



Transcatheter closure of the patent ductus arteriosus has become the leading approach due to development of the devices. Reference Agrawal, Waller, Surendan and Sathanandam1–Reference Backes, Rivera and Bridge4 It is no exaggeration to say that the success of this procedure depends on the correct choice of the device. It is therefore extremely important to understand the morphology of the patent ductus arteriosus and to measure its size accurately. The diameter and length of the patent ductus arteriosus are usually measured using lateral angiographic images. Occasionally, the devices come out of the patent ductus arteriosus easily and appear inappropriate, even if the device size is considered optimal based on the lateral angiographic images. The extensibility of the patent ductus arteriosus may also have an effect, but it is common for there to be a difference in the minimum patent ductus arteriosus diameter between the horizontal echocardiographic view and the long axis view. It remains controversial whether lateral angiographic images can accurately measure the minimum patent ductus arteriosus diameter. Reference Anilkumar3 In our institution, a contrast-enhanced CT is performed for a relatively large patent ductus arteriosus in early infants. In this study, we examined the diameter of cross section of the patent ductus arteriosus minimum portion using contrast-enhanced CT imaging and investigated the accurate cross-sectional morphology and size of them.
Materials and methods
We conducted a retrospective study of 29 patients who underwent contrast-enhanced CT imaging before transcatheter closure of the patent ductus arteriosus between January 2016 and December 2022. Contrast CT imaging was performed using the Aquilion ONE PRISM Edition (Canon Medical Systems Corporation, Otawara, Japan) with the following settings: tube voltage, 80–100 kV; tube current, 90–462 mA. Imaging was performed under sedation using virtual electrocardiographic synchronisation conditions at a heart rate of 150 beats/min. The contrast agent was 300 mg/mL iopamidol, diluted 1.5–2.0 with normal saline and injected at a dose of 2 mL/kg and a rate of 1.0–1.5 mL/s; imaging was performed 0–3 s after injection. An Aquarius NET (TeraRecon, Inc., Foster City, CA) was then used to extract the long sagittal and horizontal axes of the patent ductus arteriosus, from which a section perpendicular to these axes was extracted. The morphology of the narrowest part was visualised and measured (Fig. 1). Angiographic measurements were performed on lateral images acquired with the Allura Xper FD20/20 (biplane system, Philips Healthcare, Best, The Netherlands).

Figure 1. Narrowest part of the PDA visualised by contrast-enhanced CT. a : Narrowest part of long axis of horizontal cross section. b : Narrowest part of sagittal long axis. c : Narrowest part of the coronal section after adjusting by A and B. d : 3D image of the narrowest part after adjusting by a and B.
For the angiography, a 4-Fr pigtail catheter was placed in the thoracic aorta with the upper end at the lower end of the patent ductus arteriosus. The contrast agent was iopamidol 370 mg/mL. Infants weighing 3 kg or less received 2.0 mL/kg, those weighing 3–6 kg received 1.5 mL/kg, and those weighing 6 kg or more received 1 mL/kg. The diameter of the narrowest point of the patent ductus arteriosus was measured in the lateral view during ventricular systole, when the patent ductus arteriosus diameter was at its maximum.
The diameter appears different on CT depending on how the image contrast was applied; therefore, the measured minimum patent ductus arteriosus diameter on angiography was compared with the measured minimum vertical patent ductus arteriosus diameter on the CT images, adjusting the contrast value for the measurements. We then measured the vertical and horizontal diameters of the patent ductus arteriosus at its narrowest point using CT imaging. We also investigated differences in the morphology of the narrowest part of the patent ductus arteriosus and whether the age in months was associated with the morphology or diameter of this part of the PDA.
Basically, the morphological classification of the patent ductus arteriosus was based on the Krichenko classification. Reference Krichenko, Benson and Burrows5 To further clarify this classification, we defined types A, C, and E based on the relationships between the length, minimum diameter, and ampulla length of the patent ductus arteriosus: type A, the ampulla length was larger than the length; type C, the length was larger than the ampulla length, and the minimum diameter was greater than or equal to half the ampulla length; type E, the length was larger than the ampulla length, and the minimum diameter was smaller than half the ampulla length (Fig. 2).
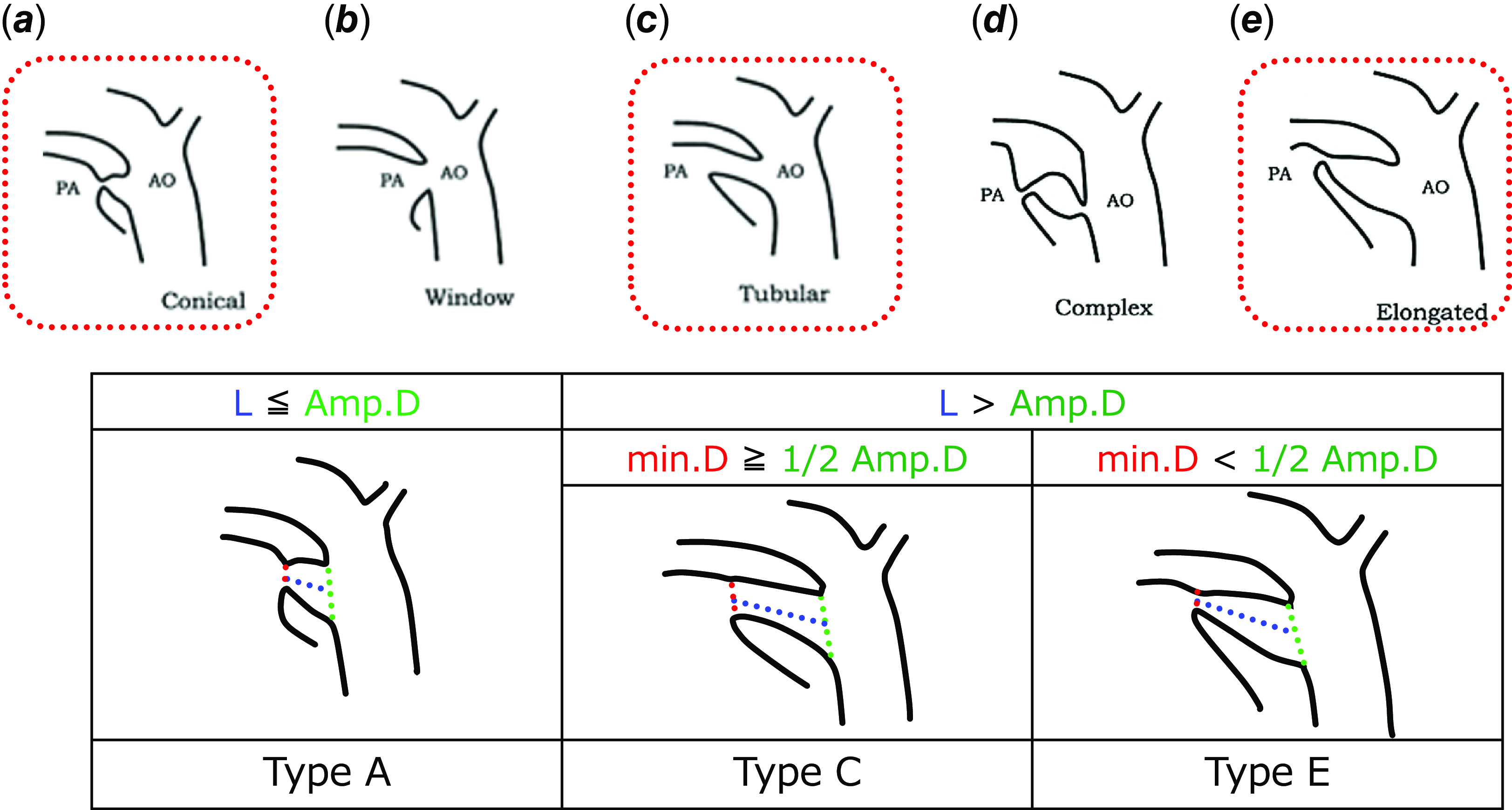
Figure 2. Patent ductus arteriosus classification. Upper row: Krichenko classification. Lower row: definition of type A, type C, and type E in this article. PA = pulmonary artery, AO = aorta, L = length, amp. D = ampulla diameter, min.D = minimum diameter.
