


Introduction
Certain rhythmic arterial pressure waves in humans and animals have been noticed since the early 19th century. Reference Guyton and Statterfield1–Reference Carroll4 These waves have distinctive frequencies, ranging from 0.006 to 1 Hz (the period ranging from 1 to 60 s). Reference Carroll4 They may be physiological or pathophysiological, with different underlying causes, such as heartbeat, respiration, sudden circulatory changes (i.e., Mayer waves), and spleen volume change (i.e., spleen waves). Reference Carroll4 The implications and mechanisms of these waves, particularly the last two, remain unclear. For example, some argued that Mayer waves, were merely an epiphenomenon of normal baroreflex operation without a particular function since it can be found in healthy humans, while others suggested that it could trigger the liberation of nitric oxide and thus benefit the end-organ function in situations like sudden circulatory changes and cerebral ischaemia, etc. Reference Julien5 To our knowledge, similar arterial pressure waves have not been found in children with CHD undergoing cardiovascular surgery.
Our centre has systematically assessed haemodynamics using the pressure recording analytical method by MostCare, Reference Romagnoli, Bevilacqua and Lazzeri6 combining with cerebral (ScO2) and renal (SrO2) oxygen saturation and perfusion using near-infrared spectroscopy Reference Steiner, Pfister, Strebel, Radolovich, Smielewski and Czosnyka7 and transcranial Doppler and brain injuries using electroencephalogram perioperatively in children with CHD for two years. The monitoring modalities, MostCare and near-infrared spectroscopy, have been modified to generate and transfer successive raw data with a 6-second interval simultaneously in one computer. We analysed these raw data initially aiming at examining the cerebral autoregulation or its loss at low arterial pressure in CHD patients. Reference Brady, Mytar and Lee8 Unexpectedly, we found the arterial pressure waves with hitherto unreported frequency in some patients at much higher arterial pressures.
In this study, we examined the incidence and characteristics of the waves and their clinical implications by analysing their relations with systemic haemodynamic and cerebral oxygenation and injury measures.
Patients and methods
Patients
After the institutional ethics approval (No.46201) and informed consent obtained, we examined the prospectively recorded raw monitoring data of 212 children with CHD (Table 1) undergoing cardiovascular surgery between September 2019 and August 2021.
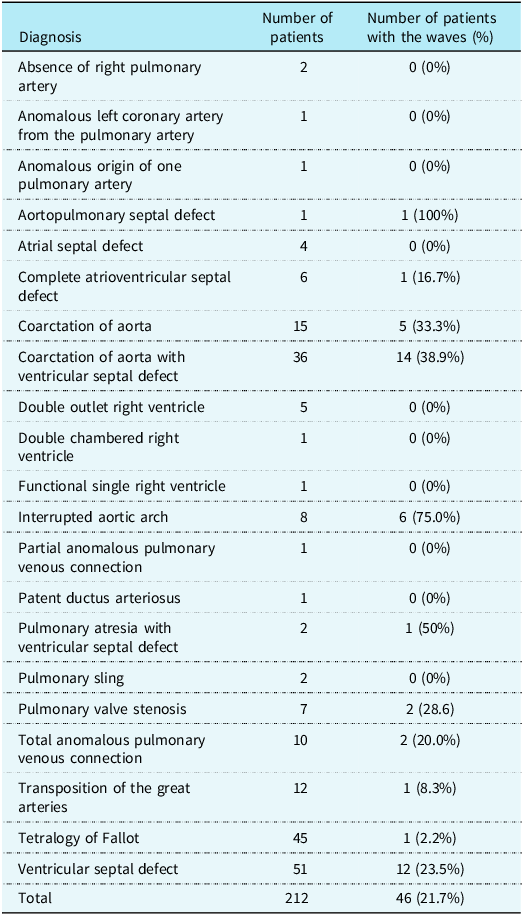
Table 1. The incidence of the arterial pressure waves in 212 patients with different types of CHD undergoing cardiac surgery
Operative procedures
Standard surgery procedures were performed. Reference Bercovitz, Shewmake and Newman9 Deep hypothermic circulatory arrest was used in patients with coarctation of aorta with ventricular septal defect or with interrupted aortic arch.
