



Economic inequality − the unequal distribution of resources and opportunities in different social domains such as education, employment and income within societies − has been one of the most challenging issues of recent decades. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1,Reference Pickett and Wilkinson2 Inequality threatens social and economic development and adversely affects the individual’s sense of fulfilment and self-worth. 3 Moreover, this might be associated with an increased risk of poor mental health. Reference Ribeiro, Bauer, Andrade, York-Smith, Pan and Pingani4–Reference Patel, Saxena, Lund, Thornicroft, Baingana and Bolton6
Several studies have focused on objective economic inequality (e.g. Gini coefficient) in understanding how economic inequality could impact mental health. Reference Ribeiro, Bauer, Andrade, York-Smith, Pan and Pingani4,Reference Patel, Burns, Dhingra, Tarver, Kohrt and Lund5 Previous systematic reviews and meta-analyses have shown that economic inequality negatively affects mental health. Reference Ribeiro, Bauer, Andrade, York-Smith, Pan and Pingani4,Reference Patel, Burns, Dhingra, Tarver, Kohrt and Lund5 Although objective measures of inequality can explain how different socioeconomic positions affect population mental health, people may not always perceive the same level of inequality in society. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1,Reference Schmalor and Heine7 Perception of economic inequality refers to how individuals perceive the distribution of resources within society through everyday interactions and social comparisons. Reference Castillo, García-Castro and Venegas8 Previous studies reported that the perception of economic inequality was associated with well-being Reference Du, Huang, Ma, Chen, Chi and King9,Reference Oshio and Urakawa10 and mental health. Reference Kim11–Reference Zhang, Wang, Zhang, Wei, Jian and Guo13 Understanding the psychological impact of economic inequality should also consider its perceived component. Reference Schmalor and Heine7
Young adulthood is a period when individuals face the challenges of transitioning into adulthood within a society. Reference Pegado, Alvarez and Roberto14 During this phase, individuals may experience social and environmental changes through socialisation and social interaction. Reference Conley, Shapiro, Huguenel and Kirsch15,Reference Newman, Moffitt, Caspi, Magdol, Silva and Stanton16 Through these processes, the psychological impact of economic inequality may be stronger for young adults; Reference Dorling, Mitchell and Pearce17 they may be more influenced or motivated in their beliefs about future mobility by social contexts, such as income inequality and intergenerational mobility, through everyday interactions and social comparisons. Reference Castillo, García-Castro and Venegas8,Reference Kim11,Reference Lierse18,Reference Browman, Destin, Kearney and Levine19 Furthermore, young adults may be at a heightened risk for adverse mental health outcomes when they face multiple new challenges, including increased financial responsibility and distress, particularly in economically challenging environments. Reference Achdut20 This highlights the mental health consequences of economic factors, making the case for examining economic pressures and inequalities among young adults even more compelling.
However, few studies have investigated the association between perceived economic inequality and mental health among young adults and demonstrated mixed findings. Reference Kim11,Reference H-l and Shim12 One previous study showed that young adults with higher perceptions of economic inequality are more likely to experience poor mental health, such as anxiety and depression, Reference H-l and Shim12 while another found no statistically direct association. Reference Kim11 Thus, further investigation is needed to identify the association of different economic inequality perceptions (e.g. inequality of intergenerational mobility) with various public mental health indicators among young adults (e.g. suicide ideation). Moreover, few studies have provided evidence on whether the association between perceived economic inequality and mental health varies by socioeconomic status (SES). Reference Du, Huang, Ma, Chen, Chi and King9 One previous study, conducted in a specific region in China, showed that neither objective nor subjective SES intensified or mitigated the association between perceived inequality and well-being among college students. Reference Du, Huang, Ma, Chen, Chi and King9 Further investigation into mental health is needed using nationally representative samples among young adults.