Statistical analysis
The relationship between the morphology of the patent ductus arteriosus on the CT image and on the angiography was analysed using linear regression. Comparisons between groups were made using the Mann–Whitney U and chi-squared tests. Statistical significance was set at p < 0.05. Intraclass correlation coefficients were obtained to evaluate the consistency between CT examination measurements and angiographic measurements. The vertical diameter measured from CT and angiography was measured by two observers, one of whom measured it again two weeks later. The Bland–Altman analysis used these measurements to calculate the inter- and intra-observer reliability. The Bland–Altman analysis involved investigating the presence of addition and proportional errors—both systematic error types. Addition error involved calculating the 95% confidence interval for the average differences between the measured values. It was judged that a positive or negative fixed error was present when this interval did not include 0. The proportional error involved calculating the Pearson product–moment correlation coefficient in the Bland–Altman plot. A proportional error existed when a strong correlation was present at a significance level of 5%.
All statistical analyses were performed using GraphPad PRISM, Version 9 (GraphPad Software, San Diego, CA, USA).
Ethical considerations
This study was conducted with the approval of the Hiroshima City Hospital Institutional Review Board and the consent of the patients’ families.
Results
Cases
We performed CT imaging and catheter treatment in all 29 infants. At the time of treatment, the median age was 4.8 (range, 1–52) months, the median weight was 5.0 (range, 2.5–12.7) kg, and the male–female ratio was 20:9. The median minimum patent ductus arteriosus vertical diameter was 2.9 (range, 1.6–6.6) mm. Of the patients in this study, 27 were treated with catheterisation and 2 were treated with surgery (Table 1).
Table 1. Horizontal length and vertical length were measured from CT

ADO = Amplatzer™ Duct Occluder (Abott, Pylmouth, MN, USA); AVP = Amplatzer™ Vascular Plug.
Case 9: Catheterisation was abandoned as AVPII6 mm was undersized, and AVPII8 was complicated by an occluded LPA.
Case15: Initially, AVPII 6 mm was placed. However, due to undersize, the size was increased to AVPII 8 mm.
Case 25: AVPII12 mm was too small and AVPII14 mm had a high probability of LPA occlusion, so we decided against catheter treatment.
Investigation of CT and angiographic measurements of the narrowest patent ductus arteriosus part
The vertical diameter of the patent ductus arteriosus at the narrowest point on the CT images and the vertical systolic diameter on angiography showed a significant correlation (R2 = 0.90, p < 0.001; Fig. 3), demonstrating that the CT contrast setting (CT value) was appropriate.

Figure 3. Correlation diagram of vertical diameter of narrowest part of the PDA measured by 3DCT ( a ) and angiography ( b ). Red dotted line: measurement of narrowest part of the PDA.
The narrowest part of the patent ductus arteriosus in the CT image had a horizontal-to-vertical diameter ratio in the range of 1.0–1.7, with no cases where the vertical diameter was greater than the horizontal diameter. One patient had identical vertical and horizontal diameters, and the remaining 28 had a horizontal diameter greater than the vertical, resulting in a horizontally oriented elliptical shape (Fig. 4).

Figure 4. Comparison of horizontal and vertical diameters of narrowest part of the PDA measured by 3DCT. Red dotted line: vertical diameters of narrowest part of the PDA. Blue dotted line: horizontal diameters of narrowest part of the PDA.
