


Autism spectrum disorder (ASD) associated with average range IQ (e.g. Asperger syndrome) or so-called high-functioning autism, has been shown to have a varied trajectory of functioning through the lifespan. Reference Cederlund, Hagberg, Billstedt, Gillberg and Gillberg1–Reference Howlin, Moss, Savage and Rutter4 Severity of ASD symptoms, intelligence, psychiatric comorbidity, degree of support, and age at diagnosis have all been hypothesised to affect long-term outcome but there is no clear-cut evidence of factors that affect ultimate outcome. Several of the earliest works within the field Reference Asperger5–Reference Wing and Gould7 suggested personality features as possible factors affecting functioning and outcome, but very little is published regarding the possible connection between personality and outcome in ASD. In a recent published thesis Reference Suh8 it was shown that children with a history of ASD and so-called ‘optimal outcome’ (i.e. no longer meets criteria of an ASD and has functioning in the normal range) differed significantly from a matched ASD group regarding a number of personality features, and were more similar to controls regarding personality, except regarding extroversion where the optimal outcome group had higher scores. This gives some support to the notion that personality may be related to different long-term outcomes in populations with ASD.
The psychobiological personality theories of Robert Cloninger Reference Cloninger, Svrakic and Przybeck9,Reference Cloninger10 comprise four temperament dimensions (highly hereditary traits relating to different emotional drives) and three character dimensions (less heritable traits that develop over age relating to style of mental self-governing). These seven dimensions have been associated with varying aspects of mental health. Reference Fassino, Amianto, Sobrero and Abbate Daga11–Reference Jylha, Ketokivi, Mantere, Melartin, Suominen and Vuorilehto13 The four temperament dimensions described in Cloninger's theory are novelty seeking, harm avoidance, reward dependence and persistence, and the three character dimensions are self-directedness, cooperativeness and self-transcendence (Table 1).
Table 1 Description of traits associated with high and low levels of specific temperament and character dimensions
| Descriptors | High score | Low score |
|---|---|---|
| Novelty seeking | Excitable | Stoic |
| Impulsive | Reflective | |
| Extravagant | Reserved | |
| Disorderly | Orderly | |
| Harm avoidance | Worried | Optimistic |
| Fearful | Calm | |
| Shy | Outgoing | |
| Fatigable | Vigorous | |
| Reward dependence | Sentimental | Practical |
| Attached | Detached | |
| Dependent | Independent | |
| Persistence | Persistent/hard-working | Inactive/unreliable |
| Self-directedness | Responsible | Blaming |
| Purposeful | Lacking goal direction | |
| Resourceful | Inert | |
| Self-accepting | Self-striving | |
| Good habits | Bad habits | |
| Cooperativeness | Accepting | Intolerant |
| Empathic | Disinterested | |
| Helpful | Unhelpful | |
| Compassionate | Revengeful | |
| Conscientious | Self-serving | |
| Self-transcendence | Self-forgetful | Self-conscious |
| Identifying with nature | Individualistic | |
| Spiritual | Rational |
The table is an adapted version of a descriptive table in Cloninger et al. Reference Cloninger, Przybeck, Svrakic and Wetzel27
Studies on Cloninger's definition of temperament and character in adult populations have repeatedly shown that ASD is associated with high harm avoidance and low self-directedness. Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14–Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 Also, low reward dependence, Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14,Reference Soderstrom, Rastam and Gillberg16,Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 low novelty seeking, Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14,Reference Soderstrom, Rastam and Gillberg16 low cooperativeness Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14–Reference Soderstrom, Rastam and Gillberg16 and high self-transcendence Reference Sizoo, van der Gaag and van den Brink15–Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 have been associated with ASD but not in a consistent manner. Considering subclinical ASD traits, negative associations with novelty seeking and reward dependence, and positive associations to harm avoidance have been demonstrated. Reference Kunihira, Senju, Dairoku, Wakabayashi and Hasegawa18 Yet, no studies examining possible differences in temperament and character between individuals with a clinical ASD diagnosis and subclinical ASD difficulties have been performed, despite the evidence that this is relevant for other neurodevelopmental disorders such as attention-deficit hyperactivity disorder (ADHD). Reference Faraone, Kunwar, Adamson and Biederman19
The possible influence of comorbid disorders on an association between personality dimensions and ASD also needs to be considered. ASD in combination with ADHD has been shown to be associated with high levels of novelty seeking when compared with individuals with ASD without ADHD. Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14 ASD combined with substance abuse has been shown to be associated with a higher degree of persistence and a lower degree of self-directedness compared with individuals with ASD and no substance abuse. Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 Individuals with ASD and former substance abuse scored higher regarding persistence than other individuals with ASD. There have to this date been no studies examining temperament and character in relation to ASD in combination with anxiety or mood disorders. In children, a combination of ASD and other neurodevelopmental disorders have been shown to be related to a combination of self-directedness and cooperativeness scores, with the children with a higher degree of comorbid diagnoses scoring lower on these scores, while also reporting greater suffering. Reference Garcia, Anckarsater and Lundstrom20
In summary, even though there is some knowledge on the relationship between temperament and character dimensions on the one hand and ASD on the other, very little is known on how such a relationship actually influences long-term outcome and functioning for individuals with clinical and subclinical presentations of ASD. There is also some evidence indicating that personality traits differ between ‘ASD pure’ (ASD with no comorbidity) and ‘ASD plus’ (ASD with comorbidity) groups (terms coined by Gillberg and Fernell Reference Gillberg and Fernell21 which suggests that ASD plus groups have worse outcome than ASD pure groups).
This study is a part of a large project focusing on the long-term outcome of males diagnosed with Asperger syndrome in childhood and followed up over two decades. In two recently published papers from the project, Reference Gillberg, Helles, Billstedt and Gillberg22,Reference Helles, Gillberg, Gillberg and Billstedt23 it was shown that 19 years after the original Asperger syndrome diagnosis, the group can be divided into three subgroups: i) those who no longer meet criteria of an ASD, ii) an ASD plus group and iii) an ASD pure group. The aim of the present study is to examine temperament and character in males who were diagnosed with Asperger syndrome in childhood and followed prospectively over almost two decades. First, temperament and character scores of the three groups will be compared with norm data. Second, temperament and character dimensions will be compared between the three groups mentioned above. Third, possible associations between temperament and character dimensions and general functioning, intelligence, severity of ASD symptoms, depressive symptoms and/or symptoms of ADHD will be investigated.
Method
Participants
Forty males with Asperger syndrome were included in this study. They were recruited in the following way. A group of 100 males with Asperger syndrome according to Gillberg and Gillberg Reference Gillberg and Gillberg24 criteria had been followed since their original diagnosis was established at a mean age of 11.4 years (T0). They had all been thoroughly assessed and have been found to be representative of all males diagnosed with Asperger syndrome in the greater Gothenburg area during the 1980s and 1990s. Reference Cederlund and Gillberg25,Reference Gillberg and Cederlund26
Of the 100 individuals, 76 agreed to participate at the first follow-up in 2002–2003 (at mean age of 20 years) (T1) Reference Cederlund, Hagberg, Billstedt, Gillberg and Gillberg1 and 50 agreed to participate at the second follow-up in 2011–2013 (at mean age of 30 years) (T2), 47 of whom participated at both T1 and T2. Seven individuals were not contacted because they had previously declared that they were not interested in participating, 1 had died since T1, 35 declined participation and 7 were unreachable. The participants at T2 differed from non-participants of the T1 group (N=29) on Full Scale IQ (FSIQ) and Performance IQ at T1 and from the non-participants of the T0 group (N=50) on Performance IQ at T0, with the T2 participants scoring significantly higher. Thorough attrition analysis has been presented in a previous publication. Reference Helles, Gillberg, Gillberg and Billstedt23
Of the 50 men, 40 completed the Temperament and Character Inventory (TCI) and were included in the analyses in this paper. Eight individuals declined to complete the TCI questionnaire (usually saying it was too long); one did not participate in the study himself but allowed us to interview his parents and because of this could not complete the TCI questionnaire; one TCI protocol was incorrectly administered and had to be removed. The mean age of the TCI participants at T0 was 11.5 years (s.d.=4.4, range 5.5–24.5 years), and mean age at T2 was 30.0 years (s.d.=4.8, range 23.7–43.9 years), respectively. The average FSIQ at T2 was 110.2 (s.d.=14.4, range 84–140).