In South Korea, with a population of about 52 million people, objective economic inequality has increased in the last 30 years, with a gradual decline in the proportion of total income for the low- and middle-income classes but increases for the high-income class. Reference Chancel, Piketty, Saez and Zucman21 Moreover, a term called ‘spoon class’ has become popular among young people, suggesting that parental SES determines their children’s SES. In South Korea, the spoon class metaphor could refer to public dissatisfaction with stagnant upward social mobility among young people. Reference Kang and Park22 In the meantime, South Korea recently showed the highest prevalence of depression and suicide mortality rates among Organisation for Economic Co-operation and Development (OECD) countries in 2020. 23 This suggests that South Korea provides a unique context in which to investigate the association between perceived economic inequality and mental health among young adults.
Therefore, we aimed to (a) investigate the association between perceived economic inequality and mental health and (b) examine whether this association differs by individual objective and subjective income level among young adults aged 19−34 years in South Korea.
Method
Data and study sample
We used data from the Survey of Korean Youths’ Lives, a nationally representative, cross-sectional study of young adults aged 19−34 years in South Korea. The Survey of Korean Youths’ Lives was conducted in 2022 by the Office for the Prime Minister’s Secretariat and the Korea Institute for Health and Social Affairs, to understand and improve the well-being of young adults. Reference Cheong, Ryoo, Kang, Kim, Ham and Kim24 The survey used a stratified, two-stage sampling design. The first stage involved selecting administrative districts (si-gun-gu) and the second involved selecting households and individuals aged 19–34 years to ensure that the sample was representative of young adults aged 19–34 years in South Korea. Reference Cheong, Ryoo, Kang, Kim, Ham and Kim24 In this survey, a wide range of information was collected about their life conditions, including perceived economic inequality, SES and health-related behaviour and status. Further information on this survey is available elsewhere. Reference Cheong, Ryoo, Kang, Kim, Ham and Kim24 We obtained the data provided by Statistics Korea through the MicroData Integrated Service website in October 2023 (https://mdis.kostat.go.kr [in Korean]). Of the 14 966 young adults who participated in the survey, we excluded those with missing information (n = 48), resulting in a final sample of 14 918 participants.
Depressive symptoms and suicide ideation
Outcome variables were depressive symptoms and suicide ideation. Depressive symptom was measured with Patient Health Questionnaire-9 (PHQ-9), asking participants to report their depressive symptoms over the past 2 weeks using 9 items. Reference Löwe, Kroenke, Herzog and Gräfe25 Each item was rated on a 4-point Likert scale from 0 to 3, where 0 represents ‘none’ and three represents ‘almost every day’. These scores were summed for the overall PHQ-9 score, which ranges from 0 to 27. Respondents with a total PHQ-9 score >10 were considered to have depressive symptoms. Reference Choi, Choi, Park, Joo, Ga and Ko26 Suicide ideation was measured using a single question, as used by previous studies: Reference Choi, Ki, Yip, Park, Song and Lee27–Reference Nahrin, Al-Mamun, Kaggwa, Al Mamun and Mamun30 ‘Have you ever seriously considered dying by suicide over the past year?’ Respondents who reported ‘Yes’ to the question were considered as having experienced suicide ideation.
Perceived income inequality and perceived inequality of intergenerational mobility
Perception of economic inequality covers various aspects such as income, wealth, economic opportunities and social mobility. Reference Castillo, García-Castro and Venegas8 Our main explanatory variables of perceived economic inequalities were perceived income inequality and perceived inequality of intergenerational mobility. Perceived income inequality was assessed by a single question: ‘How would you assess the current level of income inequality in South Korea?’ on an 11-point scale, where 0 indicates no inequality and 10 indicates very severe inequality, similar to previous studies. Reference Oshio and Urakawa10,Reference Kim11 Perceived inequality of intergenerational mobility was measured by a single question: ‘To what extent do you think parental income influences their children’s income?’ on an 11-point scale, where 0 represents no influence and 10 represents complete influence. We transformed the answers (perceived income inequality: mean 6.9, median 7.0; perceived inequality of intergenerational mobility: mean 7.1, median 7.0) into dichotomous variables, classifying them as either high or low inequality based on the sample median (value 7.0), a common dichotomisation approach. Reference Altman and Royston31