Postoperative management
Standard postoperative management was used. The management varied among clinicians as described elsewhere. Reference Li, Lou and Cui10
Methods of measurements
Systemic haemodynamics
A MostCare device (Vytech, Padova, Italy) was used to monitor systemic haemodynamics during operation and the first 48 h after cardiac intensive care unit (CICU) admission. Reference Romagnoli, Bevilacqua and Lazzeri6,Reference Romano11 MostCare was connected to the arterial line in the right arm of patients with aortic abnormalities and randomly in the right or left arm of patients with other CHDs. The raw data of systolic, diastolic, and mean arterial pressures, heart rate, the maximal slope of systolic upstroke (dP/dTmax), cardiac cycle efficiency were generated every 6 s to be simultaneous with near-infrared spectroscopy. Cardiac cycle efficiency is a unique variable derived by pressure recording analytical method according to the ratio of systolic energetic expenditure to the total energetic expenditure of the heartbeat, evaluating the compensating interplay of different cardiovascular system compartments, i.e., left and right ventricular contractility, pre- and after-load the ventricular-arterial coupling. Cardiac index was not obtained from the raw data because its accuracy requires artificial confirmation. Note that all patients received postoperative monitoring, while 108 (49.3%) received both perioperative and postoperative monitoring because the former was extended later after our initial findings concerning intraoperative events. Reference Li, Lou and Cui10 Obvious data artefacts were manually deleted.
ScO2 and SrO2
ScO2 of the left and right cerebral hemispheres and SrO2 of the renal region were simultaneously monitored with systemic haemodynamics by INVOS-5100C (Medtronic, Minneapolis, MN, USA). Obvious data artefacts were manually deleted.
Electroencephalogram
Continuous video-electroencephalogram recordings were obtained according to the international 10-20 system (Nicolet Co., WI, USA), Reference Shellhaas, Chang and Tsuchida12 together with systemic haemodynamics and regional oxygenation. The abnormal discharges included sharp waves defined as high amplitude (≥2.5 times of the background voltage) and short duration (<200 ms) and seizures (>10s). Reference Tsuchida, Wusthoff and Shellhaas13 The number of sharp waves was summarised every one hour. Background abnormalities were classified as normal, mild, moderate, and severe following previous methods. Reference Li, Lou and Cui10 All electroencephalograms were analysed by the qualified technicians (R Lin and S Ning) independently.
Cerebral blood flow velocity
The mean blood flow velocity (Vm) of the middle cerebral artery of both left and right hemispheres was measured at the 24th postoperative hours by a Delica EMS-9WA transcranial Doppler monitor (Delica, SZ, China). The recording duration was at least 15 s under a haemodynamically stable status.
Intensive care and general clinical data
Serum lactate was measured 3-hourly. Demographics, operative data, and clinical outcomes were recorded (Table 2). For patients with coarctation of aorta, echocardiography data of pressure gradient across the coarctation area were obtained. For patients with ventricular septal defect, its size and the degree of preoperative pulmonary arterial hypertension were recorded and graded as normal, mild, moderate, and severe. Reference Skinner15
Table 2. Comparison of demographic and clinical data between patients with and those without the waves in Aorta Group and Ventricular Septal Defect Group, respectively
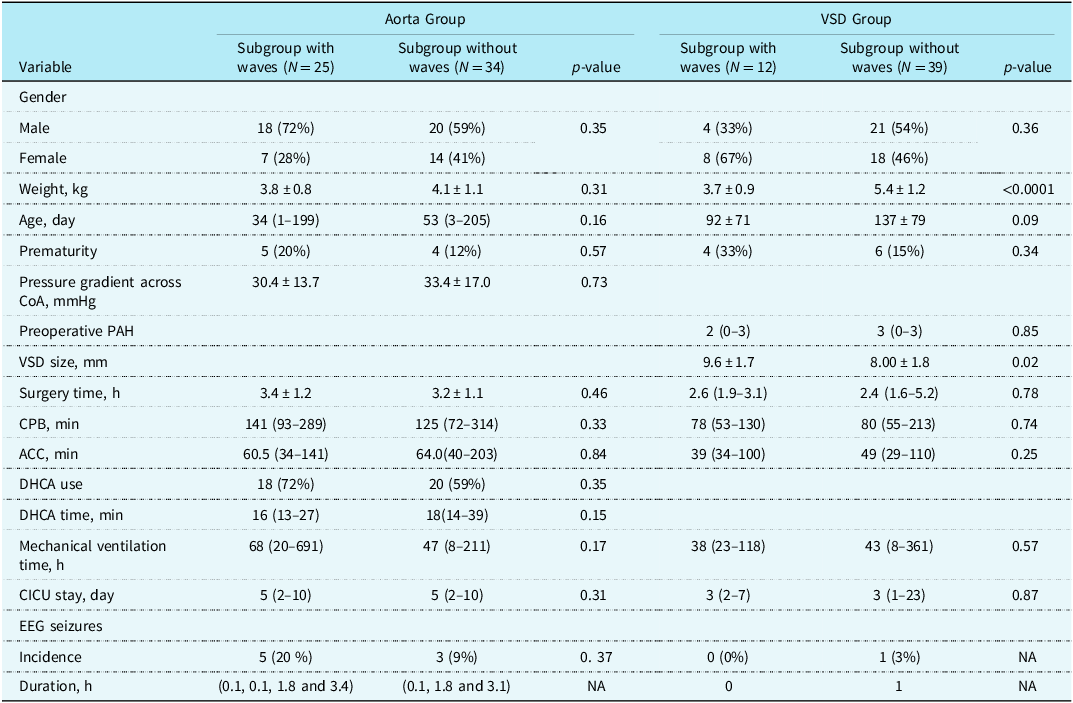