We examined differences in the morphology of the narrowest part according to the Krichenko classification, which resulted in 13 patients with type A, 14 with type C and two with type E. The median horizontal-to-vertical diameter ratio by type was: type A, 1.22; type C, 1.29; type E, 1.62. The ratios in the three groups differed significantly (p = 0.017) (Fig. 5). However, type E has a small number of cases. Caution should be exercised in interpreting the results.
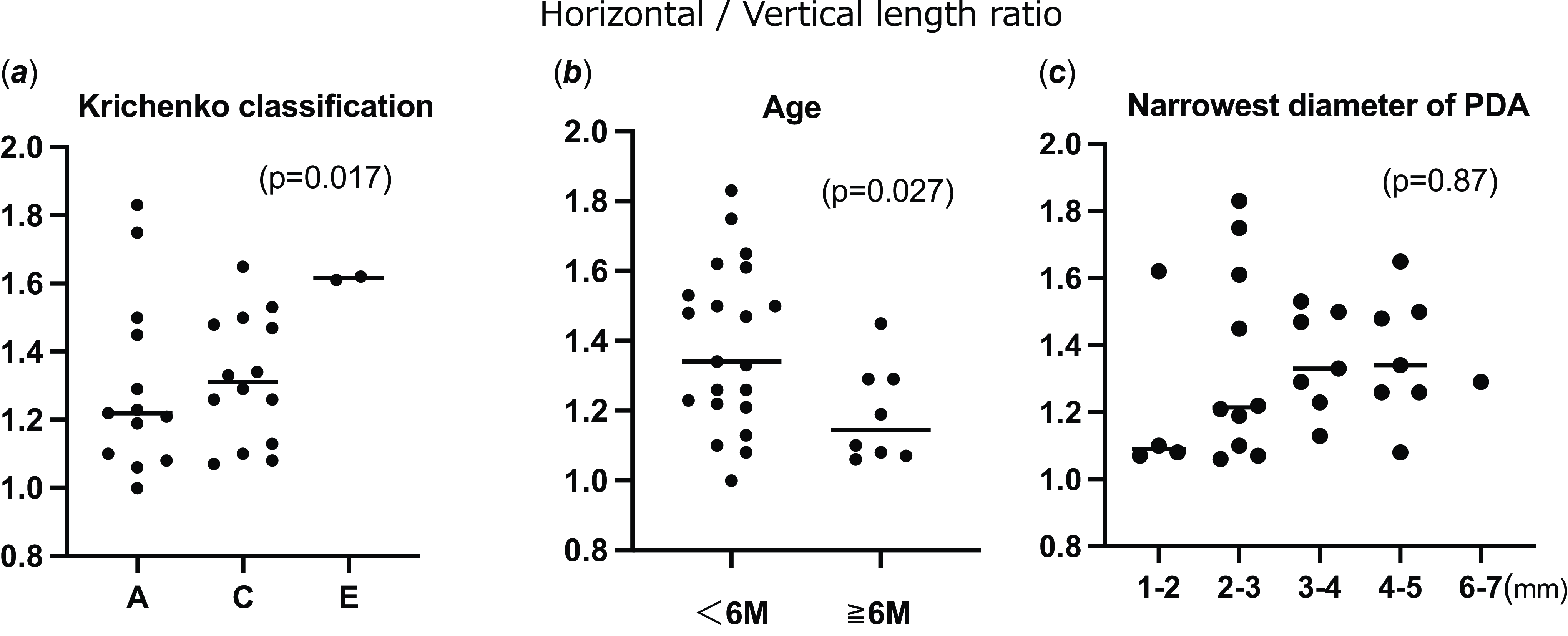
Figure 5. ( a ) A = Krichenko type A, C = Krichenko type C, E = Krichenko type E. ( b )<6M=less than six months older, ≧ 6M= six months or older.
We then investigated whether the shape of the cross section at the narrowest point of the patent ductus arteriosus was associated with the patients’ age in months. When the patients were divided into a group aged less than six months (n = 21) and a group aged six months or older (n = 8), the respective median horizontal to vertical diameter ratios were 1.34 and 1.15, with a significant difference between them (p = 0.027). The patent ductus arteriosus tended to be more elliptical at younger ages (Fig. 5).
We also investigated the shape of the narrowest part of the patent ductus arteriosus on the basis of the vertical diameter of the patent ductus arteriosus. When comparing groups with a minimum PDA diameter of 1–2 mm (n = 4), 2–3 mm (n = 10), 3–4 mm (n = 7), 4–5 mm (n = 7), and 6–7 mm (n = 1), they were statistically similar (p = 0.87). There was no correlation between the vertical diameter of the patent ductus arteriosus and the elliptical shape (Fig. 5).
Reliability of the patent ductus arteriosus measurements
When comparing morphology according to the patent ductus arteriosus vertical diameter, the inter-observer intraclass correlation coefficients values for the vertical and horizontal diameters measured on the contrast CT images were 0.98 and 0.97, respectively, showing strong correlations (Fig. 6). The intra- and inter-observer reproducibility in the patent ductus arteriosus analysis was confirmed using Bland–Altman analysis with ten randomly selected patients. Small biases were observed for intra-observer patent ductus arteriosus measurements (vertical diameter, 0.02; horizontal diameter, 0.12) and inter-observer patent ductus arteriosus measurements (vertical diameter, 0.38; horizontal diameter, 0.30); however, the 95% confidence intervals included 0, indicating that the patent ductus arteriosus measurements had high reproducibility (Fig. 7).
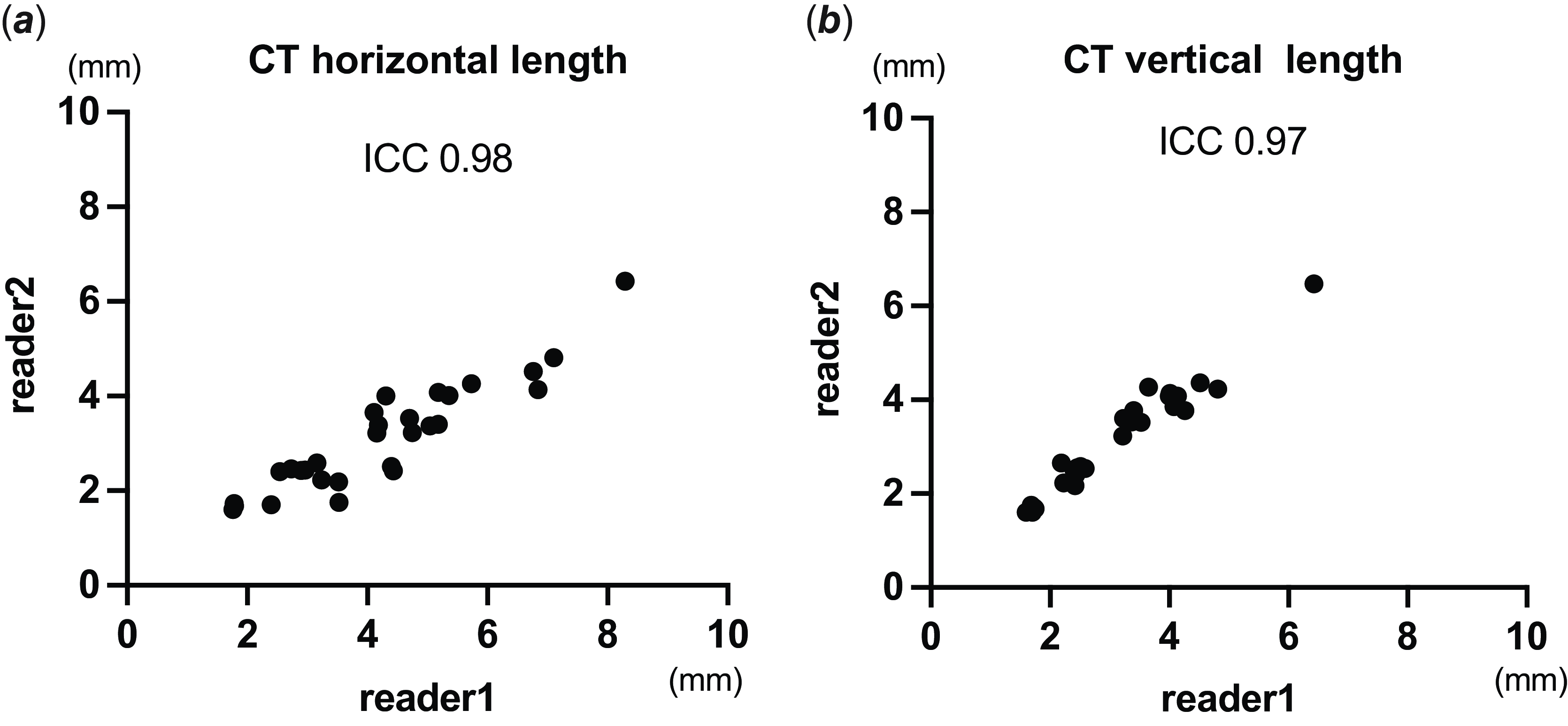
Figure 6. Regression plot between reader 1 and reader 2. ( a ) narrowest horizontal diameter from CT. ( b ) narrowest vertical diameter from CT.
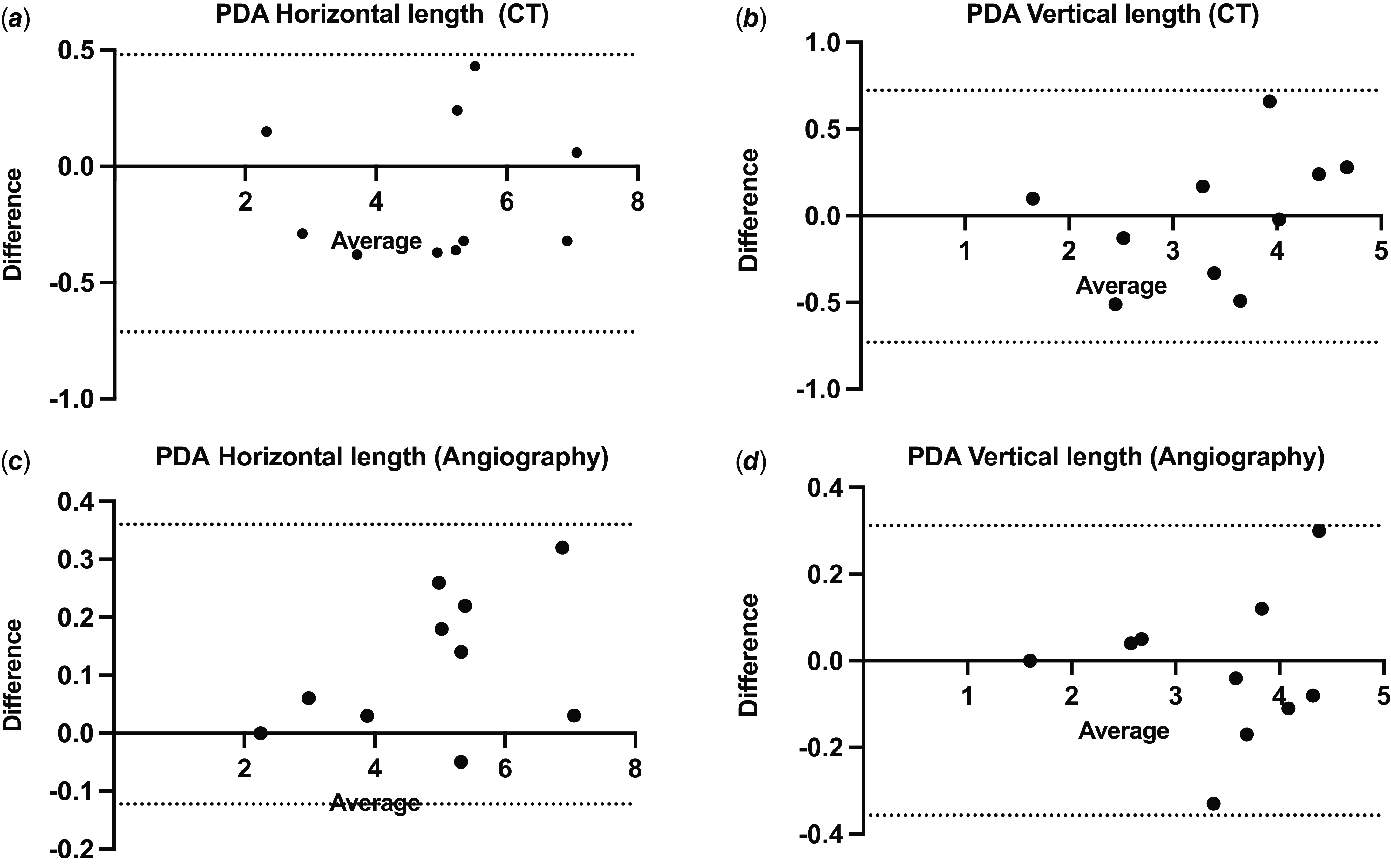
