approach to intervention(Reference Mandalenakis, Giang, Eriksson, Liden, Synnergren and Wåhlander9) For adolescents, there is increased pressure from peers to engage in physical activity(Reference Jago, Brockman, Fox, Cartwright, Page and Thompson10,Reference Sawka, McCormack, Nettel-Aguirre, Hawe and Doyle-Baker11) Consequently, engaging in physical activity may evoke mixed emotions that in turn may have complex effects on some aspects of the child’s or adolescent’s health-related quality of life and life satisfaction but also on motor development and future physical health(Reference Bjarnason-Wehrens, Dordel, Schickendantz, Krumm, Bott and Sreeram12,Reference Brudy, Hock, Häcker, Meyer, Oberhoffer and Hager13)
No clear relationship between objectively measured physical activity and health-related quality of life or satisfaction with life has been established in children and adolescents with CHD, but their overall health-related quality of life is not found to be lower than that of healthy controls(Reference Dulfer, Helbing, Duppen and Utens14,Reference Schrøder, Boisen, Reimers, Teilmann and Brok15) The focus in previous studies has mainly been patients with a univentricular heart after Fontan procedure(Reference Hedlund, Lundell, Villard and Sjoberg16–Reference Müller, Christov, Schreiber, Hess and Hager18) and these relationships have not been evaluated in patients with valvular aortic stenosis.
The aim of this study was, therefore, firstly to investigate whether there are any differences in health-related quality of life and life satisfaction between children and adolescents treated for valvular aortic stenosis and their healthy peers. Secondly, we aimed to investigate the associations between physical activity, health-related quality of life and life satisfaction.
Materials and method
Participants
All patients treated for congenital isolated valvular aortic stenosis at the two referral centres for paediatric heart surgery in Sweden and born between 2001 and 2012 (age range 8–18 years, M = 12.72, SD = 3.48) were identified in local surgical registers, constituting a complete national cohort (n = 114, female 22.6%). For each patient, five healthy controls matched for age, gender, and geographical location were generated from Statistics Sweden (www.scb.se).
The patients were asked for health problems restricting their ability to be physically active. None were excluded for this reason. One patient who was willing to participate was excluded due to a recent surgical intervention. The response rate among patients was 43%. Participants were in median 18 days (range 0 days–12.5 years) at primary aortic valve intervention and had in mean 1.33 interventions while non-participants were in median 25 days (1 day–8,1 years) at first intervention and had in mean 1.66 interventions.
Our final sample consisted of 48 patients with completed questionnaires for KIDSCREEN-52 of whom 46 also completed the Satisfaction with Life Scale and 41 had a valid physical activity measurement. The control group consisted of 43 healthy participants with completed KIDSCREEN-52 questionnaires of whom 39 also completed Satisfaction with Life Scale and 37 performed a valid physical activity measurement.
After completing the study, the participants received a cinema ticket worth approximately 15 USD.
Procedure
Patients and controls were sent postal invitations to participate including information about the study adapted to children, adolescents, and parents, and two postal reminders were sent. One parent of a non-responding patient was also contacted by phone to verify that they had received the invitation. Data collection was performed during the same week in patients and controls to adjust for seasonal variation in physical activity. Questionnaires and the accelerometer were delivered by post with age-customised instructions. All participants and/or parents provided a written consent.
Measures
Health-related quality of life
Children’s and adolescents’ health-related quality of life were assessed with the KIDSCREEN-52 self-report and parent proxy report.(Reference Ravens-Sieberer, Gosch, Rajmil, Erhart, Bruil and Duer19) KIDSCREEN-52 has been validated and found to have good reliability in several countries, including Sweden, and can be used as a measure of subjective health in both healthy and chronically ill children and adolescents.(Reference Ravens-Sieberer, Herdman, Devine, Otto, Bullinger and Rose20) It consists of 52 items divided into ten domains: Physical Well-being, Psychological Well-being, Moods and Emotions, Self-Perception, Autonomy, Parent Relations & Home Life, Financial Resources, Social Support and Peers, School Environment, Social Acceptance (Bullying). The answer alternatives range from 1 = Never to 5 = Always. A higher score indicates better health-related quality of life for each subdomain. The KIDSCREEN-52 items meet the assumptions of the Rasch model; thus, the subdomain items are summed and transformed into Rasch person parameter estimates. The Rash scores are then transformed into T scores, which are easier to interpret, as the mean T score is always 50 and the SD is 10. Participants with more than one missing item on a subdomain are excluded according to the manual. Reference norms have been obtained for a large European sample of children aged 8–17 years (Reference Ravens-Sieberer, Herdman, Devine, Otto, Bullinger and Rose20), and Swedish norms exist for adolescents aged 12–18 years. Cronbach’s alpha values for the self-reports were .72–.84, except the physical well-being scale with an alpha of .69. For the proxy reports, the values ranged from .76–.91, except the self-esteem subscale with a value of .63.
Life satisfaction
Life satisfaction is a person’s global assessment of their satisfaction with life.(Reference Diener, Emmons, Larsen and Griffin21,Reference Pavot, Diener and Diener22) We used the child version of the Satisfaction with Life Scale for children 8–12 years (Reference Gadermann, Schonert-Reichl and Zumbo23) and the adult version for adolescents 13–18 years.(Reference Diener, Emmons, Larsen and Griffin21) The scale consists of five items with answer alternatives from 1–5 for the child scale and 1–7 for the adolescents. It has been successfully used in similar age groups in a Swedish context.(Reference Virta, Sam and Westin24) The measure was calculated by using the mean across items; thus, higher values represent better life satisfaction. Cronbach’s alpha values for the scales were .81 and .82 for the children and adolescents, respectively.
Physical activity
Free-living accelerometer data were collected using the triaxial accelerometer Axivity AX3 (Axivity Ltd, Newcastle upon Tyne, UK). The participants were instructed to wear the accelerometer over the right hip for 7 consecutive days and only to remove the sensor for water-based activities (including showers, baths and swimming). Daytime activities, sleep time, and sports participation were recorded in diary.
Accelerometer protocol
We used OmGUI software (Axivity Ltd., Newcastle upon Tyne, UK) for accelerometer initialisation and data extraction, with a sampling frequency of 50 Hz and ± 8 g sensitivity (1 g is equivalent to Earth’s gravity). The accelerometer output data were resampled to 30 Hz and processed by the frequency extended method (Reference Fridolfsson, Borjesson and Arvidsson25,Reference Fridolfsson, Borjesson, Buck, Ekblom, Ekblom-Bak and Hunsberger26) with a three-second epoch length, as recommended for children.(Reference Aadland, Andersen, Anderssen, Resaland and Kvalheim27) Time spent at different intensity levels was estimated from previously published cut-off points.(Reference Arvidsson, Fridolfsson, Buck, Ekblom, Ekblom-Bak and Lissner28) Non-wear time was defined as 60 min of uninterrupted zeros, allowing exceptions of < 2 min of activity. Valid criteria for accelerometer data were set to ≥ 4 days of measurement (≥ 3 weekdays and ≥ 1 weekend day) with a valid day set to ≥ 10 hours per day of wear time.
Statistical analyses
t-tests were used to investigate age group differences in health-related quality of life and life satisfaction. Bivariate Spearman’s correlation was used to investigate the association between time spent at different physical activity intensities and health-related quality of life and life satisfaction. In addition, some associations were visualised by scatter plots with lines fitted by linear regression. No adjustments were performed for multiple statistical tests, as this procedure also has limitations.(Reference Perneger29) Instead, it is recommended to present the outcome of all tests, to allow understanding of whether reasonable conclusions can be drawn from data. Data processing and statistical analyses were performed in MATLAB, version R2020b (The MathWorks Inc., Natick, Massachusetts) and IBM SPSS Statistics, version 25 (IBM Corp., Armonk, NY). The statistical analysis has been chosen based on the distribution of data.
Results
Data were collected between September 2019 and June 2020. Descriptive statistics for health-related quality of life can be found in Table 1a and Table 1b. The cohort reflects the gender distribution for the diagnosis. No differences between the health-related quality of life domains were found between patients’ and controls’ self-reports, either for the children or for the adolescents. However, the parents of the adolescent patients experienced that their offspring had less autonomy than reported by the parents of the healthy controls. Because the Swedish KIDSCREEN-52 norm values (mean T scores) differ from the European norm mean T scores, the results were compared with the control group and with the Swedish norm values for healthy adolescents. The only difference found between the Swedish norm values and our patients was that the patients experienced less physical well-being than the healthy population norm (Table 1b). T scores for the patients, controls and parents are depicted in Figure 1.