Covariates
To account for previously identified covariates of depressive symptoms and suicide ideation in the multivariate analysis, demographic, SES and health-related variables were included as covariates based on previous studies. Reference Choi, Ki, Yip, Park, Song and Lee27–Reference Choi, Sempungu, Kim, Han and Lee29,Reference Lee, Hahm and Park32–Reference Graham and Ciciurkaite37 For SES covariates, objective income, subjective income, education level and employment status were included. Reference Choi, Lee, Sempungu and Lee28,Reference Choi, Sempungu, Kim, Han and Lee29,Reference Lee, Hahm and Park32,Reference Akhtar-Danesh and Landeen36,Reference Graham and Ciciurkaite37 Objective income was assessed by asking participants to report their actual annual income (median 19 090 000 KRW; mean 19 234 262 KRW). We categorised the reported income into binary groups (high or low) based on the median value. Reference Altman and Royston31 Subjective income was assessed by asking respondents to evaluate their perceived income, which was classified as high, high-middle, middle, low-middle or low. We then transformed the responses (mean 3.24; median 3.0) into dichotomous variables, categorising them as either high subjective income (high, high-middle and middle) or low subjective income (low and low-middle) based on the median value. Reference Altman and Royston31 Education level was categorised based on the current level of education (elementary school, middle school, high school, college, university and graduate school), and we grouped this into ‘high school or below’ and ‘college or higher’ for this study. Reference Choi, Lee, Sempungu and Lee28,Reference Choi, Sempungu, Kim, Han and Lee29 Employment status was grouped into three categories: employed, unemployed and economically inactive. Other demographic covariates included sex (male and female), age group (19−29 and 30−34 years), marital status (single and married) and household size (1, 2−3 and 4+ persons); health-related covariates included subjective health status (very good/good and moderate to very poor), current smoking (yes and no) and heavy drinking (yes and no). Reference Choi, Ki, Yip, Park, Song and Lee27,Reference Choi, Sempungu, Kim, Han and Lee29,Reference Schmidt, Golden, Gottfredson, Ennett, Aiello and Ribisl34,Reference Weitzman35
Statistical analysis
First, a descriptive analysis of the study participants was conducted using chi-square tests. We then calculated the prevalence of depressive symptoms and suicide ideation by category in each explanatory variable and covariate, and used Rao−Scott chi-square tests to examine bivariate associations. Third, to assess the association of perceived economic inequalities with depressive symptoms and suicide ideation, we conducted a multivariate logistic regression analysis to estimate the odds ratio and its 95% CI. Specifically, we included perceived income inequality and perceived inequality of intergenerational mobility in the same model and analysed depressive symptoms and suicidal ideation separately. The analysis was adjusted for all confounding variables, including gender, age group, education, employment status, subjective income, objective income, marital status, number of household members, region, subjective health, current smoking and heavy drinking, because there was no statistical evidence of multicollinearity (data not shown). Additionally, we conducted the same analyses using continuous variables before dichotomisation, including perceived income inequality, perceived inequality of intergenerational mobility, quintile objective income and subjective income as a sensitivity analysis. Last, subgroup analysis of the association of perceived economic inequalities with depressive symptoms and suicide ideation was conducted by objective and subjective income (high or low). We also conducted an interaction test by including interaction terms in the multivariate models. In all analyses, except for chi-square tests of the general characteristics of the sample, we applied sample weights provided to all study participants to represent the young adult population aged 19−34 years in South Korea. All analyses were performed using SAS 9.4 software for Windows (SAS Institute, Cary, NC, USA; see https://www.sas.com). We considered statistical significance at two-sided P-values <0.05. Because this study used publicly available secondary data, ethical approval for the research was waived by the Institutional Review Board (IRB) of Korea University (approval no. KUIRB-2024-0298-01), and participant consent was not required.