Among the 40 participants, three subgroups have emerged in the previously published studies: no longer ASD (n=8), ASD only (we opted to use the term ‘ASD only’ instead of ‘ASD pure’ as more neutral sounding) (n=11) and ASD plus (n=21). The no longer ASD group consisted of individuals who at T2 no longer met criteria of any ASD even though they did so at T0 and in most cases also at T1. Reference Helles, Gillberg, Gillberg and Billstedt23 The ASD plus group consisted of individuals with a stable ASD over two decades who at T2 met criteria for at least one of the following psychiatric disorders: depression, panic disorder, social phobia, general anxiety disorder, ADHD, obsessive–compulsive disorder or alcohol dependence. Reference Gillberg, Helles, Billstedt and Gillberg22 The ASD only group consisted of individuals with a stable ASD diagnosis throughout the follow-up period and no comorbid psychiatric diagnoses.
Attrition
There were no significant differences between those 40 who completed the TCI and the 10 who did not as regards age, FSIQ, or on scores from Asperger Syndrome Diagnostic Interview (ASDI), ADHD Self Report Scale (ASRS), Global Assessment of Functioning (GAF), Beck Depression Inventory (BDI), or as regards ASD diagnostic group status at T2. There were missing answers for one item on five questionnaires, and missing answers for two to eight items on four questionnaires, but no individual had more missing answers on the TCI than is allowed (max missing allowed 12). Reference Cloninger, Przybeck, Svrakic and Wetzel27 Missing answers were not replaced.
Procedure
In the T2 study, performed in 2011–2013, the group was contacted by mail and phone, reminded of the follow-up and asked to participate. The research team comprised a psychiatrist and a clinical psychologist, both with extensive experience in the field of ASD and other developmental disorders. In all cases but one (home visit), data were collected during a 4–6 h visit to the Gillberg Neuropsychiatry Centre. The data collection included results of clinical interviews, IQ tests and self-report measures, including the TCI. All assessments were made blind to results from T1.
Participation was preceded by participants providing written, informed consent. Ethical approval had been obtained from the Regional Ethical Approval Board in Gothenburg (reference: 508-10).
Measures at T2
Temperament and character dimensions
The TCI Reference Cloninger, Przybeck, Svrakic and Wetzel27 is a self-rating questionnaire measuring seven personality dimensions that are divided into four temperament dimensions (‘harm avoidance’, ‘novelty seeking’, ‘reward dependence’ & ‘persistence’) and three character dimensions (‘self-directedness’, ‘cooperativeness’ & ‘self-transcendence’). ‘Rare answers’ is also presented as a separate scale and is a collection of unusual answers that are associated with low social skills and odd or bizarre personality traits. All scores are presented as T-scores based on Swedish norm samples Reference Gillberg and Cederlund26 with a mean of 50 and a standard deviation of 10. Higher scores indicate higher levels of the temperament or character trait. The TCI has been proven to have good test–retest reliability, consistency with interview ratings and have high internal consistency. Reference Cederlund and Gillberg25 The TCI original version with dichotomous answers (true/false) was used and scored using the TCI software. Reference Brändström, Sigvardsson, Nylander and Richter28
Psychiatric and neurodevelopmental symptoms
The ASDI, Reference Gillberg, Gillberg, Rastam and Wentz29 a semi-structured clinical interview for use with an adolescent or adult with suspected Asperger syndrome relating to symptoms of the disorder, with scores ranging from 20 to 60 (high scores indicating more ASD symptoms), was used to assess ASD symptoms. The BDI Reference Beck and Steer30 was used to assess depressive symptoms. Scores range from 0 to 63 with scores of 14–19 indicating mild depression, scores of 20–28 indicating moderate depression and scores of 29–63 indicating severe depression. The ASRS Reference Kessler, Adler, Gruber, Sarawate, Spencer and Van Brunt31 is a self-report questionnaire for assessment of ADHD symptoms. In this study, only part A (score range 0–6) was used, with scores of 4–6 indicating presence of ADHD.
General functioning
The GAF 32 was used to measure general functioning, with scores of 70 and above indicating good functioning or only mildly abnormal psychosocial situation.
IQ
The Wechsler Adult Intelligence Scale, 3rd edition (WAIS-III) Reference Wechsler33 was used to assess FSIQ.