Table 1a. Descriptive statistics and t-test comparisons of HRQoL scores between children 8–12 years treated for valvular aortic stenosis and their controls, for both self-report and parent proxy reports
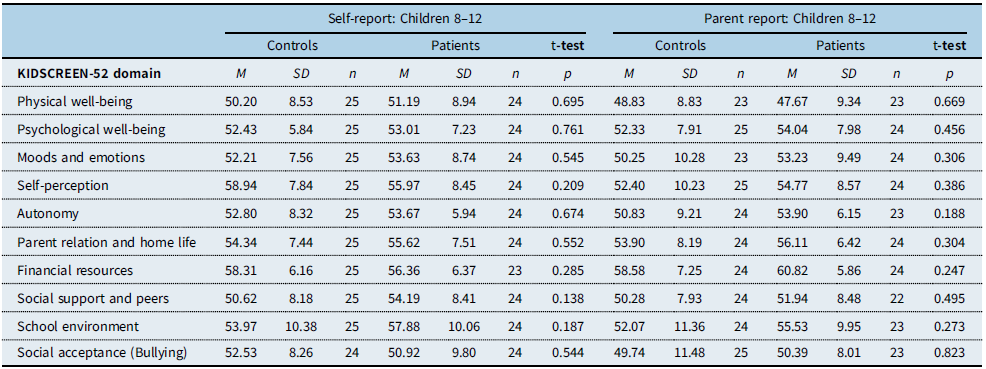
(HRQoL, health-related quality of life.)
Table 1b. Descriptive statistics and t-test comparisons of HRQoL scores between adolescents aged 13–18 years with congenital valvular aortic stenosis and their controls, for both child and parent reports
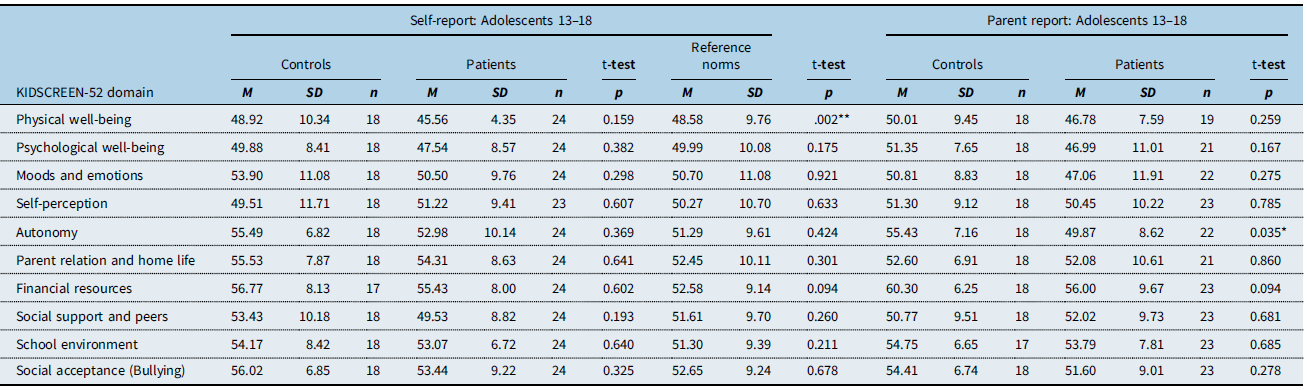
* p < .05.
** p < 01. Note: the reference norms refer to healthy Swedish adolescents aged 12–18 years. (HRQoL, health-related quality of life.)