ACC = aortic cross-clamping; CoA = coarctation of aorta; CPB = cardiopulmonary bypass; DHCA = deep hypothermic cardiac arrest; NA=not applicable; PAH = pulmonary arterial hypertension; VSD = ventricular septal defect.
Identification of the arterial pressure waves with ScO2 and SrO2 fluctuations
The successive raw data from MostCare and near-infrared spectroscopy were recorded simultaneously with a 6-second interval and transferred to one computer. We graphed the raw arterial blood pressure data with ScO2 and SrO2 in each patient during the operation and the first 48 postoperative hours and manually identified the arterial pressure waves and their frequencies and the simultaneous ScO2 and SrO2 fluctuations.
Statistical analysis
Data were described as mean ±SD, median (range), or frequency (%) when appropriate. The independent sample t-test, Mann–Whitney U test, and Chi-square test were used to analyse the group difference (patients with slow arterial pressure waves vs. patients without) of continuous and categorical variables when appropriate. Mixed linear regression for repeated measures was used to analyse the temporal trends of the variables and the associations of the wave presence with other variables. The parameter estimates indicated the degree or slope and direction of the correlations. Statistical significance was determined at a probability value of <0.05. The PROC HPMIXED Procedure was used to fit the large-scale data (SAS 9.4, Cary, NC, the USA).
Results
Out of 21 types of CHD in 212 patients, 46 patients (21.7%) in 11 types of CHD showed the arterial pressure waves following repair (Table 1). Among the 46 patients, 25 (42.3%) had aortic arch abnormalities (Aorta Group, 6 with interrupted aortic arch, 14 with coarctation of aorta and ventricular septal defect, and 5 with coarctation of aorta) and 12 (23.5%) had ventricular septal defect (Ventricular Septal Defect Group). In the remaining 102 patients, 9 (8.8%) showed the waves in 7 other types of CHD. Given the significantly large patient base and high incidence in Aorta and Ventricular Septal Defect Groups, we focused on analysing the characteristics and clinical implications of the waves in the two groups. Of 15 patients with coarctation of aorta, 5 underwent cardiopulmonary bypass in whom 1 (20.0%) showed the waves and 10 did not undergo cardiopulmonary bypass in whom 4 (40.0%) had the waves after repair.
Characteristics of the waves in Aorta and Ventricular Septal Defect Groups
The incidence of the waves was significantly higher in Aorta Group compared to Ventricular Septal Defect Group (P < 0.05). The onset time and duration of the waves were not significant between Groups (Ps ≥ 0.68). In 13 patients who received both intra-and postoperative monitoring, the waves onset immediately after weaning from repair in 2 patients and at 32 h after CICU admission in 1 patient. In 24 patients who received postoperative monitoring only, the wave onset ranged 0 to 29 h (median 0) after CICU admission. In all 37 patients, the frequency of the waves was consistent at ∼ 90 s (∼0.01 Hz), with an intra-individual variation from 72 to 96 s (Supplemental Table 1). The morphology of the waves showed that the blood pressure increased sharply but decreased in a slower and more intermittent way. The waves were accompanied with fluctuations of ScO2 in 29 out of 37 patients (78.4%) including 19 out of 25 (76.0%) in Aorta Group and 10 out of 12 (83.3%) in Ventricular Septal Defect Group, and fluctuations of SrO2 in 25 out of 37 patients (67.6%) including 18 out of 25 (72.0%) in Aorta Group and 7 out of 12 (58.3%) in Ventricular Septal Defect Group) (Figure 1A, B).

Figure 1. A 30-minute segment of the arterial pressure waves accompanied with cerebral and renal oxygen saturation fluctuations during early postoperative period in one patient with coarctation of aorta and ventricular septal defect ( a ) and one patient with ventricular septal defect ( b ). MBP = mean blood pressure, ScO 2 = cerebral oxygen saturation, SrO 2 = renal oxygen saturation.
The waves in relation to clinical, haemodynamic, and cerebral measures in Aorta Group
In Aorta Group (Table 2), there was no significant difference in demographic and perioperative clinical data, the incidence of electroencephalogram seizures or the pressure gradient in the coarctation area between subgroup of patients with the waves and that without. The occurrence of the waves was negatively associated with time (parameter estimate = −0.01, P < 0.0001), and the temporal trends of other monitored variables were similar to our previous reports (Supplemental Table 2). Reference Li, Lou and Cui10 After adjusting for time, the subgroup with the waves, compared to that without, was significantly, or trended to be, associated with lower cardiac cycle efficiency, left and right Vm and worse electroencephalogram background abnormalities and higher number of sharp waves and serum lactate (Ps = 0.01–0.07) compared to that without. It was not significantly associated with the rest variables (Ps ≥ 0.18).
Within the subgroup with the waves and after adjusting for time, the presence of the waves was associated with lower systolic, diastolic and mean arterial blood pressure (SBP, DBP and MBP), dP/dTmax, ScO2 and SrO2, worse electroencephalogram background abnormalities, and higher number of electroencephalogram sharp waves (Ps < 0.0001) (Table 3).
Table 3. Statistical results of the associations between the arterial pressure waves and haemodynamic and cerebral variables in patients with aortic arch abnormalities
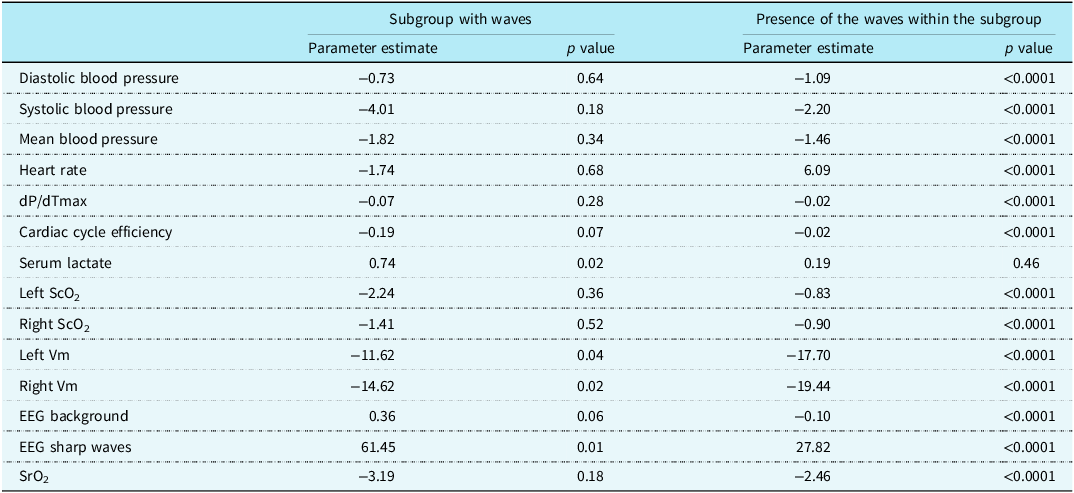
ScO2 = cerebral oxygen saturation; SrO2 = renal oxygen saturation; Vm = mean cerebral blood flow velocity.
The waves in relation to clinical, haemodynamic, and cerebral measures in Ventricular Septal Defect Group
In Ventricular Septal Defect Group (Table 2), the subgroup with the waves had, or trended to have, a significantly lower weight (P < 0.0001), younger age (P = 0.09), and larger ventricular septal defect size (P = 0.02). The degree of preoperative pulmonary arterial hypertension did not differ between two subgroups (P = 0.85).
The presence of the waves was negatively associated with time (parameter estimate = -0.01, P < 0.0001), and the temporal trends of other monitored variables were similar to our previous reports. Reference Li, Lou and Cui10 After adjusting for time, the subgroup with the waves was significantly, or trended to be, associated with lower DBP and mean blood pressure (P = 0.03 and 0.09, respectively), but not with the rest variables (Ps ≥ 0.16).
Within the subgroup with the waves and after adjusting for time, the wave presence was significantly associated with lower DBP and mean blood pressure, dP/dTmax, cardiac cycle efficiency, ScO2, and SrO2 (Ps < 0.0001) and higher number of electroencephalogram sharp waves (Ps < 0.0001) (Table 4)
Table 4. Statistical results of the associations between the slowest arterial pressure waves and haemodynamic and cerebral variables among patients with ventricular septal defect

ScO2 = cerebral oxygen saturation; SrO2 = renal oxygen saturation; Vm = mean cerebral blood flow velocity.
Aorta Group had significantly worse electroencephalogram background abnormality and higher number of electroencephalogram sharp wave than Ventricular Septal Defect Group (parameter estimate = 0.36 and 72.7 respectively, Ps < 0.0001).
Discussion
By continuously monitoring systemic haemodynamics of children during cardiopulmonary bypass and the subsequent 48 postoperative hours, we found the novel and consistent arterial pressure waves with a period of ∼ 90 s (∼0.01 Hz) that occurred most frequently in patients with aortic arch abnormalities (42%), secondarily in those with ventricular septal defect (24%) and rarely in other CHD types. In both Aorta and Ventricular Septal Defect Groups, the waves were mostly found immediately after surgical repair with or without the use of cardiopulmonary bypass and lasted 3 to 48 h after CICU admission.
To our knowledge, such waves have not been reported in children with CHD following cardiac surgery. The arterial pressure waves have drawn much attention in the past century. Reference Guyton and Statterfield1–Reference Carroll4 They could be categorised into four types with distinctive frequencies. Reference Carroll4 The first type, with a period of ∼ 1 s, is largely caused by heartbeats; the second (∼5 s, i.e., Traube-Hering waves,) is largely affected by respiration; and the third (∼10 s in humans, i.e., Mayer waves) may occur in healthy humans Reference Taylor, Williams, Seals and Davy16 as well as in various pathological states including cerebral ischaemia Reference Guyton and Statterfield1 and sudden circulatory changes. Reference Guyton and Harris2 Of interest, the frequency of Mayer waves is consistent within species (e.g., 0.3 Hz in rabbits, 0.4 Hz in rats). Reference Julien5 The fourth (∼60 s) has been found in animals like cats, dogs, and rabbits, not yet in humans. Reference Barcroft and Nisimaru17,Reference Roy18 It was named the “spleen wave” because it was caused by the rhythmic spleen volume change. Reference Barcroft and Nisimaru3 Therefore, the waves identified in our patients with a period of ∼ 90 s are the slowest and have not been reported in humans or animals. Besides the period, the wave morphology was also distinctive: the blood pressure increased sharply but decreased in a slower and more intermittent way in the waves we identified (Figure 1), while it fluctuated smoothly in the previous ones. Reference Guyton and Harris2,Reference Barcroft and Nisimaru17,Reference Barcroft, Nisimaru and Steggerda19
Importantly, such arterial pressure waves had clear clinical implications. Integrating two patient groups’ results, we found that the occurrence of the waves, when compared between the subgroups with or without the waves and particularly within the subgroup with the waves, was significantly associated with poorer systemic haemodynamics (lower blood pressures), myocardial mechanics and efficiency (lower dP/dTmax and cardiac cycle efficiency), worse cerebral oxygenation (lower Vm and ScO2), and brain injury (worse electroencephalogram background abnormalities and higher number of electroencephalogram sharp waves) as well as renal oxygenation (lower SrO2).
