



Cardiovascular complications are the leading cause of morbidity and mortality in type 1 diabetes mellitus. Reference Laing, Swerdlow and Slater1 Cardiovascular disease is more common in the later stages of type 1 diabetes mellitus and is rare in childhood. However, early detection and treatment of these serious complications of type 1 diabetes mellitus reduce morbidity and mortality in patients. Reference Donaghue, Marcovecchio and Wadwa2
Real-time three-dimensional echocardiography (known as four-dimensional echocardiography) and speckle-tracking echocardiography are newly developed echocardiographic techniques used to evaluate left ventricular systolic function, global and regional myocardial deformation or strain, and detect early left ventricular systolic dysfunction in different cardiac pathologies. Reference Voigt and Cvijic3–Reference Čelutkienė, Plymen and Flachskampf5 Many studies investigated its role in detecting subclinical left ventricular systolic dysfunction in adult patients with diabetes mellitus, but studies are scarce, and the results of these studies are contradictory in paediatrics. Reference Fang, Leano and Marwick6–Reference Yoldaş, Örün and Sagsak10 This study aimed to evaluate the role of real-time three-dimensional (four-dimensional) echocardiography and speckle-tracking echocardiography for early detection of subclinical left ventricular systolic dysfunction in asymptomatic children with type 1 diabetes mellitus.
Materials and method
Study population
This cross-sectional case–control study was performed in a single centre between March and September 2019. The sample size was calculated with an effect size of 0.75, an alpha of 0.05, and a power of 0.85, and it was found 35 patients were needed in each group. The study included 38 consecutive children with type 1 diabetes mellitus who were followed in the Pediatric Endocrinology Outpatient Clinic, and 38 age, gender, and body measurements matched healthy children. Each patient underwent an interview about medical history, a detailed clinical examination, blood laboratory tests, as well as echocardiography. Type 1 diabetes mellitus was defined according to the American Diabetes Association Criteria. Reference Ernande, Rietzschel and Bergerot7 Patients under the age of 21 with a diagnosis of type 1 diabetes mellitus for at least 5 years were eligible for inclusion in the study. Patients with chronic disease other than type 1 diabetes mellitus, congenital/acquired heart disease, chronic complications of type 1 diabetes mellitus, using another drug regularly other than insulin, obesity (body mass index Z score > +2 standard deviation), and poor echocardiographic images were excluded from the study. Two patients and one control patient were excluded from the study because of poor echocardiographic images. Age, sex, weight, and height were recorded; body surface area (Haycock formula) and body mass index [the ratio of weight to height squared (kg/m2)] were calculated for all patients. Blood pressure and heart rate were measured with a digital device (A&N Medical, London, England) consecutively three times after 10 minutes resting period. Those with a body mass index >2SD and hypertension were excluded from the study because obesity and hypertension may affect speckle-tracking echocardiographic measurements. The study complies with the World Health Medical Association Declaration of Taipei on Ethical Considerations Regarding Health Databases and Biobanks. The study protocol was approved by the local ethics committee (A-47, 08.05.2018), and written informed consent was obtained from all patients and/or their legal guardians before enrolment.