Statistical analysis
All data analysis was done with IBM SPSS Statistics for Windows, Version 22.0 (IBM Corp, Armonk, NY, USA). Normal distribution and linear associations could not be assumed (i.e. non-parametric statistics were used). All significance tests were two-tailed, and significance level was set at P<0.05. Comparisons with norm data were made with one-sample t-test comparing the subgroup mean with the normative sample mean of 50 with a standard deviation of 10. Group comparisons between the no longer ASD, ASD only and ASD plus subgroups were made with the Kruskal–Wallis H test and Dunn's post hoc test. Correlation analyses between TCI factor scores and WAIS-III, GAF, ASRS and ASDI scores were made with Spearman's rho. All results with P-values below 0.05 are presented and values considered statistically significant are in bold. Effect sizes from Spearman's rho are considered strong if rho≥0.5, moderate if rho≥0.3 and weak if rho≥0.1. To minimise the risk of type I errors in the correlation, an automated bootstrapping technique in the SPSS software was used with 1000 samples and simple sampling. To be considered statistically significant, both the P-values were below 0.05 and the bootstrap 95% confidence interval did not overlap 0. Reference Haukoos and Lewis34
Results
Temperament and character compared with norm data
The results from the groups were compared with norm data with a mean of 50 and a standard deviation of 10 (Fig. 1). The no longer ASD group scored higher than norms on reward dependence (t=2.9, P=0.025). The ASD only group scored lower than norms on novelty seeking (t=−3.2, P=0.009) and higher on harm avoidance (t=2.8, P=0.020). The ASD plus group scored higher than norms on harm avoidance (t=7.0, P<0.001) and rare answers (t=6.6, P<0.001) and lower on self-directedness and cooperativeness. Generally, the ASD plus group was most deviant on temperament and character dimensions compared with norms.
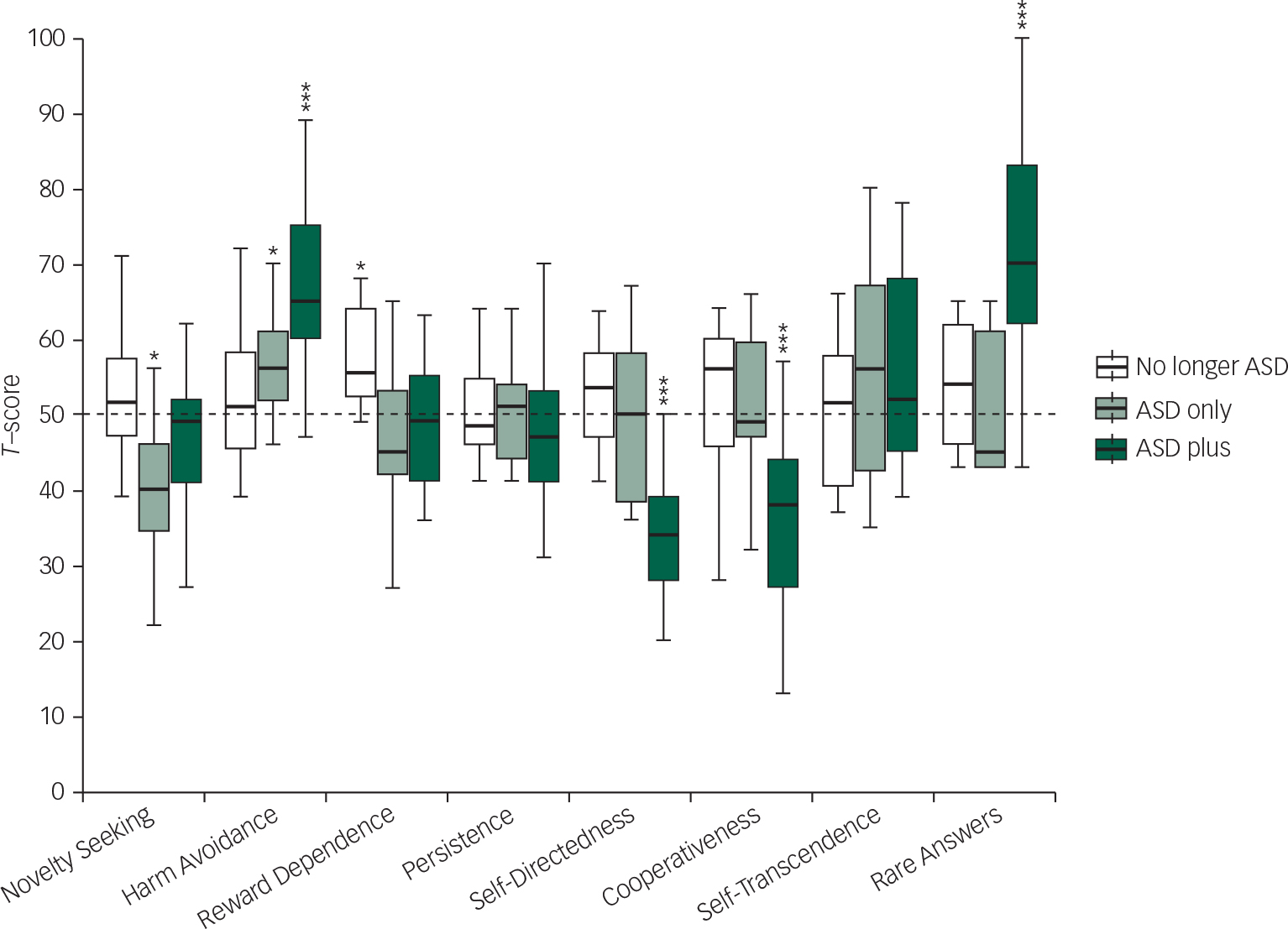
Fig. 1 Temperament and character dimensions compared with norm data with a one-sample t-test, presented in a Tukey boxplot. The boxplot represents medians (line in box), 25th and 75th quartiles (outer lines of box) and 1.5 IQR above and below quartiles (end of whiskers). The statistical analysis was based on means, but boxplots were presented to better represent the variance of the data. Outliers have been removed to enhance readability (there were no extreme outliers). In the ASD only group, there were two outliers, one below regarding reward dependence and one below regarding cooperativeness. In the no longer ASD group, there was one outlier below regarding self-directedness and in the ASD plus group there was one outlier above regarding self-directedness. *= significant difference from norm data at P<0.05; **= significant difference from norm data at P<0.01; *** significant difference from norm data at P<0.001.
