


Evidence for the impact of eating behaviours on health is overwhelming and alarming. A study of over 20 000 UK adults reported that eating less than five portions fruit and vegetables daily was associated with a significantly higher risk of mortality after 11 years compared with adults who ate five or more portions daily (relative risk 1·44, 95 % CI 1·31, 1·59)( Reference Khaw, Wareham and Bingham 1 ).
Effective interventions are needed to change eating behaviours. It is apparent that many interventions to change behaviours are designed according to the ISLAGIATT principle (a term coined by Martin Eccles, Emeritus Professor of Clinical Effectiveness), an acronym for ‘it seemed like a good idea at the time’. This term is intended to encapsulate the non-systematic, non-comprehensive approach to designing interventions, essentially guessing at what might be the solution without having understood the problem.
The present paper summarises a systematic, comprehensive method of intervention design described in the recently published book The Behaviour Change Wheel: A Guide to Designing Interventions (BCW Guide)( Reference Michie, Atkins and West 2 ) which brings together recently developed tools in behavioural science intended to be useful and usable to those tasked with changing behaviour but who do not necessarily have a background in behavioural science. The method is similar to that described in a paper published in Nutrition Bulletin in 2012( Reference Atkins and Michie 3 ); since then the methods have been refined and examples are included of how these tools and methods have been used to understand and change eating behaviours.
Using theory in intervention design
The Medical Research Council has published guidance on designing and evaluating complex interventions( Reference Craig, Dieppe and Macintyre 4 ). The BCW Guide puts ‘flesh on the bones’ of this guidance, in particular where the Medical Research Council guidance advocates the use of theory in intervention design. Using theory in intervention design has a number of benefits: it can provide a framework to facilitate the accumulation of evidence, i.e. summarising what is known; it can permit communication across research groups, i.e. a common language; theory can be used as a starting point for intervention design to identify what needs to shift in order for behaviour to change and also in the evaluation of interventions by identifying mechanism of action, i.e. how an intervention is working. Two theory-based tools are described in the present paper. A companion to the BCW Guide, the ABC of Behaviour Change Theories ( Reference Michie, West and Campbell 5 ) summarises eighty-three theories identified in a cross-disciplinary project, drawing on psychology, sociology, anthropology and economics. The component constructs for each theory are listed and some guidance to their use is provided.
Designing interventions using the Behaviour Change Wheel
The intervention design method described in the BCW Guide is separated into three tasks for intervention designers: (1) understand the behaviour; (2) identify intervention options; (3) identify content and implementation options. These tasks are described in greater detail.
Understand the behaviour
Define problem in behavioural terms. In the first instance, intervention designers are encouraged to define the problem in behavioural terms. There are two components to this: (i) who is performing the behaviour and (ii) what the behaviour is. The rationale for this is that if a problem is expressed in terms of outcome, e.g. weight gain, this does not indicate what behaviours one is trying to change or whose behaviour is involved. By stating for example, that the ‘who’ is parents of obese children and the ‘what’ is serving larger than recommended portion sizes there is now a behaviour to target.
Select a target behaviour. Behaviour does not occur in a vacuum, it occurs within constantly evolving systems and contexts. Fig. 1 gives an example of the inter-dependence of behaviours related to healthy eating.
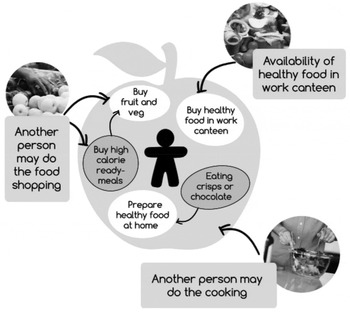
Fig. 1. Behaviour as part of a system: the example of healthy eating behaviours( Reference Michie, Atkins and West 2 ).
Intervention designers are encouraged to begin by generating a list of all the potential behaviours that may be relevant to the problem they are trying to solve. Then consider each behaviour in terms of: the impact of changing the behaviour (what difference will it make?) the likelihood of changing the behaviour (to what extent can the behaviour be easily changed?) and any spillover effect (will changing the behaviour positively or negatively influence other behaviours?). By considering these criteria, intervention designers can make pragmatic decisions on which behaviour to target.
When tasked with designing interventions to change behaviour designers will understandably want ‘value for money’ and as such may seek to target multiple behaviours. Designers are encouraged to consider that it may be more effective to intervene intensively on one or two target behaviours and build on small successes than to attempt to change too much too soon.
Specify the behaviour targeted for change. For each target behaviour, intervention designers should specify the behaviour in terms of: (i) who needs to perform the behaviour? (ii) what does the person need to do differently to achieve the desired change? (iii) when will they do it? (iv) where will they do it? (v) how often will they do it? (vi) with whom will they do it? Being more or less specific is the difference between ‘eating healthier foods’ and ‘Lou will eat no more than two cream cakes per week for the next 3 months.’ Being more specific about which behaviour(s) we are trying to change allows us to be more focussed when it comes to understanding these behaviours.
Identify what needs to change. We expect any medical intervention to have been based on a diagnosis and the diagnosis to be based on a thorough examination (or analysis) of the problem. The same is true of designing interventions to change behaviour. To change behaviour we need to understand why behaviours are as they are and what needs to shift for the desired behaviour to occur. Answering these questions is helped by a model of behaviour, the COM-B model( Reference Khaw, Wareham and Bingham 2 , Reference Michie, van Stralen and West 6 ). The initials stand for capability, opportunity, motivation and behaviour. According to the model, behaviour is part of an interacting system involving all these components. Each component is divided into two types. Capability is divided into physical (having the physical skills, strength or stamina to perform the behaviour) or psychological (having the knowledge, psychological skills, strength or stamina to perform the behaviour). Opportunity is divided into physical (what the environment allows or facilitates in terms of time, triggers, resources, locations, physical barriers, etc.) or social (including interpersonal influences, social cues and cultural norms). Motivation is divided into reflective (involving self-conscious planning and evaluations (beliefs about what is good or bad)) or automatic (processes involving emotional reactions, desires, impulses and reflex responses).
If more detail is needed to understand the behaviour, the COM-B model components can be further elaborated using the Theoretical Domains Framework (TDF)( Reference Cane, O'Connor and Michie 7 ). The TDF is made up of fourteen domains synthesised from 128 constructs taken from thirty-three theories of behaviour and behaviour change: knowledge; skills; memory, attention and decision processes; behavioural regulation; social/professional role and identity; beliefs about capabilities; optimism; beliefs about consequences; intentions; goals; reinforcement; emotion; environmental context and resources; and social influences. Explicit links between TDF domains and the COM-B model are given in the BCW Guide( Reference Michie, Atkins and West 2 ).
Using the COM-B model and/or TDF intervention designers can make a behavioural diagnosis of what needs to shift in order for the desired behaviour to occur. The COM-B model has been used in the development of two mobile applications to promote healthy eating behaviours( Reference Curtis, Lahiri and Brown 8 , Reference Robinson, Higgs and Daley 9 ). One application was designed to support parents of overweight children in providing appropriate portion sizes across the five food groups( Reference Curtis, Lahiri and Brown 8 ). The intervention designers ran focus groups with parents of overweight children and asked about their capability, opportunity and motivation to provide appropriate portion sizes. Parents responses to the focus group questions resulted in the following behavioural diagnosis: psychological capability needed to shift as parents reported a lack of knowledge and monitoring of appropriate food portion sizes and difficulty understanding food packaging portion guidelines; reflective motivation needed to shift as parents were not confident in their ability to provide correct portion sizes; social opportunity needed to shift as partners were not always supportive of efforts to provide appropriate portion sizes and continued to give too big portion sizes. A questionnaire and an interview schedule have been developed to support intervention designers in making a behavioural diagnosis( Reference Michie, Atkins and West 2 ).
Identify intervention options
Having made a behavioural diagnosis, the next step is to begin building the intervention. A systematic review identified nineteen frameworks to guide intervention design and rated them according to whether they were comprehensive, coherently structured and linked to a model of behaviour( Reference Michie, van Stralen and West 6 ). None met all the criteria so the frameworks were synthesised and the resulting integrated framework was the BCW (Fig. 2). The BCW is composed of the COM-B model at the hub of the wheel, nine intervention functions form the inner ring and seven policy categories form the outer ring of the wheel. Since its publication in 2011, the original paper reporting the BCW( Reference Michie, van Stralen and West 6 ) has been accessed over 59 000 times and cited over 150 times. In addition to being used to understand and change eating behaviours two case studies in the BCW Guide show how it has been used to improve paediatric health care in Kenya( Reference English 10 ) and promote adherence to guidelines for post-natal depression( Reference Hanbury, Farley and Thompson 11 ).