Echocardiographic assessment
Transthoracic echocardiography was performed with an appropriate transducer interfaced with Philips IE 33 ultrasound system (Philips Healthcare, Inc., Andover, Massachusetts, United States of America) by the same experienced echocardiographer. Each patient was evaluated with two-dimensional; M-mode; colour, pulse, and continuous-wave Doppler echocardiography, and tissue Doppler imaging, according to the American Society of Echocardiography guidelines. Reference Lopez, Colan and Frommelt12
Three-dimensional echocardiographic images were recorded during 4–6 cardiac cycles and end-expiratory breath hold by X5-1 matrix array transducer. Frame rates of the images were 15–30 frames/second. Data were digitally stored and analysed offline by Tomtec 2.0 four-dimensional left ventricular function software (GmbH, Unterschleissheim, Germany). Manual editing after an automated tracking method was used so that trabecula, papillary muscles, and ventricular bands were accepted as part of the ventricular cavities. Left ventricular end-diastolic and systolic volume; ejection fraction; global longitudinal, circumferential, and radial strain; twist; and torsion were measured. Volume measurements were adjusted for body surface area and expressed as mL/m2. Investigators were blinded to the clinical findings of the patients. The amount of myocardial deformation (positive or negative strain) is expressed in %. Positive strain values describe thickening, negative values describe shortening, of a given myocardial segment related to its original length. During myocardial contraction, as the wall shortens it also thickens and thus assessment of all parameters, longitudinal shortening (negative strain), circumferential shortening (negative strain), and radial thickening (positive strain), is useful for the evaluation of contractile function. Left ventricular rotation, twist, and torsion, due to the complex helical myocardial fibre architecture, are the result of the clockwise rotation of the base and the counterclockwise rotation of the apex of the left ventricle. The left ventricular twist was defined as the net difference between the basal and apical rotation angles. Left ventricular torsion was calculated as the net left ventricular twist normalised with respect to the ventricular end-diastolic longitudinal length between the left ventricular apex and the mitral plane (left ventricular torsion (°/cm) = left ventricular twist/left ventricular end-diastolic longitudinal length).
This study aimed to evaluate the role of real-time three-dimensional echocardiography (known as four-dimensional echocardiography) and three-dimensional speckle-tracking echocardiography for the early detection of subclinical left ventricular systolic dysfunction in asymptomatic children with type 1 diabetes mellitus.
Statistical analysis
SPSS v.21 (SPSS Inc., Chicago, Illinois, United States of America) was used for statistical analysis. Results were presented as the mean and standard deviation for normally distributed variables and median and interquartile range for non-normally distributed variables. Comparisons of the groups for continuous variables were made using the independent t-test or Mann–Whitney U test, according to whether normally distributed or not. Categorical variables were presented as frequencies and percentages, and a chi-square test was used to compare categorical variables. Pearson correlation analysis was used for normally distributed continuous variables, and Spearman correlation analysis for non-normally distributed continuous variables. In order to determine intra-observer and inter-observer variability, 30 cases (15 patients and 15 controls) were randomly selected. Image analysis was repeated by the same observer one month after the first analysis for intra-observer variability and a second observer for inter-observer variability on the same cardiac cycle. Observers were blinded to the previous measurements. Intra-observer and inter-observer variability were assessed using intra-class correlation. In SPSS, the reliability analysis with a two-way random model and absolute agreement [intra-class correlation (2.1)] were chosen to determine intra-class correlation. An intra-class correlation coefficient ≥0.75 indicated good reproducibility, 0.40–0.75 moderate reproducibility, and <0.40 poor reproducibility. The significance level was set at p < 0.05.
Results
Study population
Clinical and laboratory findings of the study population are presented in Table 1. Patients and controls were matched for general characteristics. There were no statistically significant differences between the patient and control groups regarding age, gender, weight, height, body surface area, and body mass index. The mean age at diagnosis and duration of the disease for type 1 diabetes mellitus was 6.7 ± 2.9 years and 8.7 ± 2.2 years, respectively. The mean serum glycosylated haemoglobin level (HbA1C) was higher in the patient group (8.4% versus 5.4%).
Table 1. Clinical and laboratory findings of the study population

Data are expressed as mean ± standard deviation, median (interquartile range), or n (%).
Bold font style represents statistically significant differences.
* Student t-test;
** Chi-square;
*** Mann–Whitney U test.
Conventional echocardiography and tissue Doppler imaging
Table 2 shows the conventional echocardiography and tissue Doppler imaging parameters of patients with type 1 diabetes mellitus and healthy controls. There was no statistically significant difference between the patients and controls concerning the left ventricular ejection fraction, fractional shortening, E/E', and S'. However, the E/A and E'/A' ratios in patients were lower than that in controls (1.7 ± 0.3 versus 1.9 ± 0.3, p = 0.002, and 2.2 ± 0.4 versus 2.7 ± 0.6, p < 0.001).