Results
Table 1 shows the general characteristics of the study participants aged 19−34 years. Among 14 918 young adults, 862 (5.8%) and 355 (2.4%) individuals had depressive symptoms and suicide ideation, respectively. A different distribution of categories was observed for each variable, except for objective income. Table 2 presents the weighted prevalence of depressive symptoms and suicide ideation for each exposure variable and covariate. The weighted prevalence of depressive symptoms and suicide ideation was about two times higher in young adults who perceived economic inequalities, including both high inequality in income and intergenerational mobility. For example, 9.0% (95% CI 7.9, 10.0) of those perceiving high income inequality reported depressive symptoms, compared with 4.5% (95% CI 3.9, 5.0) of those perceiving low inequality. Similarly, 3.6% (95% CI 3.0, 4.2) of those perceiving high intergenerational mobility inequality reported suicide ideation, compared with 1.4% (95% CI 1.1, 1.7) for those perceiving low inequality. Regarding income level, young adults with low subjective income had higher rates of depressive symptoms and suicide ideation than those with high subjective income (e.g. suicide ideation: 1.7 v. 4.0%, P < 0.001). However, no significant difference was found for depressive symptoms based on objective income (i.e. 6.4 v. 5.8%, P = 0.22).
Table 1 General characteristics of the study sample
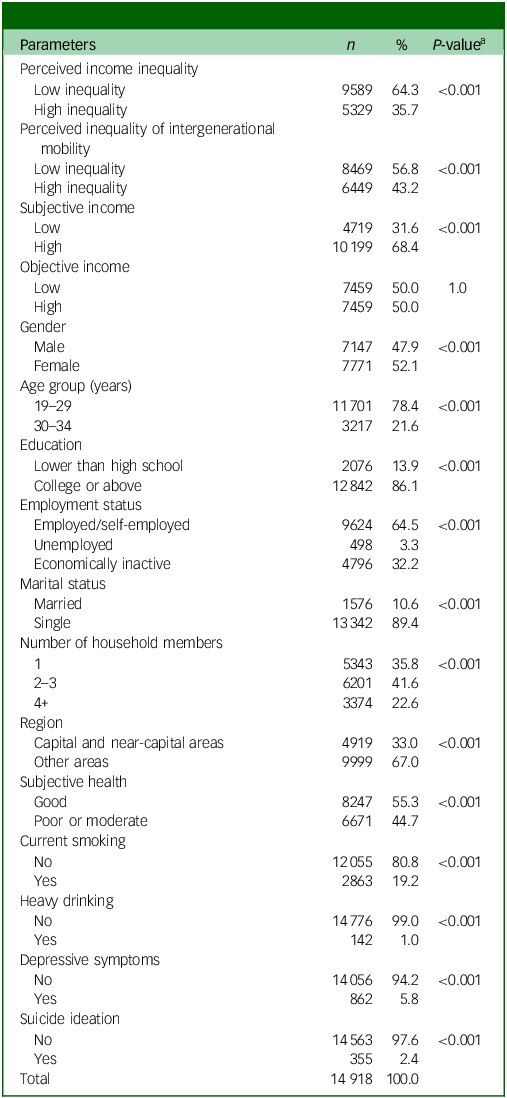
a P-value represents the difference in the distribution of categories for each variable.
Table 2 Weighted prevalence (95% CI) of depression symptoms and suicide ideation by perceived economic inequality
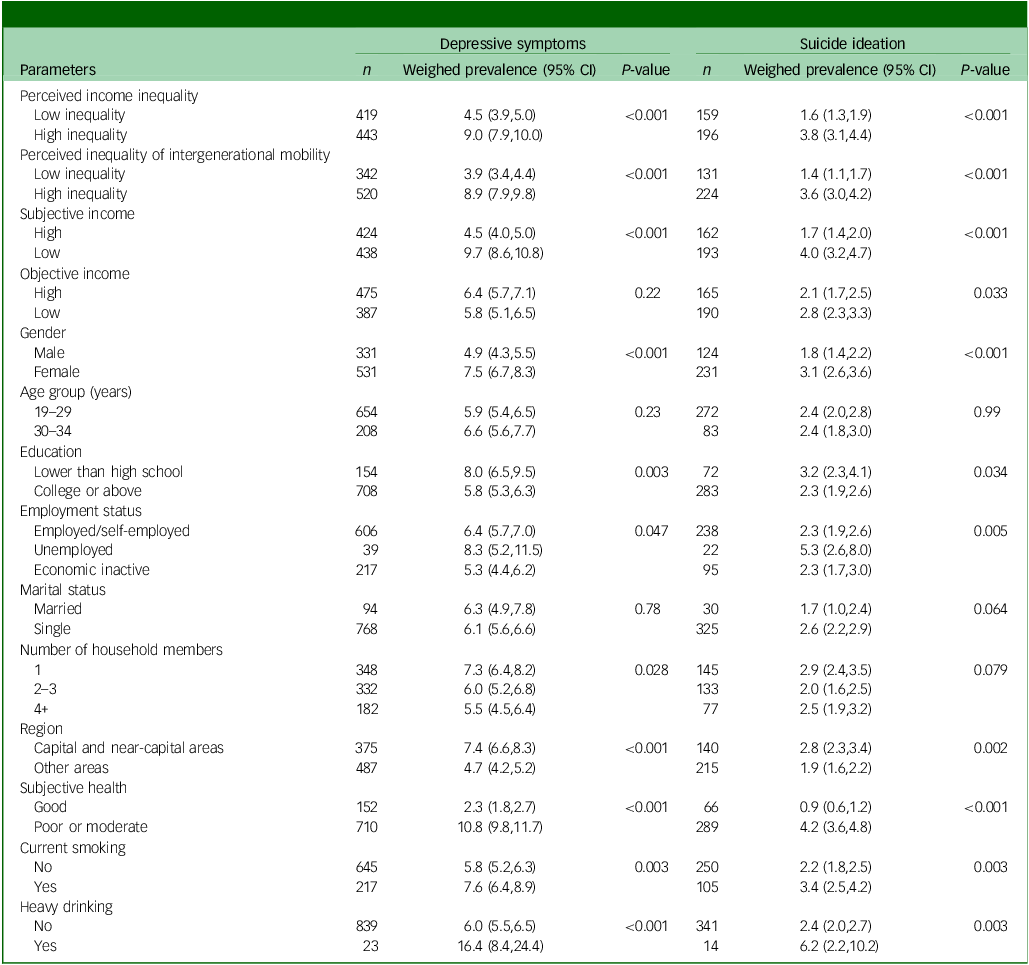
Table 3 shows the multivariate associations between perceived economic inequalities and depressive symptoms/suicide ideation. After accounting for all covariates (gender, age group, education, employment status, subjective income, objective income, marital status, number of household members, region, subjective health, current smoking and heavy drinking), young adults perceiving high income inequality were more likely to have both depressive symptoms (odds ratio 1.40, 95% CI 1.14, 1.71) and suicide ideation (odds ratio 1.62, 95% CI 1.18, 2.21) compared with those perceiving low income inequality, respectively. Similarly, high perceived inequality in intergenerational mobility was associated with higher odds of depressive symptoms (odds ratio 1.82, 95% CI 1.49, 2.23) and suicide ideation (odds ratio 1.87, 95% CI 1.35, 2.60). Associations with other covariates, such as low SES and poor health behaviour, were in line with expected patterns. In a sensitivity analysis, similar results were observed using continuous variables (perceived income inequality, intergenerational mobility inequality, quintile objective income and subjective income) (see Supplementary Material 1).
Table 3 Multivariate association between perceived economic inequalities and mental health
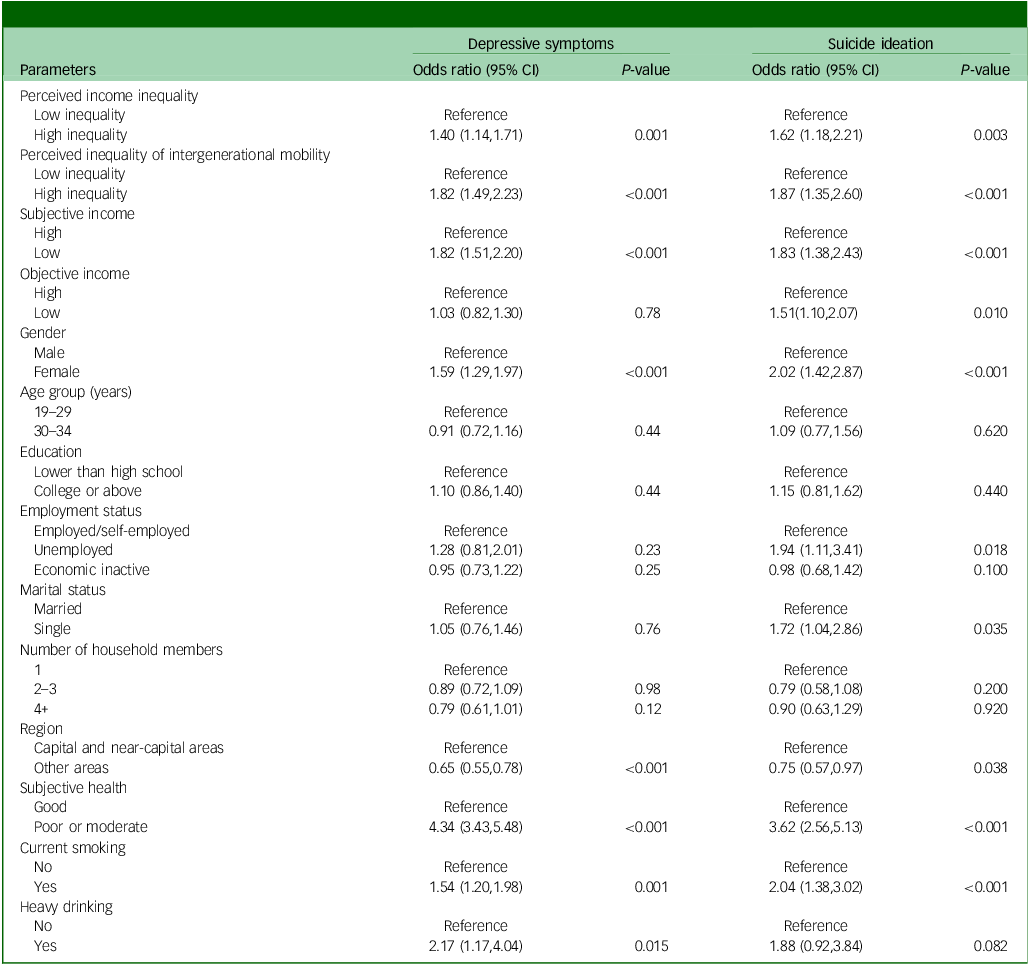
Figure 1 shows the subgroup analysis of multivariate associations between perceived economic inequalities and depressive symptoms/suicide ideation by objective and subjective income. Although no statistical evidence of an interaction between perceived economic inequalities and income was found, associations were consistently observed between high perceived inequalities and depressive symptoms/suicide ideation, particularly among young adults with low objective or subjective income. The strongest associations were observed for those with high perceived intergenerational mobility inequality or low subjective income. For example, the highest odds ratio for depressive symptoms (odds ratio 3.26, 95% CI 2.50, 4.25) and suicide ideation (odds ratio 3.22, 95% CI 2.11, 4.93) was found in young adults with high perceived intergenerational mobility inequality and low subjective income (see Supplementary Material 2).

Fig. 1 Multivariate association between perceived economic inequalities and mental health, by (a) objective and (b) subjective income.
a. Adjusted for subjective income, perceived inequality of intergenerational mobility, gender, age group, employment, marital status, number of household members, region, subjective health, current smoking and high-risk drinking.
b. Adjusted for subjective income, perceived income inequality, gender, age group, employment, marital status, number of household members, region, subjective health, current smoking and high-risk drinking.
c. Adjusted for objective income, perceived inequality of intergenerational mobility, gender, age group, employment, marital status, number of household members, region, subjective health, current smoking and high-risk drinking.
d. Adjusted for objective income, perceived income inequality, gender, age group, employment, marital status, number of household members, region, subjective health, current smoking and high-risk drinking. *P < 0.5.
Discussion
Main findings
Our main findings showed that young adults who had a high perception of economic inequalities were more likely to have depressive symptoms and suicide ideation. Given that there was no statistical evidence of an interaction between perceived economic inequalities and income, individuals with a high perception of inequalities showed more depressive symptoms and suicidal ideation, regardless of income level. Nevertheless, young adults with low income and a high perception of economic inequalities showed the strongest association with depressive symptoms and suicide ideation, particularly when they perceived high inequality in intergenerational mobility and had low subjective income levels.