Fig. 2. (Colour online) The Behaviour Change Wheel( Reference Michie, Atkins and West 2 ).
Identify intervention functions. Intervention functions are broad categories of means by which an intervention can change behaviour. The nine intervention functions resulting from the synthesis of nineteen frameworks are provided in Table 1. The term ‘function’ is used rather than ‘type’ or ‘category’ as an intervention may have more than one function. For example, a mass media campaign to promote healthy eating may contain an element that is educational (providing new information on the benefits of healthy eating) but also be presented in a way that is intended to be persuasive (generating feelings of worry about the health harms of eating high fat foods). Thus it would be unhelpful to classify the mass media campaign as either educational or persuasive; it would be more accurate to say that it served both educational and persuasive functions.
Table 1. Behaviour Change Wheel intervention functions

Explicit links between the COM-B model and intervention functions suggest which functions are likely to be effective in bring about the desired change based on the behavioural diagnosis (Table 2). For example, if the behavioural diagnosis to increase healthy eating in adults in the workplace identified that they were not prioritising doing this; this would be coded as reflective motivation. According to the COM-B model/intervention function matrix, there are several functions that could potentially bring about a shift in reflective motivation (as denoted by the shaded cells). These are education, persuasion, incentivisation or coercion. Which of these functions might be most appropriate depends on a number of contextual factors. The APEASE criteria( Reference Michie, Atkins and West 2 ) has been developed to support intervention designers in making context-based decisions by considering the following criteria: (i) affordability (can it be delivered on budget?) (ii) practicality (is it feasible to deliver?) (iii) effectiveness and cost-effectiveness (does it work?) (iv) acceptability (is it acceptable to those receiving/delivering it and at a political level?) (v) side-effects/safety (are there any unintended side-effects or safety issues?) (vi) equity (does it advantage some groups over others?).
Table 2. Matrix of links between capability, opportunity, motivation and behaviour (COM-B) model and intervention functions

