



Introduction
Ventricular septation is a surgical technique of biventricular repair for the univentricular heart with a total or almost absent interventricular septum and was introduced at the Mayo Clinic in 1956. Reference McGoon, Kanielson, Ritter, Wallace, Maloney and Marcelletti1 Kawashima and colleagues reported good ventricular function after the septation of a single ventricle with transposition of great arteries. Reference Kawashima, Mori, Matsuda, Miyamoto, Kozuka and Manabe2,Reference Shimazaki, Kawashima, Mori, Matsuda, Kitamura and Yokota3 However, the Fontan procedure has been utilised for single ventricle due to the complexity of ventricular septation, early high mortality, and some complications. Reference Margossian, Solowiejczyk and Bourlon4 Few reports indicate the long-term result of ventricular septation, Reference Shimada, Hoashi and Nakata5 and there is no case report of reoperation for bending and torn spiral Teflon patch 40 years after the septation technique.
Case report
The patient is a 50-year-old man who underwent ventricular septation at the age of 6 years. Reference Kawashima, Mori, Matsuda, Miyamoto, Kozuka and Manabe2 During childhood, examinations confirmed a functional univentricular heart. The aorta arose from the heart just in front of the pulmonary artery. In the inspection of the intraventricular structure through the tricuspid valve, the atrioventricular valves were side by side, and left-sided atrioventricular valve was posterior to the right-sided atrioventricular valve. The right ventricle was found in the anterior and right side of the heart. The ventricular septum was almost absent. Echocardiogram showed that the blood flow velocities measured using the continuous Doppler method of the left ventricular outflow tract was 1.5 m/s and the right ventricular outflow tract was 2.2 m/s, and he was diagnosed with single ventricle, D-malposition of great arteries. Ventricular septation was performed by the spiral patch technique using a Teflon patch (Fig 1). Three years after surgery, the cardiac angiography examination showed that the left ventricular end-diastolic volume was 139 ml/m2. The right ventricular end-diastolic volume index was 93 ml/m2. