



On 17 October, 2021, we lost a true giant in the fields of cardiac anatomy and development. The name of Lodewyk H.S. van Mierop, known universally as “Bob” (Fig 1), Reference Van Mierop1 is likely less well known to those working in the current era. In the formative years of paediatric cardiology and paediatric cardiac surgery, however, he was one of the innovators. Many, if not most, of his works retain their value. Until recently, those who might have chosen to consult the Netter Atlas would have seen the results of his investigations, but even that masterpiece is now somewhat dated. Frank Netter was a great friend of Bob, and the illustrations of Netter of the temporal changes taking place during normal cardiac development were based on the original drawings made by van Mierop. Reference Van Mierop and Netter2 These original drawings made by van Mierop, in turn, were based on van Mierop’s own assessment of serially sectioned human embryos, with his descriptions being well ahead of their time. van Mierop used these studies to provide an account of the results of abnormal development of the atrioventricular junctions, which he continued to describe as persistent atrioventricular canal. Reference Van Mierop, Alley and Kausel3 As an extension of this work, he provided a remarkable early account of the surgical approach to the so-called “cleft mitral valve”, Reference Van Mierop and Alley4 which we now recognise as the zone of apposition between the left ventricular components of the bridging leaflets of the common atrioventricular valve. van Mierop also provided an accurate account of the development of the outflow tract, Reference Van Mierop, Alley and Kausel5 relating this analysis to the lesions reflecting “abnormal transfer” of the pulmonary trunk, Reference Van Mierop and Wiglesworth6 and so-called “true” transposition. Reference Van Mierop and Wiglesworth7 In his subsequent studies, working with Donald F. Patterson from University of Pennsylvania, van Mierop described the changes to be observed in the abnormal outflow tracts of Keeshond dogs, providing an accurate description of the morphogenesis of common arterial trunk. Reference Van Mierop, Patterson and Schnarr8–Reference Van Mierop and Patterson10 These studies, in themselves, would be enough to place Bob in the pantheon of our Paediatric Cardiology Hall of Fame. They represent, however, but a small part of his overall achievements.

Figure 1. Bob van Mierop, on the right, is shown with two of the authors of this article (Bob Anderson on the left and Jay Fricker in the centre) in the Conference Room at University of Florida in Gainesville. His drawings showing the features of the “asplenia syndrome and polysplenia syndrome” can be seen on the wall behind. These figures were drawn in 1972, and show the obvious features of right isomerism and left isomerism, respectively.
Bob was born on 31 March, 1927, in Surabaya, Java. At that time, Java was part of the Netherlands East Indies. He spent the first 18 years of his life in Java. He provided a graphic account of these years in his autobiography. Reference Van Mierop1 It was not entirely plain sailing, since the period from 1942, up to his move to Holland in 1946, was spent as a guest of the occupying Japanese empire. He was required to catch up rapidly with his education, having moved with his mother and his stepfather to Europe, but as he comments in his autobiography, his brain was “not too shabby”. He was able to gain entrance to Leiden University, where he managed to shorten the time required for graduation as a physician. He had seen, during these studies, advertisements in the Lancet, offering the chance to study in the Medical College of Albany, in New York State. Having completed his medical degree in Leiden, he applied, and was accepted, for training in Thoracic Surgery.
It was on the initial boat trip from Rotterdam to New York that he acquired his pseudonym “Bob”, named after the bartender, since two young ladies he and his friend were accompanying at the time could not cope with “Lodewyk”. Reference Van Mierop1 In this regard, the family name itself was originally “vanMierop”. Once in North America, the spelling was transformed to van Mierop. This is how his name appears on all of his publications and how he stated it on his Curriculum Vitae.
In Albany, he encountered the first of his mentors, Ralph Alley. Working first as an Assistant Resident, then as a Research Fellow, subsequently as a Research Associate and Instructor, and culminating as a rotating Internist, he spent six happy and fruitful years in Albany.
He then spent a period of 3 years working at Montreal Children’s Hospital, also becoming a Lecturer in Anatomy at McGill University. During this period, he made a major breakthrough, being perhaps the first to recognise the features of right isomerism in the setting of so-called “asplenia syndrome” (Fig 2). Reference Van Mierop and Wiglesworth11,Reference Van Mierop, Patterson and Reynolds12 In 1962, he returned to Albany as Assistant Professor in Pediatric Cardiology. During this second stint in Albany, he established an important collaboration with Murray Barron, a radiologist working at Mount Sinai in New York. Reference Baron, Wolf and Steinfeld13 He was promoted whilst in Albany to Associate Professor, but his achievements by then had brought him into contact with Gerold Schiebler, who rapidly established himself as his second major mentor. Although Bob’s basic training had been in Cardiac Surgery, Dr. Schiebler was able to tempt him to join University of Florida in Gainesville as a Paediatric Cardiologist. More importantly, he was given responsibility for the autopsy service investigating the deaths of those with congenitally malformed hearts. Schiebler also ensured that Bob would have the facilities to continue his developmental studies.