Temperament and character in relation to ASD diagnostic stability and psychiatric comorbidity
The three subgroups differed significantly from each other on all TCI scales except persistence and self-transcendence (Table 2). Post hoc analyses showed that the ASD plus group scored higher than both other groups on harm avoidance and rare answers and lower on self-directedness and cooperativeness. The no longer ASD group scored higher on reward dependence compared with both the other groups, while the ASD only group scored significantly lower on novelty seeking than the no longer ASD group. The largest differences in T-scores were found for the ASD plus group, in some cases with a deviance of almost or more than two standard deviations (harm avoidance, self-directedness and rare answers) from norms.
Table 2 Temperament and character in relation to ASD diagnostic stability and psychiatric comorbidity
| TCI | No longer ASD (n=8) | ASD only (n=11) | ASD plus (n=21) | Kruskal–Wallis H test chi-2 (P) |
No longer ASD v. ASD only
a
Z (P) |
No longer ASD v. ASD plus
a
Z (P) |
ASD only v. ASD plus
a
Z (P) |
|||
|---|---|---|---|---|---|---|---|---|---|---|
| Md | Q1–Q3 | Md | Q1–Q3 | Md | Q1–Q3 | |||||
| Temperament dimensions | ||||||||||
| Novelty seeking | 51.5 | 45.0–63.8 | 40.0 | 33.0–47.0 | 49.0 | 40.0–52.0 | 6.1 (0.046) | 2.4 (0.015) | 1.2 (0.099) | − 1.7 (0.212) |
| Harm avoidance | 51.0 | 44.5–58.8 | 56.0 | 52.0–62.0 | 65.0 | 58.5–77.0 | 11.7 (.003) | − 0.7 (0.530) | − 3.0 (0.003) | − 2.5 (0.011) |
| Reward dependence | 55.5 | 50.8–66.0 | 45.0 | 40.0–58.0 | 49.0 | 41.0–55.0 | 6.1 (.048) | 2.3 (0.020) | 2.1 (0.034) | − 0.5 (0.586) |
| Persistence | 48.5 | 46.0–58.3 | 51.0 | 42.0–55.0 | 47.0 | 41.0–53.0 | 1.2 (0.549) | b | b | b |
| Character dimensions | ||||||||||
| Self-directedness | 53.5 | 43.0–58.0 | 50.0 | 37.0–61.0 | 34.0 | 26.5–40.5 | 14.0 (0.001) | − 0.4 (0.972) | 2.9 (0.004) | 3.2 (0.002) |
| Cooperativeness | 56.0 | 39.3–60.0 | 49.0 | 46.0–61.0 | 38.0 | 25.5–45.0 | 9.6 (0.008) | 0.2 (0.811) | 2.5 (0.012) | 2.5 (0.012) |
| Self-transcendence | 51.5 | 39.5–61.3 | 56.0 | 41.0–68.0 | 52.0 | 43.0–69.0 | 0.7 (0.707) | b | b | b |
| Rare answers | 54.0 | 44.0–64.0 | 45.0 | 43.0–61.0 | 70.0 | 61.5–83.0 | 15.0 (0.001) | 0.4 (0.687) | − 2.7 (0.007) | − 3.5 (<0.001) |
TCI, Temperament and Character Inventory; ASD, autism spectrum disorder.