Both Aorta and Ventricular Septal Defect Groups are characterised by a volume increase in systemic circulation after repair, and specifically in the lower body in the case of aortic arch abnormalities, particularly relative to the smaller systemic arterial vascular bed before repair. Previous studies have identified the “spleen wave” early in 1882, Reference Roy18 that is, a sudden rise in blood pressure or recovery of spleen circulation after a temporary stoppage could elicit rhythmic spleen volume changes in cats, dogs, and rabbits, all with a period of ∼ 60 s, as a potential adaptative mechanism, Reference Barcroft and Nisimaru17 and this volume change could further induce synchronous arterial pressure waves. Reference Barcroft and Nisimaru3 Later experiments showed that similar volume changes in intestine Reference Barcroft, Nisimaru and Steggerda19 and kidney Reference Roy18 could also induce similar arterial pressure waves. This hypothesis may be supported by the relatively higher incidence of wave presence in the left to right shunt CHD types (Table 1) in contrast to the low incidence in tetralogy of Fallot. Of note, synchronised fluctuations in SrO2 were also found in about 70% of patients with the waves.
Other mechanisms, related to the anatomical and haemodynamic features of aortic arch abnormalities, may uniquely contribute to the higher incidence of the waves in Aorta Group. Before surgery, Aorta Group had adapted to a high upper-body blood pressure and perfusion status. The abrupt decrease in upper-body blood pressure and perfusion after repair may have triggered the brainstem ischaemic response. Central nervous system ischaemia could stimulate the respiratory and cardiac control nuclei in the brain-stem to increase blood pressure as compensative mechanisms to improve brain perfusion and relieve the ischaemic stimulation, and such ischaemia has been used to induce Mayer waves in dogs. Reference Guyton and Statterfield1
Another potential mechanism for the waves in Aorta Group may lie in the bluntness of the pressoreceptor-autonomic system, which regulates blood pressure via a negative reflex mechanism, and the system delay would result in arterial pressure waves. Reference Guyton and Harris2 This bluntness has contributed to the genesis of Mayer waves. Reference Julien5 Patients with aortic arch abnormalities have been found to have blunted baroreceptor sensitivity due to vascular abnormalities like an increase in collagen and a decrease in smooth muscle content in the pre-coarctation vascular beds, which diminish vascular elasticity even before operation Reference Polson, McCallion and Waki21–Reference Sehested, Baandrup and Mikkelsen23 and are not completely reversible after repair. Reference Celermajer and Greaves24 Besides, the elevated renin and angiotensin II after repair Reference Streeten and Blackman25 may further contribute to this bluntness via acting upon areas of postrema and nucleus tractus solitarii. Reference Polson, McCallion and Waki21 This lack of cerebral vascular elasticity may make the brain more difficult to adapt to the haemodynamics stress caused by the waves, as indicated by the substantially higher electroencephalogram sharp wave number and worse background abnormalities in Aorta Group. Reference Vrselja, Brkic, Mrdenovic, Radic and Curic26,Reference O’Rourke and Safar27 Attention has been increasingly paid to cerebral vascular changes, like intracranial aneurysm, Reference Curtis, Bradley and Wilde28 and brain injuries, like stroke, Reference Trenk, Lammers and Radke29 from the early perioperative period into adulthood in patients with aortic arch abnormalities. Reference Trenk, Lammers and Radke29,Reference Ryan and Richard30
When the arterial pressure waves occurred, synchronised fluctuations in ScO2 were also observed in most of patients, reflecting a loss of cerebral autoregulation. Reference Steiner, Pfister, Strebel, Radolovich, Smielewski and Czosnyka7 The loss of cerebral autoregulation has been well documented in children undergoing cardiopulmonary bypass Reference Brady, Mytar and Lee8,Reference Votava-Smith, Statile and Taylor31,Reference Bassan, Gauvreau and Newburger32 and other critically ill patients like sepsis. Reference Crippa, Subirà and Vincent33 It usually applies to what occurs under hypotension (e.g., MBP < 40 mmHg during cardiopulmonary bypass). Reference Brady, Mytar and Lee8,Reference Crippa, Subirà and Vincent33 However, this is not the case in our present study. The synchronised ScO2 fluctuations did not specifically occur under hypotension, rather they have a clear time window, i.e., the early postoperative period. Such loss of cerebral autoregulation may be more similar to that observed in severe head injury patients with Mayer waves. Reference Lemaire, Khalil and Cervenansky34 However, the waves identified in our study are unique and have the slowest frequency compared to other waves ever reported. The loss of cerebral autoregulation, in either way, would render the brain vulnerable to injuries. For example, an abrupt increase in blood pressure would be particularly dangerous for causing haemorrhagic complications. Reference Neil, Volpe, Volpe, Inder, Darras, de Vries, du Plessis, Neil and Perlman35 This might also contribute to the worse brain injury in our patients with the waves, particularly in Aorta Group.