Figure 7. Bland–Altman plots of inter-observer ( a , b ) and intra-observer ( c , d ) variability showing differences in the values of PDA horizontal length from CT and angiography, and vertical length from CT and angiography. X-axis: absolute average of two measurements for each index. Y-axis: difference between the two measurements for each index. The solid lines indicate the mean ± 1.96 SD.
Radiation exposure
The median tube current was 179 ± 92mA. A low radiation dose was achieved by the proposed protocol, as indicated by the average effective dose of 1.4 ± 0.86 mGy.
Discussion
Transcatheter closure is preferable to surgical ligation in most modern situations, and recommendations have recently been developed for the management and treatment of patent ductus arteriosus from preterm infants to adults. Reference Backes, Hill and Shelton6 In the catheter treatment of patent ductus arteriosus, it is common to measure the size of the patent ductus arteriosus on a lateral angiography image, and a device of an optimal size is selected; however, occasionally, the device size may prove to be too small when it falls off from patent ductus arteriosus easily. The diameter of the patent ductus arteriosus changes with the cardiac cycle, so undersizing may occur if it is not measured at its maximum phase. It is therefore important to make careful observations in each frame and to take measurements in the frame with the largest diameter during ventricular systole. Reference Krishna Kumar, Sievert, Qureshi, Wilson and Hijazi7 And the arterial duct is characterised by high elasticity, especially in infants, possibly due to undersizing. Furthermore, it is common for the minimum patent ductus arteriosus diameter in the horizontal view of the echocardiogram to differ from that in the long-axis view. We therefore questioned whether the lateral angiographic view