a Dunn's post hoc test.
b Post hoc analysis is not possible when Kruskal–Wallis is non-significant.
Numbers in bold are statistically significant.
Associations between temperament and character and psychiatric/neurodevelopmental symptoms, IQ and general functioning
There were associations between several of the temperament and character dimensions and general functioning and psychiatric/neurodevelopmental symptoms (Table 3). However, no associations with FSIQ were found. The strongest correlations were demonstrated for self-directedness and BDI scores (negative association), cooperativeness and GAF scores (positive association) and rare answers and BDI scores (positive association).
Table 3 Associations (Spearman's rho) between temperament and character dimensions and psychiatric/neurodevelopmental symptoms, intelligence and general functioning (n=40)

| Temperament and Character Inventory | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| NS | HA | RD | PE | SD | CO | ST | RA | ||
| GAF | rho (P) | ns | −0.469 (0.003) | 0.365 (0.026) | 0.337 (0.042) | ns | 0.558 (<0.001) | ns | −0.344 (0.037) |
| WAIS-III FSIQ | rho (P) | ns | ns | ns | ns | ns | ns | ns | ns |
| ASDI score | rho (P) | −0.471 (0.003) | ns | ns | ns | ns | −0.351 (0.033) | ns | ns |
| ASRS score | rho (P) | ns | ns | ns | ns | ns | −0.418 (0.004) | ns | 0.445 (0.006) |
| BDI Total score | rho (P) | ns | 0.442 (0.006) | ns | ns | −0.662 (<0.001) | −0.372 (0.023) | ns | 0.639 (<0.001) |
NS, novelty seeking; HA, harm avoidance; RD, reward dependence; PE, persistence; SD, self-directedness; CO, cooperativeness; ST, self-transcendence; RA, rare answers; ns, non-significant; GAF, Global Assessment of Functioning; WAIS-III, Wechsler Adult Intelligence Scale, 3rd edition; FSIQ, Full Scale Intelligence Quotient; ASDI, Autism Spectrum Diagnostic Interview; ASRS, ADHD Self-Report Scale; BDI, Beck Depression Inventory.
Numbers in bold are statistically significant.
Discussion
In the present study, we found a clear association between temperament and character dimensions on the one hand and long-term ASD diagnostic stability and psychiatric comorbidity on the other. The participants who no longer met criteria for ASD in adult life (the no longer ASD group) were characterised by high reward dependence (usually associated with being warm, attached and socially dependent), both compared with the other groups and compared with norm data, and fairly average scores on the other temperament dimensions.
The participants with a stable ASD and no current psychiatric comorbidity (the ASD only group) were characterised by lower-than-average novelty seeking (usually associated with being indifferent, reflective, detached and orderly), both compared with norm data and to the no longer ASD group, and higher than average on harm avoidance (usually associated with worrying, being fearful, shy and fatigable), compared with norm data but not to the other groups and clearly lower on this measure than the ASD plus group, and fairly average scores on the other TCI dimensions.
The ASD plus group, those with a stable ASD and at least one other current psychiatric disorder (usually depression, anxiety disorder and/or ADHD), was the most deviant in temperament and character dimensions, both compared with the other diagnostic groups and with norm data. They were characterised by elevated harm avoidance scores (usually associated with worrying, and being fearful, shy and fatigable), one and a half standard deviations above norm data and higher than both the other subgroups, and low self-directedness (usually associated with being immature, blaming others for one's own misfortunes, having low sense of purpose, being ineffective and having trouble adjusting habits to reach long-term goals). Also, their cooperativeness scores (usually associated with being socially intolerant, critical, unhelpful, revengeful and opportunistic) were around one and a half standard deviations below norm data and lower than both of the other subgroups. They also had a high degree of rare answers (usually associated with low social skills and an odd personality), more than two standard deviations above norm data and higher than both other subgroups.