Table 2. Conventional echocardiography and tissue Doppler imaging parameters of the study population

Data are expressed as mean ± standard deviation or median (interquartile range).
Bold font style represents statistically significant differences.
EF = ejection fraction; FS = fractional shortening.
* Student t-test;
** Mann–Whitney U test.
Real-time three-dimensional (four-dimensional) and three-dimensional speckle-tracking echocardiography
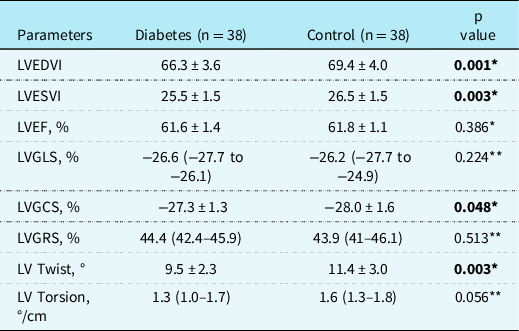
Table 3 shows real-time three-dimensional (four-dimensional) and three-dimensional speckle-tracking echocardiographic parameters of the study population. There was no statistically significant difference between the patients and controls with respect to the left ventricular ejection fraction and global longitudinal and radial strain. However, the left ventricular global circumferential strain in patients was significantly lower than in controls [(−27.3% ± 1.3) versus (−28% ± 1.6), p = 0.048]. Left ventricular twist in patients was also significantly lower than in controls (9.5 ± 2.3 versus 11.4 ± 3.0, p = 0.003). Although left ventricular torsion was lower in patients than in controls [1.3 (1.0–1.7) versus 1.6 (1.3–1.8)], the difference was not statistically significant (p = 0.056). Left ventricular end-diastolic and end-systolic volume indexes of the patients were lower than in controls.
Table 3. Real-time three-dimensional (four-dimensional) and three-dimensional speckle-tracking echocardiographic parameters of the study population
Data are expressed as mean ± standard deviation or median (interquartile range).
Bold font style represents statistically significant differences.
LV = left ventricle; LVEDVI = left ventricular end-diastolic volume index; LVEF = left ventricular ejection fraction; LVESVI = left ventricular end-systolic volume index; LVGCS = left ventricular global circumferential strain; LVGLS = left ventricular global longitudinal strain; LVGRS = left ventricular global radial strain.
* Student t-test;
** Mann–Whitney U test.
Correlation analysis
No correlation was noted between the left ventricular global longitudinal, circumferential, and radial strain and serum glycosylated haemoglobin levels (r = 0.030, r = −0.148, r = 0.040, respectively, p > 0.05 for all) and diabetes duration (r = 0.003, r = −0.066, r = 0.040, respectively, p > 0.05 for all).
Inter-observer and intra-observer reliability were excellent for all the left ventricular parameters (Table 4).
Table 4. Intra-class correlation coefficient between observers

LV = left ventricle; LVEDVI = left ventricular end-diastolic volume index; LVEF = left ventricular ejection fraction; LVESVI = left ventricular end-systolic volume index; LVGCS = left ventricular global circumferential strain; LVGLS = left ventricular global longitudinal strain; LVGRS = left ventricular global radial strain.