could correctly show the diameter of the narrowest part of the patent ductus arteriosus . The vertical diameter of the patent ductus arteriosus can be measured on lateral angiography images. However, the horizontal diameter is difficult to measure on either frontal or lateral images and is therefore neglected. Even if we try to measure the horizontal diameter of the patent ductus arteriosus by rotating the RAO instead of the front view, we often have to rotate a lot to visualise it well, and we often cannot visualise the complete horizontal section. However, our CT data showed that the narrowest part of the patent ductus arteriosus often had a larger horizontal diameter than the vertical diameter, resulting in an elliptical shape. Therefore, the size of the patent ductus arteriosus may be underestimated by the information obtained from the angiographic lateral view. As the horizontal diameter is larger compared to the vertical diameter, this underestimation becomes more significant, and the selection of the device size could be wrong.
In this study, small patent ductus arteriosus, including silent patent ductus arteriosus, did not undergo contrast CT imaging before catheter intervention. Patients included in this study were those with relatively large patent ductus arteriosus. Therefore, these data suggest that most relatively large patent ductus arteriosus have a horizontally oriented elliptical shape. This is important information to avoid choosing too small devices to close large patent ductus arteriosus. The cases that require the placement of a large device in the early stages of infants are small build size and we believe that the CT imaging is useful for a more accurate assessment prior to placement.