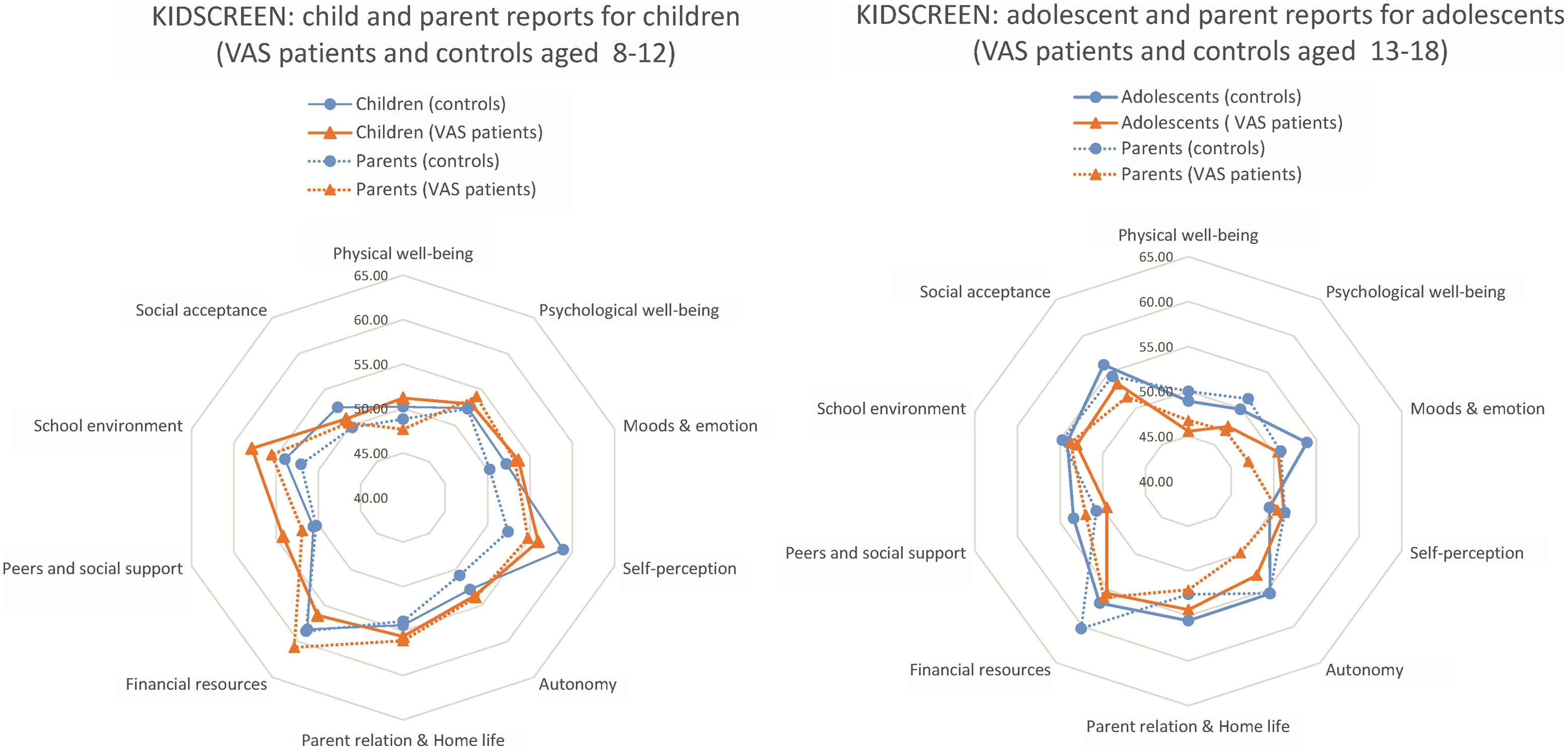
Figure 1. (Left) Sum score scale comparison showing the HRQoL self-reports of children aged 8–12 years with valvular aortic stenosis, their parents’ proxy reports, the control children’s self-reports and their parents’ proxy reports. (Right) Sum score scale comparison showing the HRQoL self-reports of adolescents aged 13–18 years with valvular aortic stenosis, their parents’ proxy reports, the control adolescents’ self-reports and their parents’ proxy reports.
No difference in life satisfaction was found between the child patients (M = 4.61, SD = 0.54) and controls (M = 4.63, SD = 0.46), t(44) = 0.12, p = .907. Neither was any difference found between the adolescent patients (M = 5.60, SD = 1.05) and controls (M = 5.24, SD = 1.85), t(44) = −1.014, p = .795.
Associations between physical activity, health-related quality of life, and life satisfaction
Time spent in physical activity of different intensities is shown in Table 2. A pattern indicating a negative correlation between time spent in moderate to vigorous physical activity and sports participation with life satisfaction and psychological well-being for the adolescents with aortic stenosis can be seen in both self-reports and parent proxy reports (Fig 2). This pattern is only evident for the adolescent patients, not for their healthy controls nor for the child group. Figure 3 illustrates the parent proxy reports of psychological well-being correlated with time spent in physical activity at the three highest intensity levels. For the children with aortic stenosis, a statistically significant positive correlations between time spent in moderate physical activity and psychological and physical well-being were seen. As can be seen in Figure 2, sports participation correlated highly with the amount of vigorous and very vigorous physical activity, indicating that a lot of the high-intensity physical activity could be due to high engagement in sports. A strong negative correlation was seen between sedentary time and psychological well-being (parent proxy) in children with aortic stenosis, with life satisfaction for the control adolescents and with physical well-being for the control children (parent proxy). For exact correlation figures, see Appendix.
Table 2. Time spent in physical activity at different intensity levels, comparing children and adolescents with congenital valvular aortic stenosis with their controls
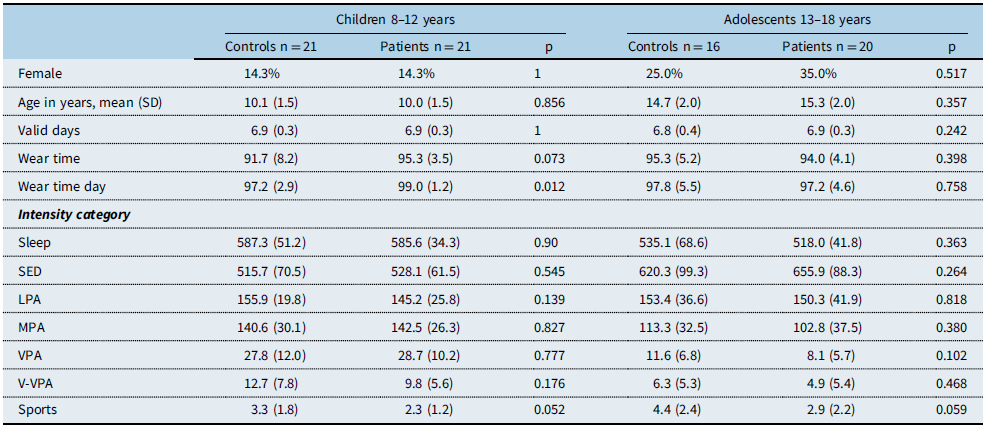
Note: Physical activity intensity categories are defined by VO2net (mass-specific net oxygen consumption) cut-off points. Time for each intensity category is shown as minutes per day, mean (SD), and wear time in percent, mean (SD). Sports is presented as number of times per week, mean (SD)
(SED, sedentary physical activity; LPA, light physical activity; MPA, moderate physical activity; VPA, vigorous physical activity; V-VPA, very vigorous physical activity; Sports, participation in sports.)
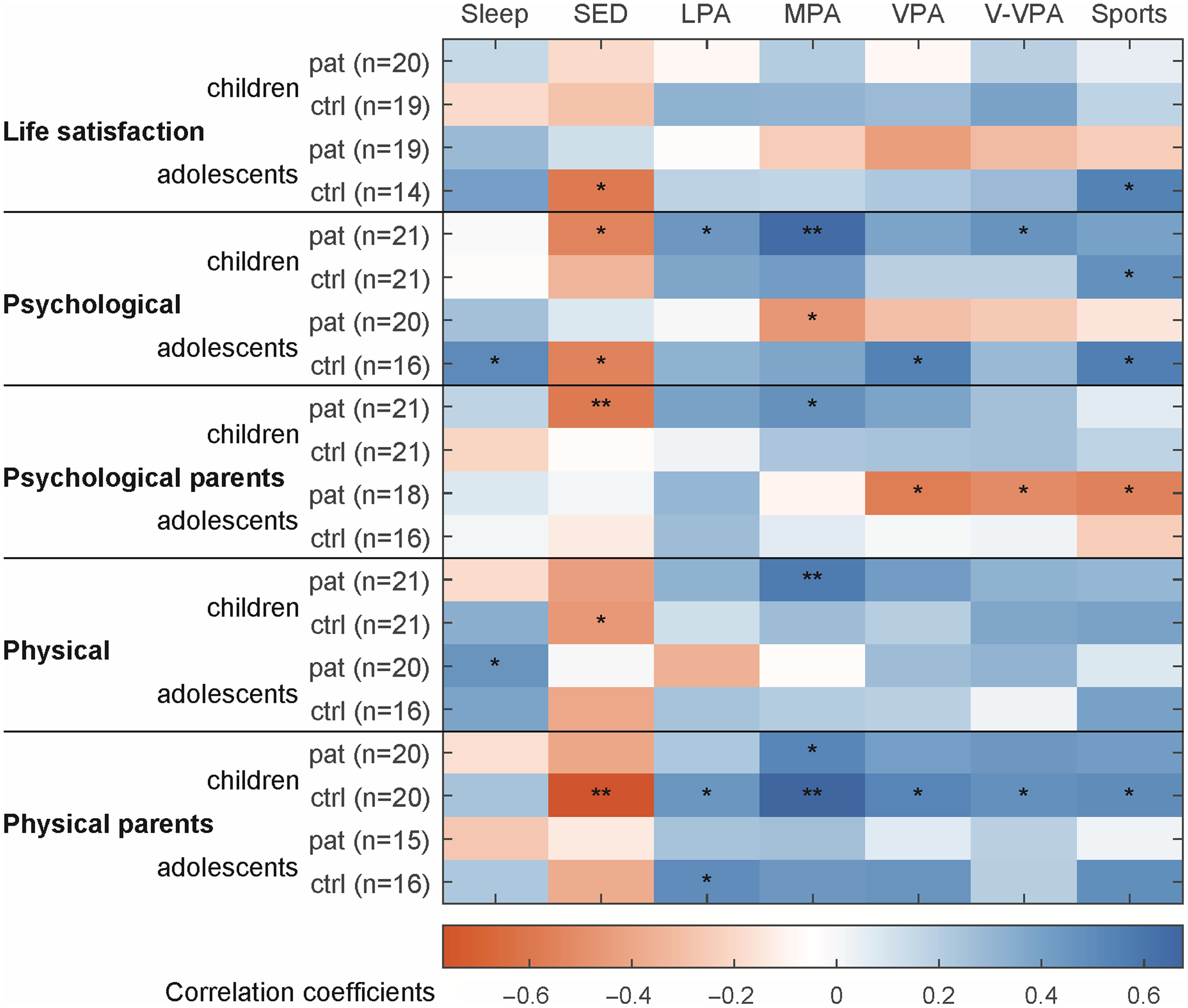
Figure 2. Bivariate Spearman correlations between time spent in physical activity at different intensities, life satisfaction, physical well-being and psychological well-being, for both self-reports and parent (proxy) reports.
Note. Blue and red cells represent positive and negative correlations, respectively. * p < 0.05, ** p < 0.01. (Pat, patients; ctrl, controls; SED sedentary; LPA light physical activity; MPA moderate physical activity; VPA vigorous physical activity; V-VPA very vigorous physical activity.)
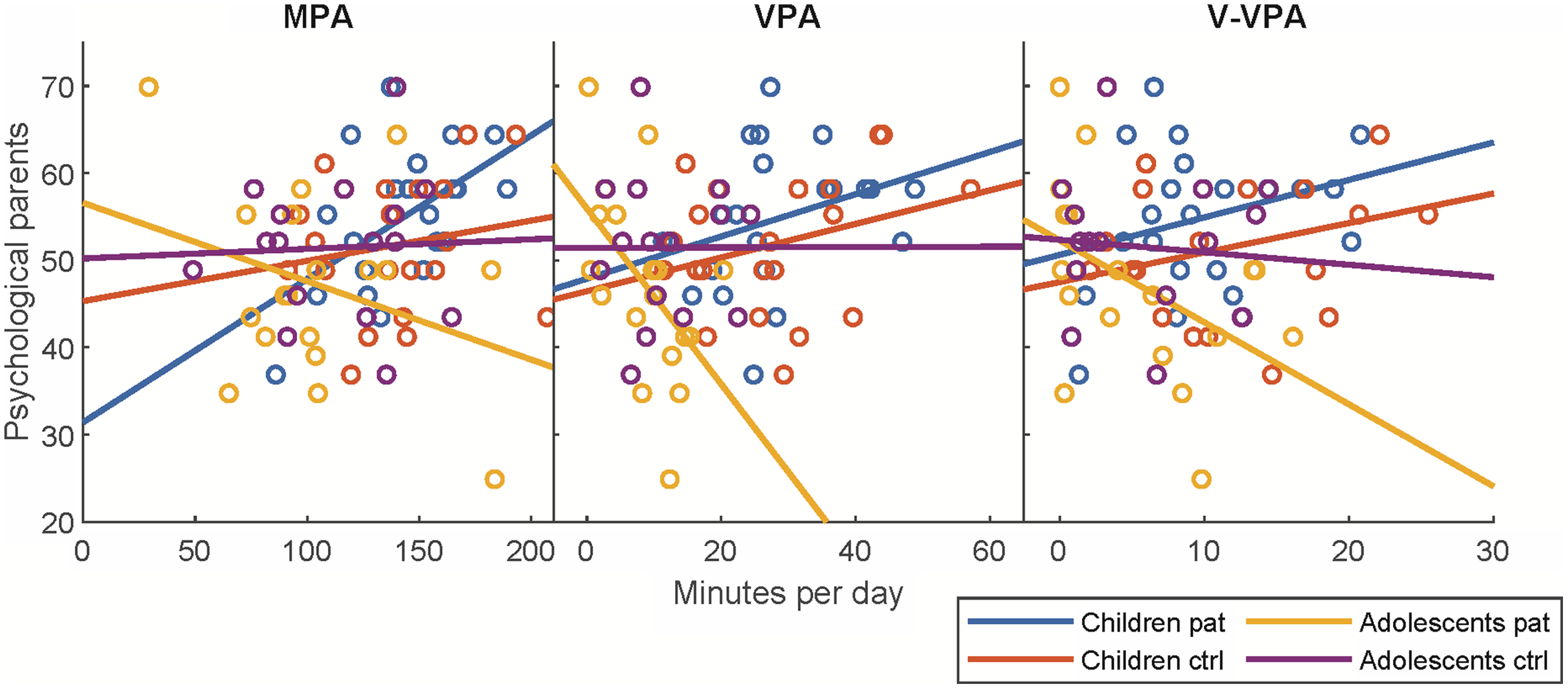