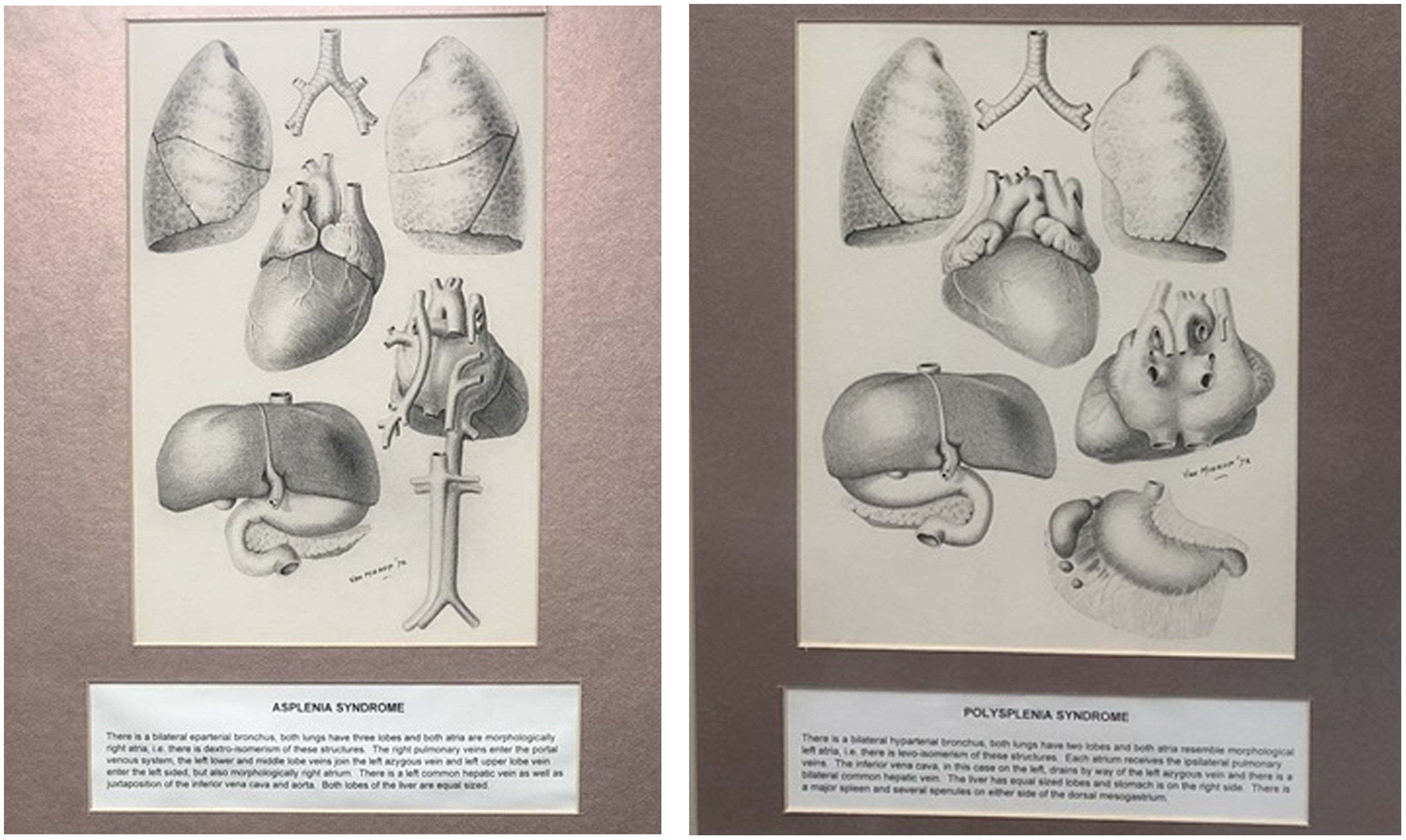
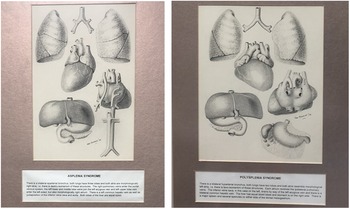
Figure 2. These drawings of Professor van Mierop, made by him in 1972, and shown in greater detail in Figures 3 and 4, are located in the Conference Room at University of Florida in Gainesville. As is explained in the legends to Figures 3 and 4, these drawings demonstrate the features of “asplenia syndrome” and “polysplenia syndrome” and show the obvious features of right isomerism and left isomerism, respectively, including the isomeric features of the lungs, bronchuses, and atrial appendages.
Thus started his association with University of Florida, which continued for the remainder of his life (Figs 3, 4, 5, 6, 7, 8, 9, 10 and 11). Although now ostensibly working as a Paediatric Cardiologist, he still retained his surgical skills. Should the situation demand, he was ready to step into the operating room to lend his hand to his surgical colleagues. It was shortly after his arrival in Gainesville that he became embroiled in the infamous polemic with Richard Van Praagh regarding the appropriate definition for “transposed” arterial trunks. At the time, Bob was of the opinion that an anterior location of the aortic root was a prerequisite for the definition of “transposition”. He set out his stall in uncompromising fashion. Reference Van Mierop14 His commentary was prompted by Richard’s suggestion that the essence of transposition was the origin of the arterial trunks from inappropriate ventricles. This suggestion meant that, on rare occasions, it was entirely appropriate to define transposition in the presence of a posteriorly located aortic root, provided that the aortic root took its origin from the morphologically right ventricle. Reference Van Praagh, Perez-Trevino and Lopez-Cuellar15 Richard then defended his own viewpoint in equally uncompromising fashion. Reference Van Praagh16 In many ways, Bob’s stance had been