Compared with other TCI-studies on adults with ASD, our results differ somewhat. The results of the ASD plus group are similar to previous studies Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14–Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 in that they also reported high harm avoidance and low self-directedness and cooperativeness but differ in the sense that previous studies found lower levels of novelty seeking, reward dependence and self-transcendence. The ASD only group showed similar temperament traits as other studies with low novelty seeking and high harm avoidance, but differed in having average reward dependence. Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14,Reference Soderstrom, Rastam and Gillberg16 They also differed regarding the character dimensions with all three dimensions being in the average range, when usually cooperativeness and self-directedness are low and self-transcendence is high in ASD populations. Some of these differences might be due to methodological differences. One significant difference in this study compared with other studies published in this research field is that we have subdivided our ASD population based on a broad range of psychiatric comorbidity. In the Anckarsater et al, Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14 study subdivision by groups was based on comorbid ADHD, and in the Sizoo et al Reference Sizoo, van den Brink, Gorissen van Eenige and van der Gaag17 study subdivision was based on substance abuse. Both these studies showed that temperament and character differs somewhat when ASD is combined with a comorbid disorder. None of the other studies have included mood or anxiety disorders as a possible comorbid diagnosis. The sampling also differed from our study compared with others, in that ours is a longitudinal cohort study, with some of the participants not having contact with any psychiatric clinic, whereas the other studies have mostly used psychiatric out-patients with ASD, that is, most probably belonging to the ASD plus group. Our results emphasise the importance of controlling for comorbid disorders when examining personality in adults with ASD but also to include non-psychiatric patients. The correlation analysis between TCI dimensions and ASD, ADHD and depression symptoms further add to the relationship between TCI dimensions and psychiatric symptoms.
In previous studies on this group of males with Asperger syndrome, Reference Gillberg, Helles, Billstedt and Gillberg22,Reference Helles, Gillberg, Gillberg and Billstedt23 we have shown that the no longer ASD group is somewhat less prone to develop psychiatric comorbidity and have lower degree of ASD symptoms in adolescence/young adulthood, but that the subgroups are very similar on a number of factors, including age at diagnosis and IQ. The result of this study might add an important piece to the puzzle of understanding why some individuals with Asperger syndrome in childhood no longer fulfil an ASD in adult life. The no longer ASD group scored significantly higher on reward dependence, a temperament trait associated with seeking approval from one's peers and being attached to other individuals. We hypothesise that this aspect is important in developing social skills for individuals with ASD because they are probably more likely to seek out social interaction and try to fit in with their peers, thus promoting naturalistic social skills training. The lower harm avoidance probably also adds to the social development seen in this group. Being less worried, shy and fearful probably leads to not avoiding difficult situations, thus promoting positive development. The relationship between harm avoidance, reward dependence and diagnostic stability in ASD is something that should be studied further in future research. One could argue the opposite of our hypothesis, that is, that the general positive development led to a decrease in ASD symptoms – which in turn led to the development of prosocial temperament traits. Because of the cross-sectional design of this study, it is not possible to determine causality. The theories behind the TCI Reference Cloninger, Svrakic and Przybeck9,Reference Cloninger10 suggest that temperament and character traits are fairly stable from young age and are highly hereditary, thus giving some support to our hypothesis. This emphasises the need for future studies with longitudinal analysis of the relationship between temperament and character and ASD diagnostic stability.