Figure 3. Scatterplots of the association between parent reports of psychological well-being and three levels of physical activity intensity.
Note. Separate linear regression lines are fitted, based on age group and responder. (MPA moderate physical activity; VPA vigorous physical activity; V-VPA very vigorous physical activity.)
Discussion
Life satisfaction and health-related quality of life scores did not differ significantly in children and adolescents with valvular aortic stenosis compared to healthy controls. Parents of the adolescent patients did, however, report that their adolescents had less autonomy compared to the healthy controls. In comparison to the Swedish norm values, adolescent patients rated their physical well-being lower. Our findings are in line with a systematic review and meta-analysis that concluded that health-related quality of life is not lower in adolescents with CHD.(Reference Schrøder, Boisen, Reimers, Teilmann and Brok15) Other studies have reached the same conclusion for children and adolescents with CHD of varying severity (Reference Bertoletti, Marx, Hattge and Pellanda30,Reference Reiner, Oberhoffer, Ewert and Müller31) , although subgroups of patient with complex CHD are reported to have impaired health-related quality of life scores.(Reference Hedlund, Lundell, Villard and Sjoberg16,Reference Grosch, Andresen, Diep, Diseth and Möller32,Reference Svensson, Idvall, Nilsson and Liuba33) Interestingly, we found a negative relation between adolescent patients’ physical activity and sports participation and their life satisfaction and psychological well-being. These results were not evident for the children with aortic stenosis. There may be many reasons for this difference. In younger children, the family is often able to help the child adjust to the consequences of the disease and can adjust the family’s activities to fit in with the child’s needs.(Reference Dowda, Pfeiffer, Brown, Mitchell, Byun and Pate34) This allows the child with CHD to engage in physical activities at their own pace and according to their own wishes, providing a more positive association between physical activity and different domains of health-related quality of life, such as physical and psychological well-being. Adolescence is a time marked by transition and changes which in themselves may affect aspects of subjective well-being and life satisfaction.(Reference González, Casas and Coenders35) Expectations of physical performance and competition increase, the influence of peers becomes more important, and feelings of fitting in become the focus of this developmental phase.(Reference McMinn, van Sluijs, Wedderkopp, Froberg and Griffin36) During this phase, adolescents’ physical activity is influenced by their peers, and studies show that the patients will try to match their friends’ activity patterns, (Reference Sawka, McCormack, Nettel-Aguirre, Hawe and Doyle-Baker11) and they can even increase their level of activity to match a friend’s level.