Interpretations of findings
Our findings showed that high perceived economic inequalities were associated with depressive symptoms and suicide ideation among young adults, even after adjusting for covariates and various SES indicators. This is consistent with previous findings. Reference H-l and Shim12,Reference Zhang, Wang, Zhang, Wei, Jian and Guo13 Economic inequality may influence mental health through psychosocial mechanisms, such as status competition and social distance. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1,Reference Pickett and Wilkinson38 Previous studies reported that perceived economic inequality was associated with lower social cohesion and interconnectedness, proxies for social distance, suggesting that perceived economic inequality increases social distance due to reduced cooperation. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1 Similarly, a previous Korean study found that social trust mediated the association between perceived income inequality and depressive symptoms. Reference Kim11 Additionally, as a proxy for status competition, individuals with a high perception of economic inequalities may have a stronger desire for power and greater sensitivity to threats from others due to heightened concerns about their SES. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1 Thus, young adults, particularly in a competitive social environment, might put in extra effort to increase their competitiveness. Consequently, a high perception of economic inequality may increase status anxiety and lead to poor mental health among adults Reference Zhang, Wang, Zhang, Wei, Jian and Guo13 through heightened social distance and status competition. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1 This indicates a stronger association between the perception of economic inequality and mental health, underscoring the importance of the perception. However, further investigation is needed to better understand the underlying mechanisms for this association.
Our findings showed that there was no interaction effect between the perception of economic inequalities and income level. Similar to a previous study, Reference Du, Huang, Ma, Chen, Chi and King9 individuals with a high perception of economic inequalities tended to have more symptoms of depressive symptoms and suicide ideation, irrespective of their income level, suggesting that the perception of inequalities affects mental health to a greater extent. Nevertheless, our findings indicate that young adults with a high perceived economic inequality and both low objective and subjective income showed the greatest risk of depressive symptoms and suicidal ideation. In particular, the inequality perception of intergenerational mobility was more strongly associated with these outcomes than perceptions of income inequality. Furthermore, those with low subjective income and perceived higher economic inequality were more likely to experience poor mental health than those with low objective income. Many young adults in South Korea started to believe that parental SES determines their children’s SES, an expression known as the spoon class since the mid-2010s. Reference Kang and Park22 After this expression became popular and widespread, young people began comparing themselves with those born with a silver spoon, which indicates wealthy families, and assessing their socioeconomic position. Consequently, some young people may perceive themselves as being born with a ‘dirt spoon’, representing a less socially advantaged background with limited resources and opportunities for upward mobility. Reference Kang and Park22 Exposure to this social climate related to intergenerational mobility inequality can lead to dissatisfaction with what we have and promote individual upward comparisons. This could then deepen perceived economic inequalities and heighten the risk of emotional distress or psychosocial burden if there are limited resources and opportunities for upward mobility. Reference Zhang, Wang, Zhang, Wei, Jian and Guo13,Reference Elenbaas, Rizzo and Killen39 In particular, individuals with lower income status and a high perception of economic inequalities may feel more frustrated than others, because they may recognise that they have very limited chances of improving their situation. Reference Oshio and Urakawa10 Such comparisons could also lead to a lower sense of subjective SES among individuals with low objective income, due to feelings of personal inadequacy Reference McCarthy and Morina40 and a sense of relative unfairness. Reference Smith, Pettigrew, Pippin and Bialosiewicz41 Furthermore, this dissatisfaction and upward comparison may drive young adults to develop a sense of relative deprivation Reference Condon and Wichowsky42 and pessimistic expectations of their future status, which could be linked to poor mental health. Reference Choi, Lee, Sempungu and Lee28 This suggests a stronger link between perceived economic inequality and mental health, highlighting the importance of addressing structural economic inequalities.