Discussion
This study evaluated left ventricular systolic function and myocardial deformation in asymptomatic children with type 1 diabetes mellitus by conventional echocardiography, tissue Doppler imaging, real-time three-dimensional (four-dimensional) echocardiography, and three-dimensional speckle-tracking echocardiography. The left ventricular systolic function was shown as preserved by conventional and tissue Doppler echocardiography in our patients. Our study showed decreased left ventricular global circumferential strain and twist by three-dimensional speckle-tracking echocardiography in asymptomatic children with type 1 diabetes mellitus. The left ventricular global longitudinal and radial strains of our patients were similar to healthy children. There are a considerable number of clinical studies using two-dimensional and three-dimensional speckle-tracking echocardiography in adults with type 1 and type 2 diabetes mellitus. Reference Fang, Leano and Marwick6–Reference Jędrzejewska, Król and Światowiec8,Reference Biswas, Sudhakar and Nanda13–Reference Ringle, Dornhorst, Rehman, Ruisanchez and Nihoyannopoulos17 Many of these studies showed longitudinal strain impairment in adult diabetes mellitus patients. Reference Enomoto, Ishizu and Seo15–Reference Ringle, Dornhorst, Rehman, Ruisanchez and Nihoyannopoulos17 It is generally agreed that left ventricular longitudinal dysfunction appears to be an early manifestation of diabetic cardiomyopathy in adults. The underlying mechanism of the longitudinal dysfunction has been proposed to be due to subendocardial damage. Radial contractility appears to compensate for reduced longitudinal contractility in subclinical left ventricular dysfunction. Reference Fang, Leano and Marwick6 Therefore, changes in the other myocardial deformation components are less well established and depend on the disease stage. In more advanced stages of the disease, a decrease of systolic strain in all directions could be seen due to further progression of the diabetic cardiomyopathy. Reference Ernande, Rietzschel and Bergerot7–Reference Altun, Babaoğlu, Binnetoğlu, Özsu, Yeşiltepe Mutlu and Hatun9 Ringle et al. evaluated the progression of left ventricular dysfunction in asymptomatic type 1 diabetes mellitus adult patients by two-dimensional and three-dimensional speckle-tracking echocardiography. They found a mild decrease in left ventricular global longitudinal strain. On the contrary, neither left ventricular global circumferential nor radial strain was unchanged at the base and during follow-up. Reference Ringle, Dornhorst, Rehman, Ruisanchez and Nihoyannopoulos17 Luis et al. demonstrated strong correlations between left ventricular global longitudinal, circumferential, and radial strain and left ventricular ejection fraction by two-dimensional and three-dimensional speckle-tracking echocardiography. Reference Luis, Yamada and Khandheria14 However, the strongest correlation for left ventricular ejection fraction in their cohort was left ventricular global circumferential strain. They postulated that the predominance of circumferential fibres over longitudinal fibres within the myocardial wall makes these fibres the primary determinant of left ventricular myocardial function. Furthermore, Matsumoto et al. demonstrated that left ventricular global circumferential strain was superior to left ventricular global longitudinal strain in determining contractile reserve during dobutamine stress. Reference Matsumoto, Tanaka and Kaneko19 Cho et al. reported that left ventricular global circumferential strain was a more powerful predictor of adverse cardiac events than left ventricular global longitudinal strain or left ventricular ejection fraction in heart failure patients. Reference Cho, Marwick, Kim, Kim, Hong and Oh20
There are a limited number of studies by speckle-tracking echocardiography in children with type 1 diabetes mellitus, and these studies’ results are contradictory. Altun et al. found significantly lower left ventricular global longitudinal and radial strain values of the left ventricle by two-dimensional speckle-tracking echocardiography in asymptomatic children with type 1 diabetes mellitus and normal left ventricular ejection fraction. Reference Altun, Babaoğlu, Binnetoğlu, Özsu, Yeşiltepe Mutlu and Hatun9 Also, Yoldas et al. showed that left ventricular global longitudinal, circumferential, and radial strain by two-dimensional speckle-tracking echocardiography were significantly lower in children with type 1 diabetes mellitus. Reference Yoldaş, Örün and Sagsak10 However, Hensel et al. showed no statistically significant difference for left ventricular global longitudinal and circumferential strain by two-dimensional speckle-tracking echocardiography between type 1 diabetes mellitus and healthy children neither at rest nor during exercise. Reference Hensel, Grimmer, Roskopf, Jenke, Wirth and Heusch21 Kaushig et al reported that left ventricular regional strain indices and flow-mediated dilatation were impaired in asymptomatic children and adolescents with type 1 diabetes mellitus despite absence of overt heart failure and normal ejection fraction. Reference Kaushic, Kapoor and Dabatghao11 The only available data about three-dimensional speckle-tracking echocardiographic values in children with type 1 diabetes mellitus to compare with us revealed a significant decrease in all three strains, including global longitudinal, circumferential, and radial strain in the patient group. Reference El Razaky, El Amrousy, Elrifaey, Elgendy and Ibrahim22 Their patients are younger, and diabetes duration is shorter than our patients, differences may be due to technical differences.