swayed by his friendship and collaboration with Maria Victoria de la Cruz, another giant in the field of cardiac development. In this regard, it is noteworthy that Maria Victoria subsequently came to appreciate the need to differentiate between the connections of the arterial trunks and their relationships. Reference de la Cruz, Arteaga and Espino-Vela17 We were never sure whether Bob also saw the need to move from his initial stance.
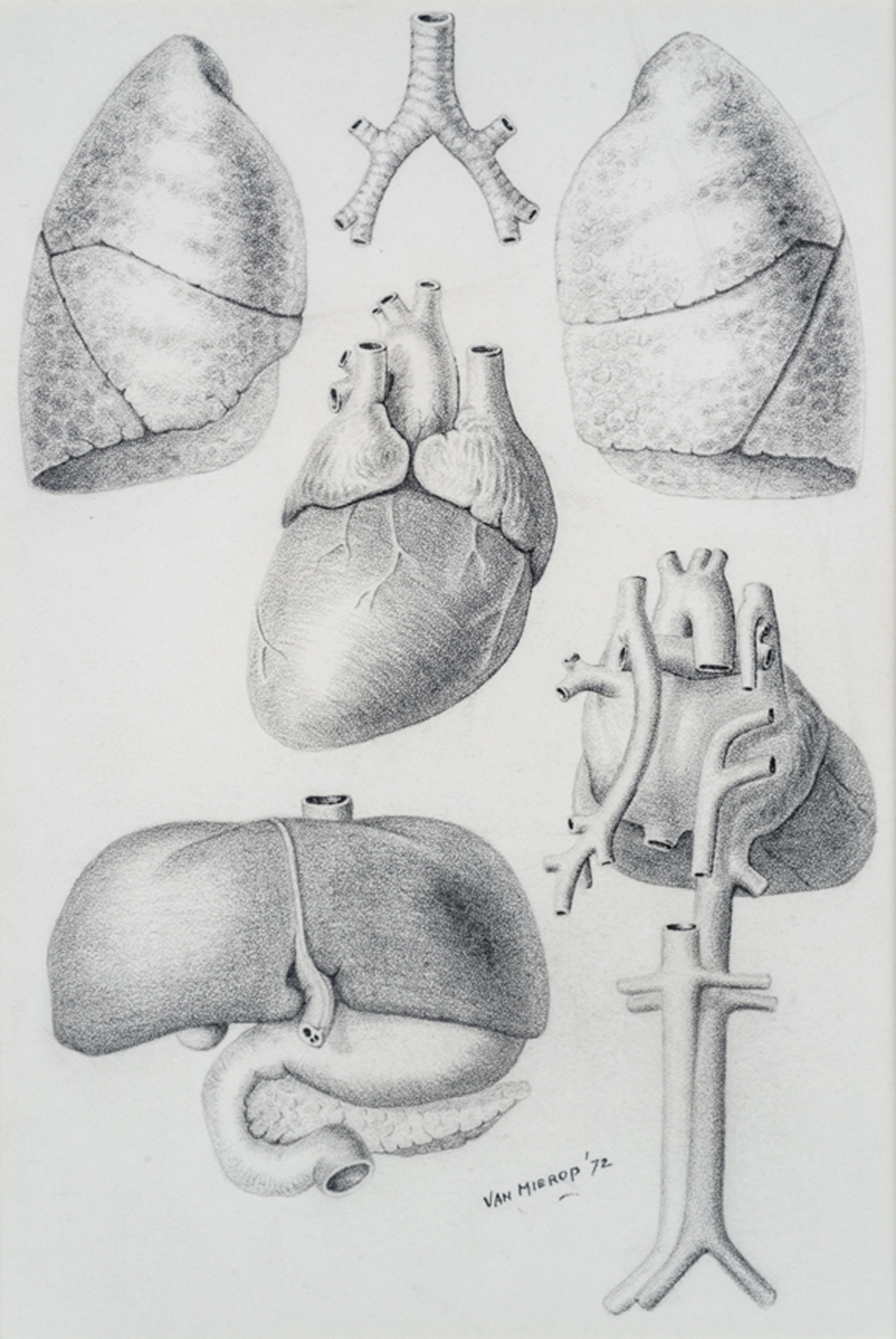
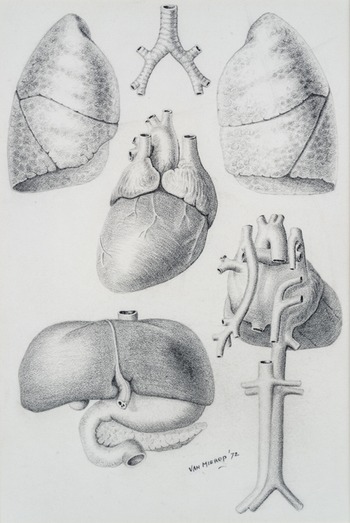
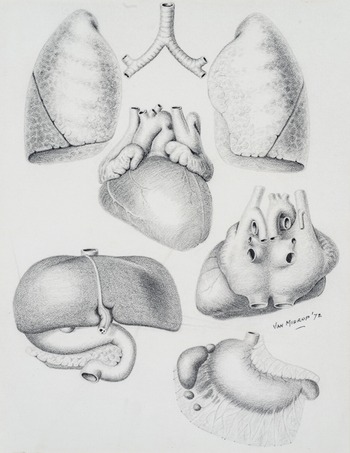
Figure 3. This drawing done in 1972 from The University of Florida van Mierop Heart Archive demonstrates the features of Asplenia Syndrome. There is a bilateral eparterial bronchus, both lungs have three lobes and both atriums are morphologically right atriums, i.e., there is dextro-isomerism of these structures. The right pulmonary veins enter the portal venous system, the left lower and middle lobe veins join the left azygous vein and the left upper lobe vein enters the left sided, but morphologically right atrium. There is a left common hepatic vein as well as juxtaposition of the inferior vena cava and aorta. Both lobes of the liver are equal sized.
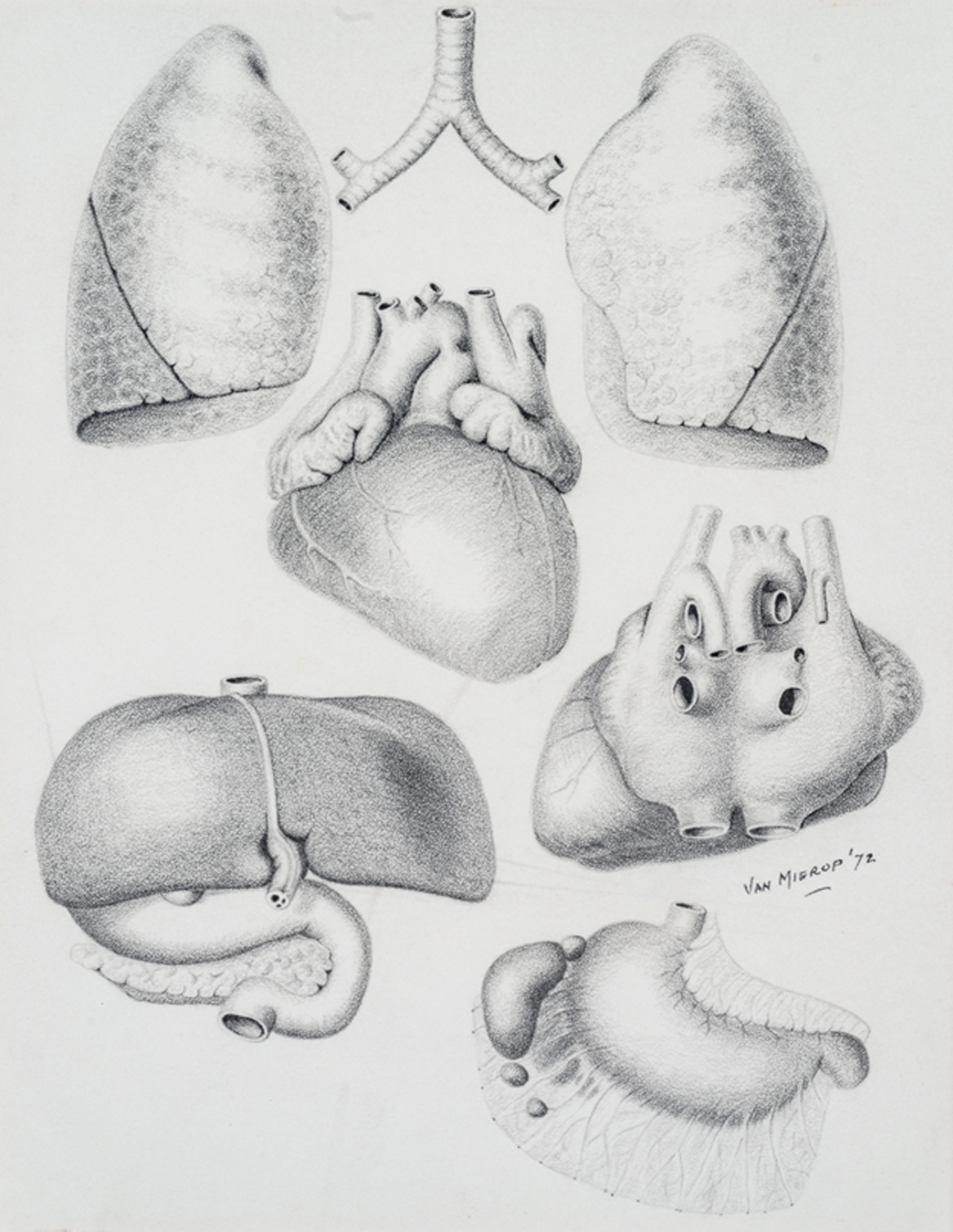
Figure 4. This drawing done in 1972 from The University of Florida van Mierop Heart Archive demonstrates the features of Polysplenia Syndrome. There is a bilateral hyparterial bronchus, both lungs have two lobes and both atriums resemble morphologically left atriums, i.e., there is levo-isomerism of these structures. Each atrium receives the ipsilateral pulmonary veins. The inferior vena cava, in this case on the left, drains by way of the left azygous vein and there is a bilateral common hepatic vein. The liver has equal sized lobes and the stomach is on the right side. There is a major spleen and several spenules on either side of the dorsal mesogastrium.

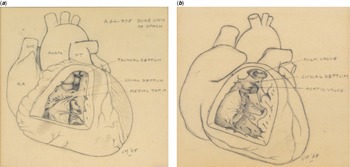
Figure 5. This set of drawings done in 1965, and now housed in The University of Florida van Mierop Heart Archive, shows the features of “two anomalies with similar clinical and hemodynamic features, but different anatomy”. ( a ) Panel A shows an example described at the time as a “Truncal Tet”. We would now describe the lesion as showing a doubly committed and juxta-arterial ventricular septal defect with a fibrous rather than a myocardial outlet septum. van Mierop emphasises the bicuspid pulmonary valve, and shows a normal medial papillary muscle. ( b ) Panel B shows the more typical variant of tetralogy of Fallot, with an anteriorly malaligned myocardial outlet septum. The medial papillary muscle is absent in this specimen, as is often the case in the setting of tetralogy of Fallot. (PT = pulmonary trunk; PULM VALVE = Pulmonary Valve; RA = right atrium; SVC = superior vena cava)
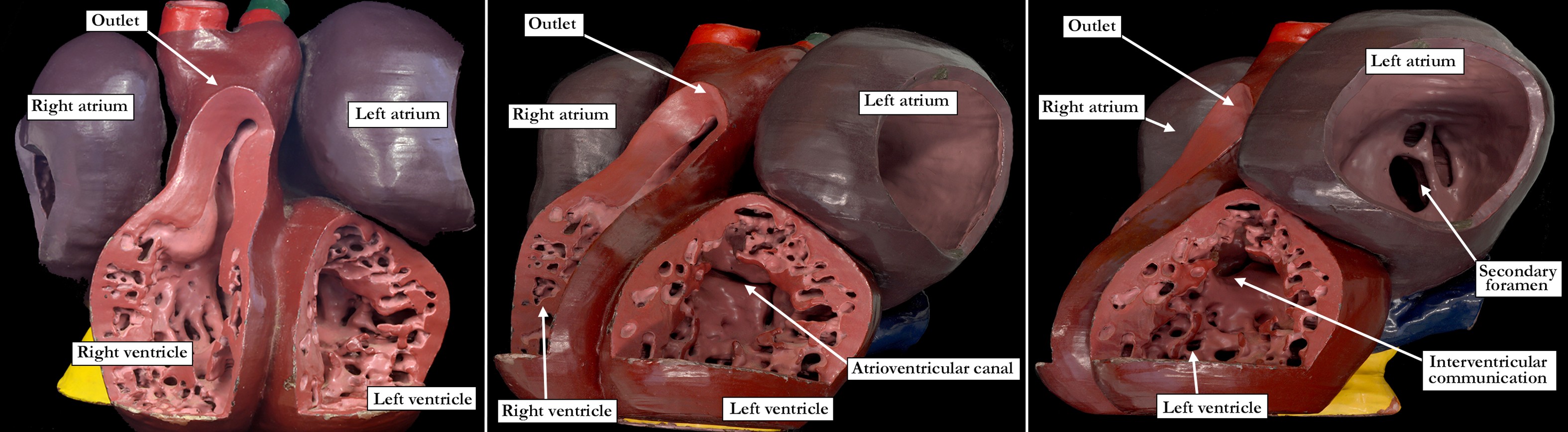
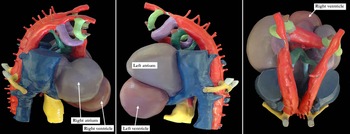
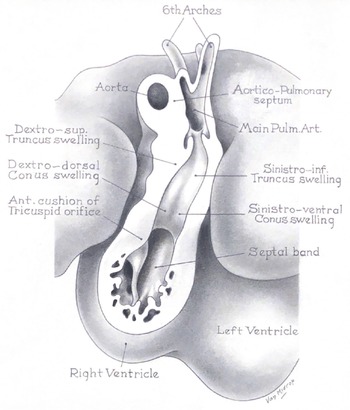
Figure 6. The panels show wax plate reconstructions from serially sectioned human embryos approximately from Carnegie stages 13 to 14. The three panels are from the same reconstruction and are rotated to show the different developmental features. The left panel is an anterior view showing the apical right ventricle ‘ballooning’ from the outlet component of the ventricular loop. The middle panel is rotated rightward and tilted to show the developing atrioventricular canal. The right panel is rotated even farther to show the embryonic interventricular communication.
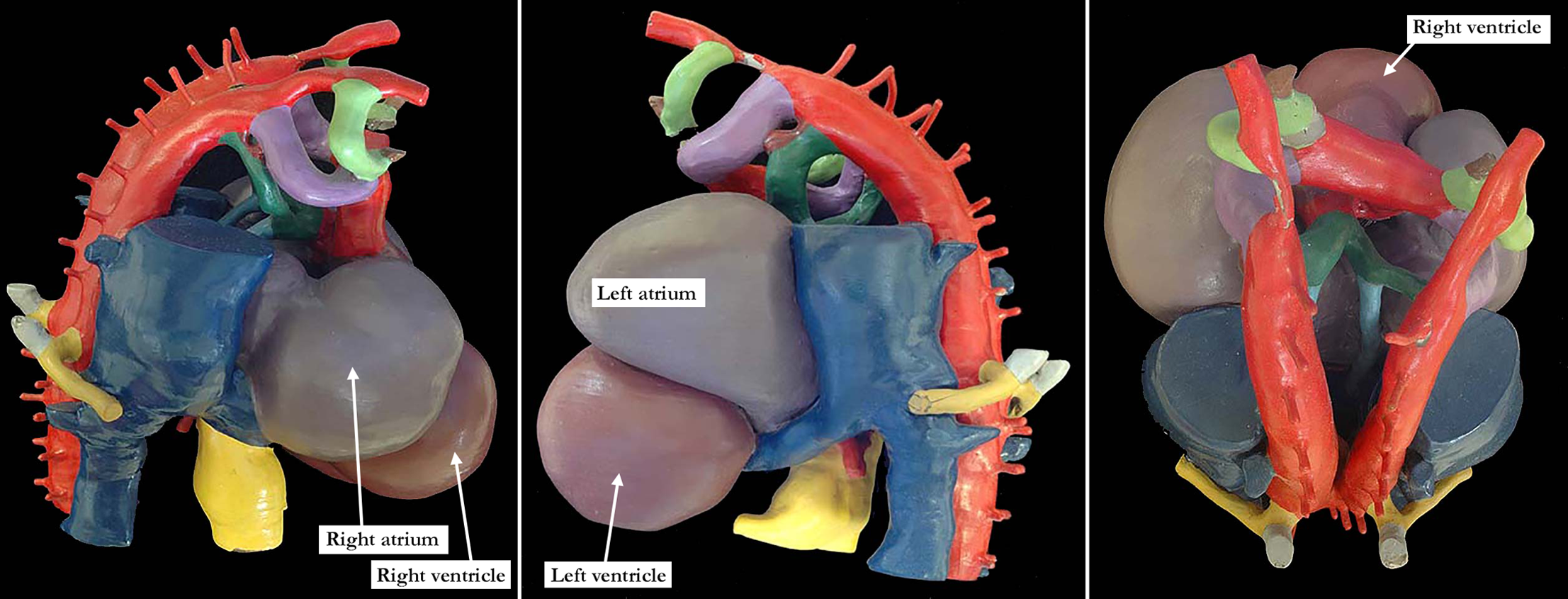
Figure 7. The panels show wax plate reconstructions from serially sectioned human embryos at Carnegie stage 14, demonstrating the developing aortic arch system. The aortic arches are red with the left panel shown from the right, the middle panel shown from the left, and the right panel as a posterior view. The lime green structure is the 3rd arch, the purple structure is the 4th arch and the dark green structure the 6th arch. Photographs of this wax plate appeared as Figure 8 in a 2013 publication by Simon D. Bamforth and colleagues that included Professor Lodewyk H.S. van Mierop and Professor Robert H. Anderson as coauthors. The legend of this Figure 8 stated: “Fig. 8. Wax plate reconstruction of a developing human embryo. Bilateral collateral channels between the dorsal components of the fourth (4) and sixth (6) arch arteries are visible on the right (a) and left (b). The collateral channels, shown in the insets, are colored brown. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]”. (Bamforth SD, Chaudhry B, Bennett M, Wilson R, Mohun TJ, van Mierop LH, Henderson DJ, Anderson RH. Clarification of the identity of the mammalian fifth pharyngeal arch artery. Clin Anat. 2013 Mar;26(2):173-82. doi: 10.1002/ca.22101. Epub 2012 May 23. PMID: 22623372.)