The results of analyses in the ASD plus group, especially compared with the ASD only group, suggest that temperament and character dimensions might be mediating factors in developing psychiatric comorbidity in an ASD population. High harm avoidance and low self-directedness are especially common traits in psychiatric populations, Reference Fassino, Amianto, Sobrero and Abbate Daga11 and both dimensions were associated with depressive symptoms (and any psychiatric comorbidity) in this sample. Cooperativeness was negatively associated with a number of factors (ASD symptoms, ADHD symptoms and depressive symptoms) and positively associated with general functioning in this sample. These results are in line with other studies as cooperativeness has repeatedly been shown to be associated with poor mental health, but to a lesser extent than harm avoidance and self-directedness. Reference Fassino, Amianto, Sobrero and Abbate Daga11
The highly elevated rate of rare answers in the ASD plus group is also of interest. Psychiatric patients generally have higher amounts of rare answers Reference Cloninger, Przybeck, Svrakic and Wetzel27 but the ASD plus group had extremely high scores on this scale, which has been reported previously. Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14,Reference Soderstrom, Rastam and Gillberg16 The rare answers are related to an odd or bizarre personality and these odd responses seem to be specific to individuals with ASD and psychiatric comorbidity. A combination of being anxious, having low belief in one-self and others, while being perceived as odd, might be factors that all contribute to developing psychiatric symptoms in adults with ASD. It is possible to argue the reverse of our hypothesis because of the difficulty of assessing causality in cross-sectional studies. Perhaps it is because of comorbidity during childhood/adolescence that more negative personality traits have developed. However, one could once again argue that the theory behind TCI gives support to the notion that temperament traits precede negative development later in life.
Low novelty seeking has been shown to differ between individuals with ASD and individuals with ASD and ADHD combined Reference Anckarsater, Stahlberg, Larson, Hakansson, Jutblad and Niklasson14 and it is possible that the differences between the ASD only and ASD plus groups on this measure is due to the fact that the ASD plus group included several individuals with ASD and ADHD combined. The results regarding novelty seeking, especially the negative correlation with ASDI scores, might indicate that low Novelty Seeking is a core feature of ASD, regardless of psychiatric comorbidity, except when combined with ADHD.
Because of the fairly small sample size, no analyses have been made on the TCI subscales or temperament types that might have given further insight into understanding temperament and character dimensions in this cohort. This should be an area of interest for further research.
The clinical implication of the study is that the TCI presents personality traits that might indicate early signs of positive or negative development in individuals with ASD. Prosocial traits might be a factor that indicates if optimal outcome is possible, whereas odd characteristics, excessive worrying, low self-esteem and distrust of others might be indications of a high-risk patient.
A limitation of this study is that even though the design is longitudinal, the analyses have been mostly cross-sectional, that is, we only have information on temperament and character in adult life. Thus, we cannot draw conclusions regarding causation. On the other hand, temperament traits have been shown to be stable over time, Reference Sigvardsson, Bohman and Cloninger35,Reference Josefsson, Jokela, Cloninger, Hintsanen, Salo and Hintsa36 even from childhood, Reference Sigvardsson, Bohman and Cloninger35 whereas character traits tends to change over time. Reference Josefsson, Jokela, Cloninger, Hintsanen, Salo and Hintsa36 This means that we might be able to see signs of differing trajectories at an early age, with children showing personality traits marked by sociability perhaps being on a more positive developmental path whereas children with personality traits marked by worrying and shyness might be on a path to a more negative development. This is something that should be examined further in young populations with ASD followed longitudinally and should be possible with the recent addition of the Junior-TCI. Reference Kerekes, Brandstrom, Stahlberg, Larson, Carlstrom and Lichtenstein37
Another limitation is the high attrition rate (only 40 out of the 100 in the original cohort and 40 out 50 in the second follow-up participated in this study). The group that participated in the present study differed from the total cohort (n=100) in that they had higher IQ in childhood/adolescence, perhaps indicating that the sample in this study functions somewhat better compared with the total cohort. However, within the sample studied FSIQ was not associated with any temperament or character dimension, suggesting that perhaps the difference in IQ might be of minor importance in this context. As there were no significant differences between those who did (n=40) and did not fill out the TCI (n=10), the results from this study can probably be generalised at least to all participants in the second follow-up.
Last, it is important to note that there were only male participants in this study, that is, any conclusions can only be made as regards males with a childhood diagnosis of Asperger syndrome.
Funding
The study was supported by funding from the Centre for Research and Development in Gavleborg and the Child and Adolescent Psychiatric Clinic in Gavle, VG Region Scientific Fund, AnnMarie and Per Ahlqvist Foundation, the Jerring Fund, Wilhelm and Martina Lundgren Foundation, Petter Silfverskiold Foundation, Region Kronoberg, Golje Foundation, the Swedish Child Neuropsychiatry Science Foundation and the Gillberg Neuropsychiatry Centre.





 Open access
Open access
eLetters
No eLetters have been published for this article.