Three-dimensional speckle-tracking echocardiography can also quantify rotational movements such as twist and torsion of the left ventricle. Reference Luis, Yamada and Khandheria14,Reference El Razaky, El Amrousy, Elrifaey, Elgendy and Ibrahim22 Left ventricular twist was decreased in our patients. Previous reports based on tissue Doppler imaging, two-dimensional speckle-tracking echocardiography, or MRI found either preserved or increased twist and torsion in adults with diabetic cardiomyopathy. Reference Kaku, Takeuchi and Tsang23–Reference Vasanji, Sigal and Eves25 A three-dimensional speckle-tracking echocardiography study in children with type 1 diabetes mellitus showed preserved twist and torsion, but their patients are younger, and diabetes duration is shorter than our patients. Reference El Razaky, El Amrousy, Elrifaey, Elgendy and Ibrahim22
We did not find a significant correlation between the left ventricular strain parameters and serum glycosylated haemoglobin levels or type 1 diabetes mellitus duration. This may be due to better glycaemic control and shorter duration of diabetes of our patients. There has been an ongoing discussion about the association between diabetes mellitus and heart failure in adult patients, if it is an independent association or related to concomitant risk factors, like coronary artery disease, hypertension, or unknown factors. An almost linear increase in heart failure risk is observed with elevation in serum glycosylated haemoglobin levels. Reference Stratton, Adler and Neil26 In a meta-analysis, four key independent risk factors were identified: history of coronary artery disease, age, poor glycaemic control, and hypertension. Reference Wang, Negishi, Negishi and Marwick27 As heart failure secondary to diabetes mellitus is almost never seen in the pediatric population, these data could not be extrapolated to our population, but early predictors of heart failure could be determined by strain echocardiography. Nakai et al. demonstrated that global longitudinal strain was significantly lower in the adult type 2 diabetes mellitus group with longer disease duration. Reference Nakai, Takeuchi, Nishikage, Lang and Otsuji18 El Razaky et al. showed a significant decrease in all strain components in children with type 1 diabetes mellitus, but that decrease did not correlate with the duration of diabetes mellitus. Reference El Razaky, El Amrousy, Elrifaey, Elgendy and Ibrahim22
We found normal range but lower transmitral E/A ratios and mitral annular E'/A' ratios among patients with type 1 diabetes mellitus; however, E/E' ratios were similar in the patients and healthy children. These findings may show diastolic function is affected in these patients.
Limitations
Conducting the study in asymptomatic paediatric patients with a narrow range of ages with type 1 diabetes mellitus who have not yet been adequately investigated by real-time three-dimensional (four-dimensional) echocardiography and three-dimensional speckle-tracking echocardiography and measurement of left ventricular contraction, strain, and rotation together are the strengths of our study. This study has some limitations also. The study design was cross-sectional and did not include follow-up information. We believe it would be more useful to follow the patients and evaluate the results obtained after long-term follow-up.
Conclusion
We found that even in children with asymptomatic type 1 diabetes mellitus with normal left ventricular ejection fraction, left ventricular circumferential function was impaired and rotation pattern was changed by real-time three-dimensional echocardiography and three-dimensional speckle-tracking echocardiography. This novel echocardiographic method might be an important tool for detecting left ventricular systolic dysfunction in type 1 diabetes mellitus patients before it becomes overt on conventional echocardiography and tissue Doppler imaging.
Acknowledgements
We kindly thank the patients, the controls, and their families who participated in the study.
Financial support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by Cerrahpaşa Medical Faculty Ethic Committee (A-47, 08.05.2018). A written informed consent was taken from all patients and their legal guardians.





 Open access
Open access