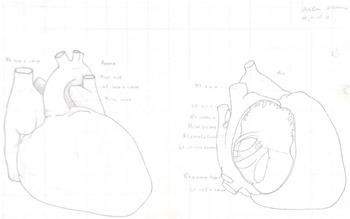
Figure 8. The University of Florida van Mierop Heart Archive contains multiple cardiac morphological specimens, as well as multiple original line diagrams and wax models produced by Professor van Mierop, including this original line drawing.

Figure 9. The University of Florida van Mierop Heart Archive contains multiple cardiac morphological specimens, as well as multiple original line diagrams and wax models produced by Professor van Mierop, including this original line drawing.
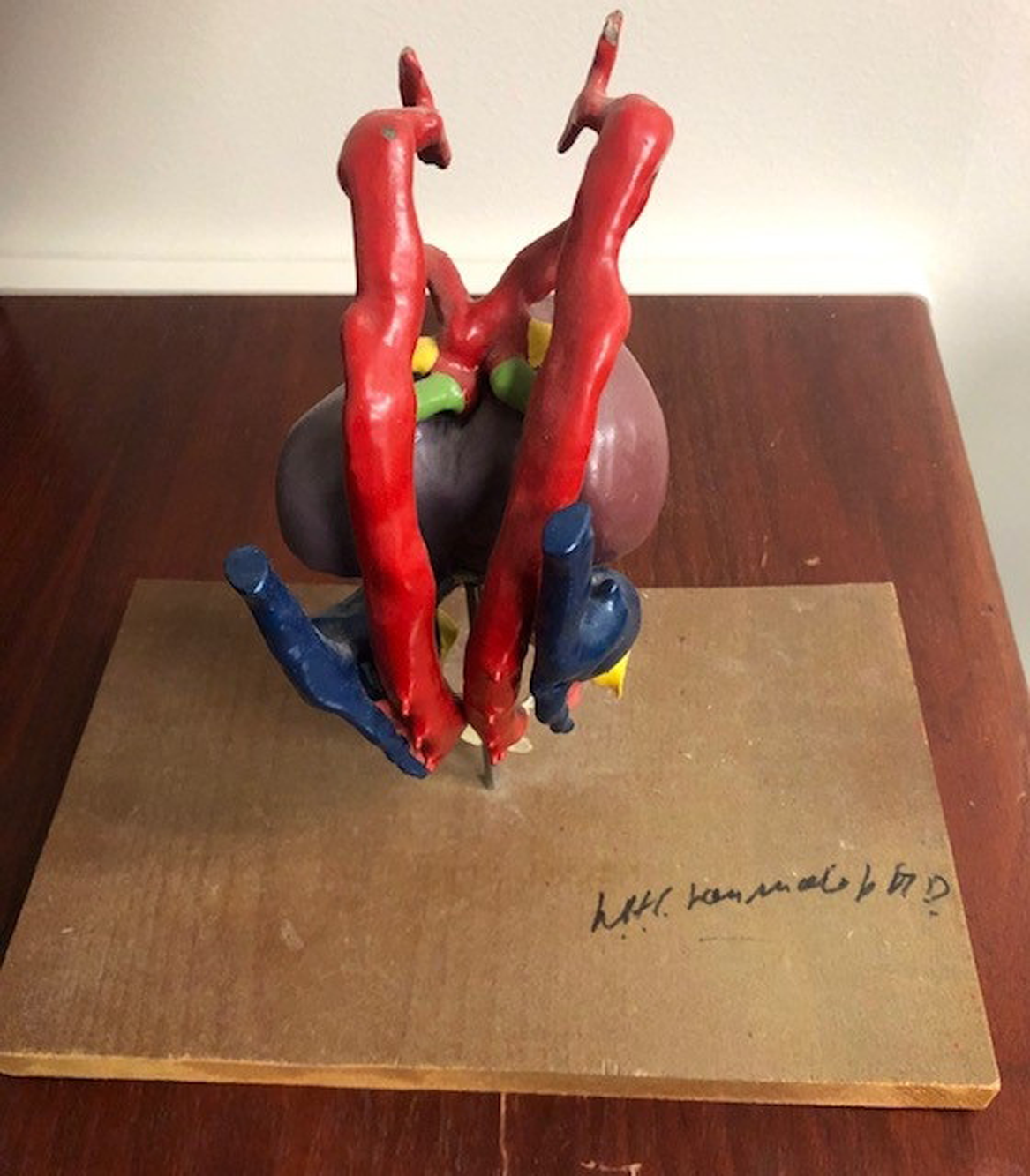
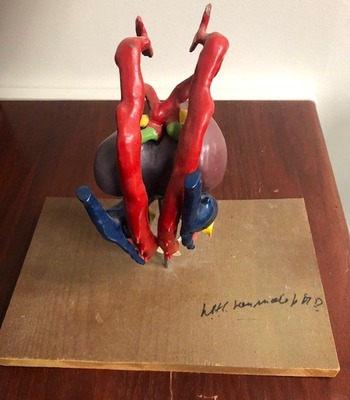
Figure 10. The University of Florida van Mierop Heart Archive contains multiple cardiac morphological specimens, as well as multiple original line diagrams and wax models produced by Professor van Mierop, including this original wax model.