In addition, our investigation showed that the horizontal diameter tended to be larger in patients younger than 6 months than in those older than 6 months. Patients who need closure of the patent ductus arteriosus younger than 6 months must be symptomatic because of significantly large patent ductus arteriosus, and they are considered high-risk cases that inevitably require a large device relative to the physique of the patient. The risk of left pulmonary artery stenosis and aortic stenosis due to device placement is obviously high in such cases, Reference El-Said, Bratincsak and Foerster8 so it is ideal to select a device as small as possible especially for this group of patients. On the other hand, the device must not slip off the patent ductus arteriosus but be enough stable, Reference Baruteau, Hascoët and Baruteau9,Reference Ewert10 so the selected device should be as small as possible and sufficiently large for the narrowest diameter. There have also been reports of effective closure using muscular ventricular septal defect devices as a treatment device for patent ductus arteriosus with heart failure in the early infant. Reference Salam, Bautista-Rodriguez and Karsenty11 Our result which shows a strong tendency for a larger horizontal than vertical diameter indicates that angiographic measurements may include the risk to underestimate the true diameter and the deployment of the device would end in failure. So, we suggest that the horizontal diameter must be taken into account when selecting the correct device size, especially in younger patients. And, we believe that for neonates and infants with a patent ductus arteriosus large enough to require device closure, there is a benefit to having a CT scan before treatment.
From the perspective of radiation exposure, in recent years, advances in technology have made it possible to construct clear images at low doses even in the paediatric heart field. Reference Shirota, Maeda and Namiki12,Reference Maeda, Shirota and Shibata13 Although it is an additional test to catheterisation imaging, we believe it is an acceptable and useful evaluation method because it sometimes provides more information than can be obtained by catheter angiography.
Ito et al. and Yokoyama reported that the patent ductus arteriosus closure mechanism involves the contraction of mature vascular smooth muscle and intima thickening by vascular separation modelling. Reference Ito, Yokoyama and Saito14,Reference Yokoyama15 However, studies on morphological changes from narrowing to the closure of the narrowest part of the arterial duct that retains patency even after birth are lacking. A more comprehensive study to understand the morphology of the patent ductus arteriosus narrowest part is necessary to do the safe and effective device closure of the patent ductus arteriosus.
Limitation
First, the number of people in the trial was small. In addition, the imaging conditions of contrast-enhanced CT do not allow precise adjustment of the systolic phase. Therefore, in this study, we confirmed that there is no difference in the size of the systolic lateral image from angiography and the lateral image from contrast-enhanced CT.
Conclusions
Most patent ductus arteriosus have a horizontally oriented elliptical shape in this study. This characteristic is important information that there is a possibility that angiography cannot evaluate the real size of the narrowest point of the patent ductus arteriosus. Furthermore, this tendency is especially strong in infants whose patent ductus arteriosus involve some difficulties in device closure. Understanding of the real morphology of the narrowest point of the patent ductus arteriosus is quite useful and necessary for selecting an appropriate device and preventing complications related to the catheter intervention.
Author contribution
YF conceived the study concept and design. NN, MK, KO, HU, and KK conducted follow-up of patients and performed computed tomography and catheter interventions. NN conducted review and editing. YF and NN collected the electronic data, conducted data interpretation, and statistical analyses. YF was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Availability of data and material
The data that support the findings of this study are available from the corresponding author, YF, upon reasonable request.
Financial support
None.
Competing interests
None.
Ethical standard
The Hiroshima City Hospital Institutional Review Board approved this study.
Patient consent statement
This study received the consent of the patients’ families.
Consent to participate
Consent to participate in the study was obtained from all authors.
Consent for publication
Consent for publication was obtained from all authors.









 Open access
Open access