Using the COM-B/intervention function matrix and the APEASE criteria allows designers to be systematic and take account of context in their selection of intervention functions.
Identify policy categories. Seven policy categories sit on the outer layer of the BCW (see Table 3 for labels, definitions and examples). These policy categories allow the consideration of not only what function the intervention will serve but how the intervention will be delivered.
Table 3. Behaviour Change Wheel policy categories

Explicit linkages between intervention functions and policy categories are given Table 4.
Table 4. Matrix of links between intervention functions and policy categories

Continuing the example in the previous step: if the intervention function persuasion were selected to change the target population's reflective motivation so they prioritised healthy eating in the work place, policy categories that could potentially deliver that intervention function would be communication/marketing, guidelines, regulation, legislation and service provision. Applying the APEASE criteria will help designers to select the most appropriate for the context in which the intervention will be delivered.
Identify implementation options
Identify behaviour change techniques. Having selected which functions an intervention will serve and which policy categories are most appropriate to deliver those functions, designers now need to select the behaviour change techniques (BCT) that will bring about the desired change. BCT are defined as the ‘active ingredients’ in an intervention designed to bring about change. Examples of BCT include: goal setting (behaviour), defined as setting or agreeing a goal defined in terms of the behaviour to be achieved, e.g. agree a daily goal to eat fresh fruit and vegetables at lunch and dinner; self-monitoring of behaviour, defined as establishing a method for the person to monitor and record their behaviour(s) as part of a behaviour change strategy, e.g. asking the person to record daily, in a diary, whether they had eaten fresh fruit and vegetables at lunch and dinner each day. The recently developed Behaviour Change Technique Taxonomy v1 (BCTTv1)( Reference Michie, Richardson and Johnston 12 ) is composed of ninety-three BCT. The BCW Guide describes how each BCT is linked to intervention functions and provides a short-list of potential BCT. Designers are again encouraged to use the APEASE criteria to help select from this short-list the most appropriate BCT for their context. The BCTTv1 is available as an application( Reference Michie, Richardson and Johnston 12 ) and the UCL Centre for Behaviour Change has recently launched free online training to use the taxonomy (www.bct-taxonomy.com).
Identify mode of delivery. In addition to intervention content, designers need to decide on the mode of delivery for the intervention, for example, whether the intervention will be delivered face-to-face either to groups or individuals or by website, mobile application, print media to list a few of the options. A simple taxonomy of modes of delivery is provided in the BCW Guide. The sample principles apply here as in previous steps: be comprehensive and consider all available options to deliver the intervention and be systematic and use the APEASE criteria to judge which mode of delivery is most appropriate for the context.
Implementation
The present paper has described a method of designing interventions in the context of changing eating behaviours using tools recently developed in behavioural science. The tools and method described here are, of course, applicable to a wide range of behaviours in a variety of contexts and there are common challenges in implementing behaviour change interventions. Two key challenges are discussed briefly here: (1) Implementing an intervention to change behaviour in a particular group is likely to depend on changing behaviour of those delivering the intervention. For example, implementing an intervention in primary care to change eating behaviours in patients with diabetes is reliant on primary care staff (general practitioners, practice nurses and health care assistants) changing their behaviour in order to deliver the intervention. Identifying and addressing barriers and facilitators to health professional change will support implementation. (2) Related to the previous point is the issue of fidelity of intervention delivery. That is, the extent to which interventions are delivered as planned. Monitoring fidelity of delivery is encouraged in Medical Research Council Guidance on intervention development and evaluation( Reference Craig, Dieppe and Macintyre 4 ) and promotes accurate interpretation of outcomes and identification of provider training needs( Reference Lorencatto, West and Christopherson 13 ).
Summary
The key benefit of using the BCW and the BCTTv1 is that they encourage intervention designers to be comprehensive in considering all options to intervene and then to systematically select those that are most promising for the context. It is not a ‘magic bullet’ but a system for making the best use of the understanding and resources available to arrive at a behaviour change intervention.
As these technologies, the BCW and BCTTv1, are relatively new, there are currently few examples of effective interventions developed using them. However, the BCW and BCTTv1 can be retrofitted to existing reports of existing interventions to better characterise their functions and specify active ingredients. This will permit a more coherent synthesis of the evidence and identification of interventions most effective in different populations and settings.
For further information on BCW training, talks and workshops please visit the UCL Centre for Behaviour Change website (www.ucl.ac.uk/behaviour-change).
Financial Support:
None.
Conflicts of Interest:
None.
Authorship:
Both authors contributed equally to all aspects of preparation of this paper.