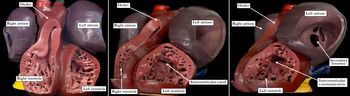
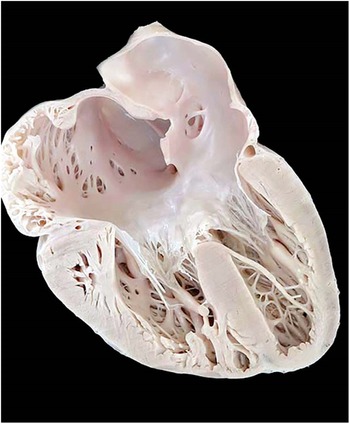
Figure 11. The University of Florida van Mierop Heart Archive contains multiple cardiac morphological specimens, as well as multiple original line diagrams and wax models produced by Professor van Mierop, including this cardiac morphological specimen. This image shows a specimen of atrioventricular septal defect with common atrioventricular junction sectioned by Bob van Mierop to replicate the four-chamber echocardiographic cut. This heart is representative of the amazing specimens within The University of Florida van Mierop Heart Archive housed at the Congenital Heart Center at University of Florida in Gainesville, Florida, United States of America.
During his tenure at University of Florida in Gainesville, Bob continued to build on his reputation as a cardiac anatomist and embryologist, establishing important collaborations with Patterson, to which we have already referred. He was also on hand to offer important advice to Peggy Kirby as she began her own important investigations on the role of the neural crest in normal and abnormal formation of the outflow tracts. Reference Besson, Kirby and Van Mierop18 His own specific investigations of these topics continued, with important contributions made with Lynne Kutsche. Reference Kutsche and Van Mierop19–Reference Kutsche and Van Mierop21 He also provided important mentoring for Rebecca Snider, who made very important contributions in paediatric echocardiography. The fact that, throughout his career, he was thinking way ahead of the next person is demonstrated by the achievements of his sabbatical period. He took the opportunity to visit centres throughout Europe and the rest of the World, producing a coding system for the overall group of congenitally malformed hearts. Reference Van Mierop22,Reference Van Mierop23 His system is very much the forerunner of the latest system that is named The International Paediatric and Congenital Cardiac Code (IPCCC) [https://ipccc.net/], which has become the paediatric and congenital cardiac component of the Eleventh Revision of the International Classification of Diseases (ICD-11). Reference Jacobs, Franklin and Jacobs24–Reference Jacobs, Franklin and Béland30
Over and above his huge contributions in the fields of cardiac anatomy, embryology, and congenital cardiac care, Bob also established himself as a world-class herpetologist. Those who were fortunate to dine with him were somewhat taken aback to be seated in a Dining Room in the van Mierop home framed by cages containing rattlesnakes and pythons, which on occasion would make their presence known by tapping on the glass of their cages. Not surprisingly, his expertise was often called for in the setting of rattlesnake bites, when his knowledge of the distance between the fang marks was sufficient to predict the size of the animal in question.
Bob rose in the administrative ranks at University of Florida, serving as Chief of the Division of Pediatric Cardiology in Gainesville. For a short period, he was also Chair of the Department of Pediatrics (Fig 12). On allegedly “retiring” from active duty in 1995, University of Florida honoured him with the distinction of Emeritus Professor. Far from retiring, however, he continued to play his part in the Division, providing the benefit of his huge knowledge and expertise. Dr. Bob remained the voice of reason, providing evidence and logic as the data were interpreted and clinical decisions made. He provided regular weekly teaching sessions for the students, Residents, and Fellows in paediatric cardiology well into his 80s. Those who attended these sessions continue to recognise and frequently mention his dedication, along with the tremendous impact that he had on their future. Professor van Mierop imparted embryologic and anatomic knowledge interspersed with many stories of his life experiences, all of which they fondly remember.
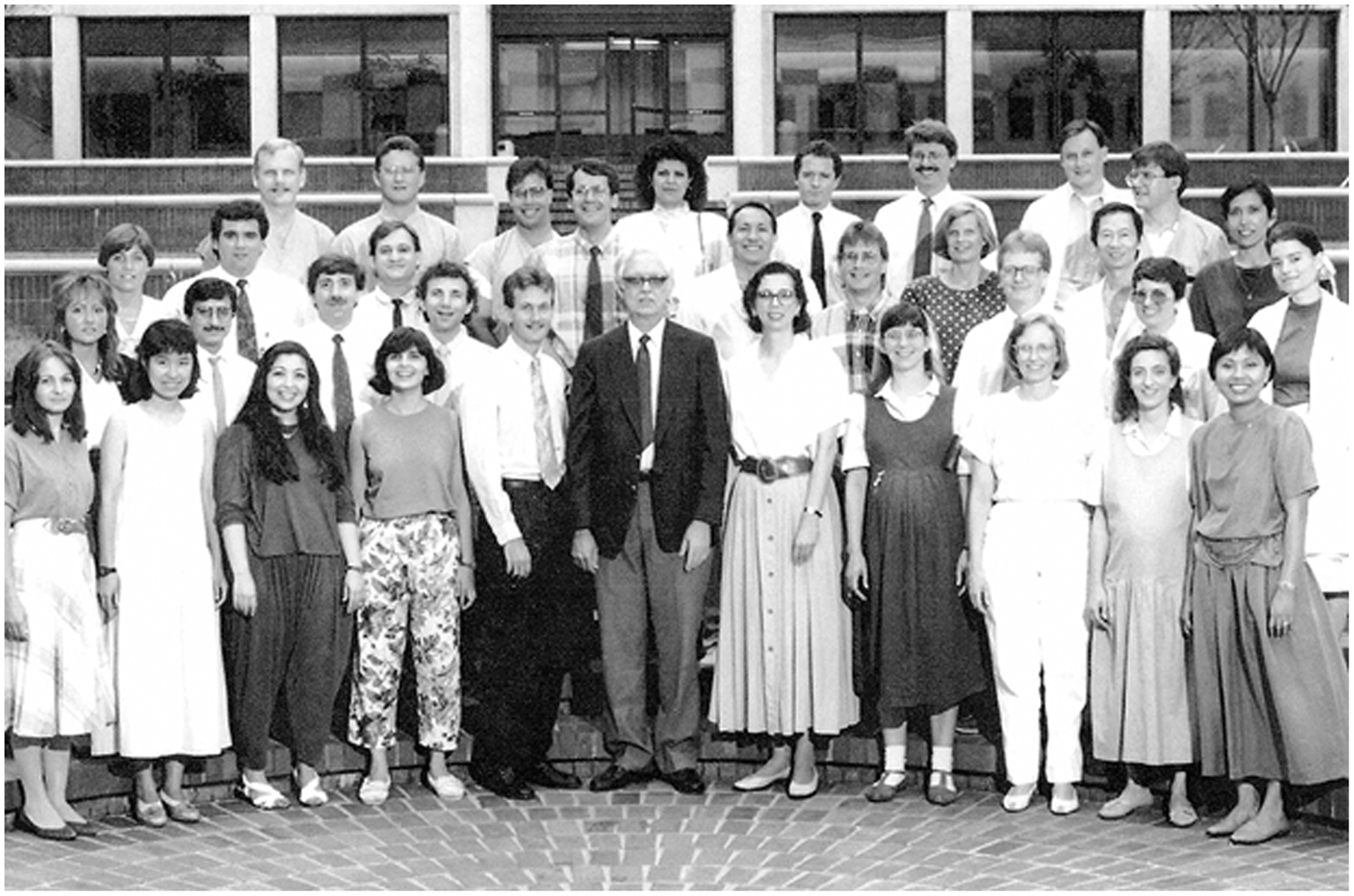
Figure 12. This photograph was taken during the time when Bob van Mierop served as Chair of Pediatrics at University of Florida in Gainesville, Florida, United States of America. He is front and centre, in the black jacket. Lynne Kutsche stands to his left hand.