Some studies have reported the positive implications of the arterial pressure waves. Reference Julien5,Reference Aalkjær, Boedtkjer and Matchkov36 For example, Mayer waves could trigger the liberation of endothelium-derived nitric oxide and benefit the end-organ function. Reference Julien5 Likewise, rhythmic vasomotion, leading to a blood flow motion, could improve tissue oxygen delivery and metabolism. Reference Aalkjær, Boedtkjer and Matchkov36 Thus, although these waves were associated with poorer haemodynamics and compromised brain perfusion and function, they might not contribute to them. Rather they might serve as an adaptive mechanism responding to them, like pacemaker for example. Reference Julien5 Clearly, these above-discussed mechanisms are purely speculative, based on previous studies on other types of arterial pressure waves. Note that 46 patients with different CHD types and different age and gender had the same unique wave frequency (∼0.01 Hz), so there may be other mechanisms underlying the wave genesis in children with CHD following surgical repair that need explorations and expectedly complex. Mayer waves found more than 70 years ago remain an enigma. Reference Julien5
Limitations
This study had several limitations. First, the patient number was still small and our monitoring time was still limited. Further studies are warranted in larger patient populations and longer monitoring time in varied CHD types to better depict the characteristics and clinical implications of the waves. Second, no significant difference was found in the incidence of electroencephalogram seizures between subgroups, due to the small number of patients. The abnormal discharges were mainly manifested as sharp waves which have been paid little attention in children with CHD. Neonates with higher incidence of sharp waves and other electroencephalogram transients had worse neurological outcomes at 12 months of age. Reference Biagioni, Boldrini, Bottone, Pieri and Cioni37 Third, We did not evaluate neurodevelopmental outcomes of these patients, which are being studied. Third, we did not investigate the potential mechanisms contributing to the waves, such as the level of circulating renin and angiotensin II that may provoke arterial blood pressure variations and relate to Mayer waves. Reference Polson, McCallion and Waki21,Reference Lemaire, Khalil and Cervenansky34
Conclusions
The novel arterial pressure waves with a frequency of ∼ 90 s in children with CHD following surgical repair are the slowest ever reported in humans and animals. They are prevalent in patients with aortic arch abnormalities or Ventricular Septal Defect. While the occurrence of the waves was associated with statistically worse and fluctuated ScO2 and SrO2, worse systemic haemodynamics, and electroencephalogram abnormalities, at present these waves have no known clinical relevance.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951124026039.
Availability of data and materials
The data supporting the analyses and generated during the study are presented and available in the Open Science Framework at https://osf.io/t7wru/.
Acknowledgements
The authors acknowledge all the clinicians and nurses at the Heart Center of Guangzhou Women and Children’s Hospital for their support of our study.
Authors’ contributions
Li Ma and Linyang Yu have contributed to the conducting and reporting of the work described in the article. Yingying Liu, Rouyi Lin, Jinqing Feng, Yanqin Cui, Jianbin Li, Lijuan Li, Shuyao Ning, Minghui Zou, Guodong Huang, Huanzhen Wang, and Xinxin Chen have contributed to the conducting of the work. Jia Li has contributed to the planning, conducting, and reporting of the research.
Financial support
The Key-Area Research and Development Program of Guangdong Province (No. 2019B020227001); Jia Li’s start-up fund provided by Guangzhou Women and Children’s Medical Center.
The study was reviewed and approved by Guangzhou Women and Children’s Medical Center institutional Research Ethics Boards. (No. 46201; 2019-12-13).
Competing interests
None.
Ethical standard
Ethics approval and consent to participate: This study was approved by the institutional ethics board at the Guangzhou Women and Children’s Medical Center No.46201) and informed consent obtained from the participants and their parents/legal guardians.