(Reference Jago, Brockman, Fox, Cartwright, Page and Thompson10) In order to fit in and to perform as their peers do, adolescents with aortic stenosis are at risk of pushing their physical activity to extremes. Supporting this, a study has shown that adolescents with higher physical activity levels may be more aware of their physical limitations than less active patients.(Reference Parent, Sterrett, Caldwell, Darragh, Schamberger and Murphy37)
Another contributing factor could be that some adolescents treated for valvular aortic stenosis have more severely impaired physical performance than they themselves perceive and thus fail to take their limitations into account in their daily lives.(Reference Kipps, McElhinney, Kane and Rhodes4) This could add to the struggle for the adolescent to meet requirements and expectations set not only by themselves but also by parents, teachers, sports coaches, and peers. This may contribute to our finding that adolescents who spent more time in high-intensity physical activity and had higher sports participation, rated their psychological well-being lower than adolescents who spent less time in high-intensity physical activity.
In adolescence, training intensity might reach an elite level and although cardiologists stress the importance of physical activity, training at such high intensity may not be recommended due to the risk of sudden cardiac death.(Reference Takken, Giardini, Reybrouck, Gewillig, Hovels-Gurich and Longmuir8) This may result in mixed messages from the health care providers, as physical activities that were encouraged during early childhood need to be limited in adolescence. Thus, providing children and adolescents with individualised advice on physical activity on a level appropriate to promote a healthy lifestyle remains a challenge.
Future studies need to further address the negative relation between physical activity intensity and psychological well-being and life satisfaction. For example, qualitative interview studies could be conducted with the adolescents engaged in more intense physical activity to better understand how they experience their quality of life.
Another implication of our results is that follow-up programmes should assess both medical issues, physical activity, and physical and psychological well-being, as new challenges need to be addressed when children progress into new developmental phases.
Limitations