The students, Residents, Fellows, and faculty at University of Florida are all indebted to Professor van Mierop for decades of teaching and training. It is a fact that the diagnostic tools that he trained with did not initially include the basic and more advanced forms of imaging that we all take for granted today. However, the faculty at University of Florida distinctly remember his enthusiasm and encouragement to us as we strived to introduce these new technologies and further push the boundaries of these modalities at University of Florida. Professor van Mierop would regale us with tales of his interactions with various individuals, the names of whom adorn various procedures that we use commonly now. He made special mention of his interactions with Giancarlo Rastelli (1933–1970), a Cardiac Surgeon and creator of the Rastelli classification of atrioventricular septal defects, as well as the Rastelli procedure, who unfortunately died of cancer at 36 years of age. The faculty at University of Florida also fondly remember the dialogue and lively debates between Professor Lodewyk H.S. van Mierop and Professor Robert H. Anderson during the annual visits of the latter to Gainesville, debates which could in themselves be a source for academic reading. Most of all, however, the faculty at University of Florida fondly recall the over-arching care for the University of Florida Congenital Heart Center and its members provided by Professor van Mierop, and this leadership and support will never be forgotten.
Reflections from the family of Lodewyk H.S. van Mierop
Family was of tremendous value to Bob van Mierop (Figs 13 and 14). His family provided us with the following text, entitled: “ Story about Dad’s favorite hobby ” (Provided by Juliana Koca, daughter of Bob van Mierop):
Many people knew our father as a renowned Paediatric Cardiologist. A man with a passion for science and nature and a unique point of view on medicine.
But he also had many hobbies and interests outside of medicine, including raising exotic orchids, fishing, woodworking, and collecting antique firearms.
But, by far, his most interesting, and sometimes scary, hobby was his interest in snakes (Fig 15). When we moved to Florida, Dad decided to show us all which snakes were harmless and which ones were poisonous. After that, the collection began. It started with a harmless yellow rat snake he found in our back yard. He placed it in a small terrarium and from then on, snakes were his passion and the collection grew larger over the years. Dad used his carpentry skills to build elaborate cages for the snakes with running water and plants, and our home became somewhat of a reptile zoo with over 60 snakes occupying our home and back porch! Later, he became quite an expert on the treatment of venomous snake bites.
Many times, at dusk, we accompanied him to Wacahoota Road – a remote area near Paynes Prairie Preserve State Park, just to go snake hunting. (Paynes Prairie Preserve State Park is a Florida State Park, encompassing a 21,000-acre savanna in Alachua County, Florida, United States of America, lying between Micanopy and Gainesville. It is also a United States of America National Natural Landmark.) Snakes were very common on that road, and Dad knew how to capture them safely and bring them home. Sometimes, we would keep them for a long time, other times we would set them free a short time later. Over time, the snake collection became more exotic, including boa constrictors, pythons, green tree pythons, and, for a very short time, a cobra – which our mom insisted he get rid of immediately!
My siblings and I will never forget those years of Dad’s snake hobby. Many years later, people would still ask, “Do you still have all those snakes?” And we would fondly remember the man who made our lives so much more interesting.
-
From: Lizabeth Craig, Diana Latta, Bobby van Mierop, Juliana Koca, Pete van Mierop

Figure 13. The van Mierop Family. Photograph provided by Juliana Koca, daughter of Bob van Mierop, “Just for old times’ sake…”.

Figure 14. The van Mierop Family. Photograph provided by Juliana Koca, daughter of Bob van Mierop, “Photograph taken probably around 2010. Left to right: Robert (Bobby), Diana, Dad, Lizabeth, Mom, Juliana, Pete”.
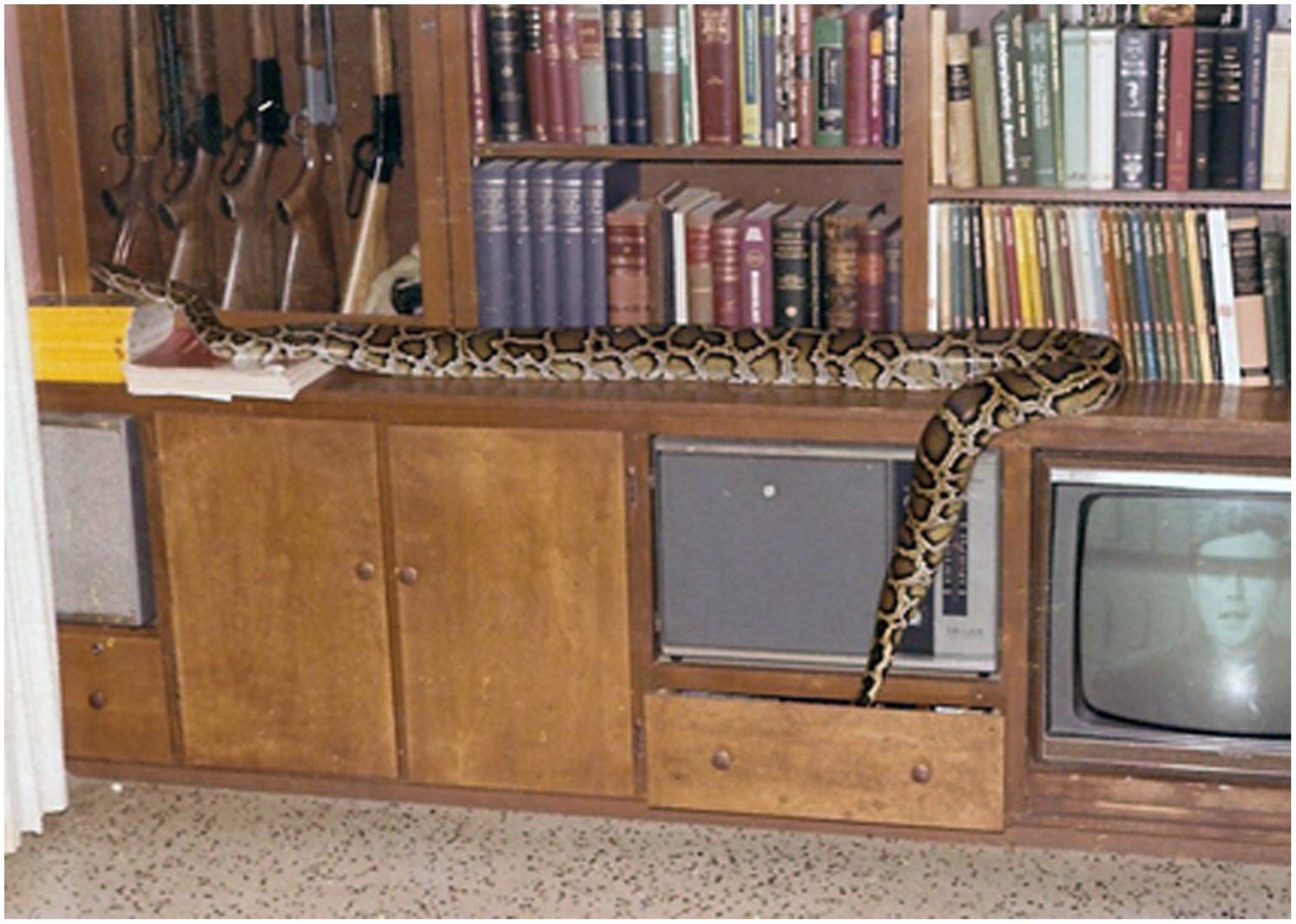
Figure 15. This photograph from the van Mierop family collection shows one of the snakes from the collection of Bob van Mierop. Those who were fortunate to dine with Bob van Mierop were somewhat taken aback to be seated in a dining room framed by cages containing rattlesnakes and pythons, which on occasion would make their presence known by tapping on the glass of their cages.