Implications
Given that young people have social interactions in their everyday lives, including via media, communications with people and other informal sources, Reference Pickett and Wilkinson2,Reference Oshio and Urakawa10,Reference Gugushvili, Reeves and Jarosz43 these interactions may not only influence individuals’ perception of economic inequality (visible condition) but also shape the social climate surrounding the perception of economic inequality in communities (invisible condition). Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1 Policy needs to interact with young adults through social campaigns and education to reduce the perception of economic inequalities and promote optimistic expectations for their future social mobility. Furthermore, governments and policymakers should consider structural factors to ensure fair access to resources and opportunities for young adults, regardless of parental and individual SES, which can reduce inequality and its negative consequences. Reference Willis, García-Sánchez, Sánchez-Rodríguez, García-Castro and Rodríguez-Bailón1,Reference Browman, Destin, Kearney and Levine19 Specifically, greater socioeconomic and welfare support is needed to alleviate the social burden and pressure among young adults with lower SES, such as expanding support policies and fostering the development of high-quality job opportunities. Reference Kim11 Therefore, it is essential to develop and implement strategies that reduce both perceived and actual economic inequalities to improve mental health among young adults.
Strengths and limitations
This study provides additional evidence on the association of perceived economic inequalities with mental health, using a large, nationally representative sample of South Korean young adults aged 19−34 years. Moreover, we focused on two aspects of perceived inequalities: income inequality and inequality of intergenerational mobility. However, some limitations should be considered when interpreting our findings. First, the data used in this study were cross-sectional, which suggests that we could not infer clear causality between perceived inequalities and depressive symptoms/suicide ideation. Although we assumed that perceived inequalities among young adults might influence their depressive symptoms and suicide ideation, the association could also be bidirectional. This suggests that further investigation is necessary with longitudinal data to better understand the dynamic of this relationship over time. Reference H-l and Shim12,Reference Zhang, Wang, Zhang, Wei, Jian and Guo13 Second, some of the key variables (e.g. perceived inequalities and suicide ideation) used in this study were measured using a single question. Although these single-question measurements were commonly used in previous studies, Reference Kim11,Reference Choi, Ki, Yip, Park, Song and Lee27–Reference Nahrin, Al-Mamun, Kaggwa, Al Mamun and Mamun30 such an approach may provide less detailed information and lead to measurement errors. Reference Fisher, Matthews and Gibbons44 Future studies might consider using a more comprehensive and validated scale, such as the Perceived Economic Inequality Scale (PEIS) Reference Valtorta, Vezzoli, Mari, Durante and Volpato45 or the Beck Scale for Suicide Ideation (BSS). Reference Beck, Kovacs and Weissman46 Third, although dichotomising the continuous variables of interest in our study might pose some limitations, it may also be beneficial for data presentation and the ready interpretation of results. Reference Altman and Royston31 While this dichotomising process may incur some cost, such as loss of information, Reference Altman and Royston31 our sensitivity analysis shows that similar results with statistical evidence were observed using the continuous variables (see Supplementary Material 1). This suggests that our findings using dichotomisation may be less biased. Fourth, although we accounted for a range of covariates in our analysis, we could not include potential interpersonal factors (e.g. personality or self-esteem) or cultural factors (e.g. Confucianism and capitalism). Addressing these factors in future studies could potentially improve the understanding of the underlying mechanisms of the association. Lastly, future qualitative research could enhance our understanding of how perceived inequality impacts mental health challenges in young adults.
Supplementary material
The supplementary material can be found online at https://doi.org/10.1192/bjo.2025.785
Data availability
The data-sets used and/or analysed during the current study are available from MicroData Integrated Service (https://mdis.kostat.go.kr/index.do [in Korean]) provided by Statistics Korea.
Author contributions
M.C. and Y.H.L. designed the study. M.C. and J.K.S. were involved in reviewing the literature, data collection and statistical analyses and drafted the manuscript. M.C., J.K.S. and M.-H.K. interpreted the data. M.C. and J.K.S. contributed to the creation of tables and figures. M.-H.K., E.H.L. and J.H.H. revised the manuscript. All authors approved the final manuscript.
Funding
Y.H.L. was supported by grants from Korea University. M.C. was supported by the National Research Foundation (NRF) of Korea funded by the Ministry of Education (grant no. NRF-2022R1A6A3A01086222). The funding bodies played no role in the design, collection, analyses and interpretation of data.
Declaration of interest
None.
Ethical statement
Ethical approval for this research was obtained from the IRB of Korea University (approval no. KUIRB-2024-0298-01).







 Open access
Open access
eLetters
No eLetters have been published for this article.