Strengths of the study are the use of an objective method of measuring physical activity, which has made it possible to correlate different health-related quality of life domains and life satisfaction with time spent in different levels of physical activity and a study group of patients with one well-defined diagnosis. As the complete national cohort of patients treated for valvular aortic stenosis was invited to participate, no power analysis was performed. A limitation is that loss of patients and controls during recruitment made the sample rather small, which may have influenced the outcome of the analysis. It is possible that participants are more physically active and have higher health-related quality of life than non-participants. Information from non-participating controls was not accessible in accordance with ethical regulations.
It should be noted that the cross-sectional design of the study makes the inferences regarding differences between children and adolescents in the association between physical activity and certain aspects of health-related quality of life slightly limited. It could be that the differences are not a result of differences in developmental phases but rather due to cohort effects. However, the suggestion of cohort effects is not so plausible, given that the recommendations for the care of these patients have not changed substantially over the last two decades.
Conclusion
Overall, children and adolescents treated for valvular aortic stenosis showed similar life satisfaction and health-related quality of life to their healthy peers. Adolescents experienced their physical well-being as slightly lower than the Swedish reference norm. In children, a positive correlation between physical activity and well-being was present but in adolescents a pattern of negative correlations between time spent in high-intensity physical activity and more frequent sports participation with life satisfaction as well as psychological well-being was found, both in self-reports and in the parent proxy reports. In conclusion, our study highlights the positive effect of physical activity in children as well as the challenge and the need to give individualised advice on physical activity to adolescents with CHD. While moderate exercise may be beneficial to several patients’ well-being, high-intensity physical activity and sports participation in particular may have the opposite effect.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1047951122000920
Acknowledgement
We are grateful to Arielle Reitberger at the Pediatric Cardiology department, Karolinska University Hospital, for assistance in the recruitment of the participating patients.
Funding
This work was supported by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (SU 2018–04267), and from the Research and Development Department, Västernorrland County Council.
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation in Sweden and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the Central Ethical Review Board in Gothenburg, approval no. 582-18.







 Open access
Open access