Final thoughts
In the final analysis, Bob’s detailed examination of the heart, and his skill as an anatomist, were unsurpassed in the contribution to our knowledge and understanding of paediatric cardiac care (Fig 11). Even to the very end, he was assertive in defending his own position, no matter how entrenched that position might be. He was always ready, nonetheless, to accept the new evidence and to change his mind once convinced of the validity of the opposing viewpoint. In this regard, he was the epitome of the true physician scientist. It is these features, and the evidence that remain from his writings and illustrations, along with the contents of The University of Florida van Mierop Heart Archive he established and maintained, which will serve as his enduring legacy. Undoubtedly, with these extraordinary contributions to the fields of cardiac anatomy and embryology, which were way ahead of his time, Dr. van Mierop was a true giant in Paediatric Cardiology (Figs 16 and 17). The invaluable archive he established at University of Florida in Gainesville, The University of Florida van Mierop Heart Archive, has been instrumental in teaching medical students, Residents, Medical Fellows, and Surgical Fellows. Only a handful of similar archives exist across the globe, and these archives are the true legacy of giants such as Dr. van Mierop. We have an important obligation to leave no stone unturned to continue to preserve these archives for the future generations of surgeons, physicians, all providers of paediatric and congenital cardiac care, and, most importantly, our patients.
Figure 16. Photograph of the front cover of the truly fascinating and multi-dimensional autobiography of Professor Lodewyk H.S. van Mierop entitled “Doctor Bob”: Reference Van Mierop1 van Mierop LHS. Doctor Bob. Denver, Colorado; Outskirts Press Inc., 2013.
Figure 17. This photograph from the van Mierop family collection pictures Bob van Mierop and demonstrates his true love of nature. Over and above his huge contributions in the fields of cardiac anatomy, embryology, and congenital cardiac care, Bob van Mierop also established himself as a world-class herpetologist.
Acknowledgements
The authors of this paper and the University of Florida Congenital Heart Center acknowledge the following three friends and professional colleagues of Professor Lodewyk H.S. van Mierop who all made massive and awesome contribution to University of Florida and paediatric and congenital cardiac care: Gerold L. Schiebler, MD, his late wife, Mrs. Audrey Lincourt Schiebler, and Ms. Deborah Floyd.
Dr. van Mierop would always remind his faculty about the importance of providing due recognition to all members of the TEAM, and he particularly highlighted the singular contribution of Ms. Deborah Floyd. Debbie was the administrative anchor for the Division of Pediatric Cardiology at University of Florida for over 30 years. In addition to her extensive administrative duties and tasks related to management of the Pediatric Cardiology Fellowship at University of Florida, Debbie even assisted Dr. van Mierop in the 1980’s in collecting the snakes he would incubate in his lab as part of his embryological research. At the recent retirement dinner in honour of Debbie Floyd, held at the home of Dr. and Mrs. Jay Fricker on Saturday, February 19, 2022, multiple graduates of the Pediatric Cardiology Fellowship at University of Florida who now practice all across the United States of America, as well as current Pediatric Cardiology Fellows at University of Florida, all honoured Debbie and paid tribute to her tremendous and awesome contributions to University of Florida and the community of paediatric and congenital cardiac care.
Gerold L. Schiebler, MD, recruited Professor Lodewyk H.S. van Mierop to join University of Florida. The University of Florida Congenital Heart Center acknowledges the tremendous contributions of Gerold L. Schiebler, MD, and his late wife, Mrs. Audrey Lincourt Schiebler [https://www.uff.ufl.edu/giving-opportunities/008049-gerold-l-schiebler-m-d-and-audrey-lincourt-schiebler-childrens-advocacy-fellowship-in-pediatrics/].
Dr. Schiebler is a graduate of Harvard Medical School and a Professor Emeritus and a Distinguished Service Professor of the Department of Pediatrics at University of Florida. Born in 1928 to German immigrant parents, Dr. Schiebler was raised in Hamburg, Pennsylvania, United States of America. He graduated from Harvard Medical School in 1954 and joined the University of Florida Department of Pediatrics faculty in 1960, becoming the first Paediatric Cardiologist in North Florida. In 1968, Dr. Schiebler was named Chair of the University of Florida Department of Pediatrics. He became University of Florida Associate Vice President for Health Affairs for External Relations in 1985. Dr. Schiebler founded the Division of Children’s Medical Services within the State’s Department of Health and Rehabilitative Services, and established specialised medical services at the University of Florida Health Center for women undergoing high-risk pregnancies.
Mrs. Schiebler was born in Newport, Rhode Island, United States of America, and graduated from the Newport Hospital School of Nursing. After moving to Gainesville in 1960, Mrs. Schiebler became a distinguished volunteer of Florida. She served as President of the University of Florida Medical Guild, Medical Auxiliary, and Junior League of Gainesville. For 20 years, she acted as the Vice Chair of The Ounce of Prevention Fund of Florida. From 1987 to 2000, Mrs. Schiebler worked for University of Florida’s Institute for Child Health Policy. Mrs. Schiebler was awarded the Medal of Honor by the Florida Bar Foundation in 1990. She was a Florida Blue Key Honorary Member, and an honorary Fellow of the American Academy of Pediatrics. She and Dr. Schiebler were married for 61 years and had six children and 17 grandchildren. Mrs. Schiebler passed away in 2015.
Financial support
None.
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.



 Open access
Open access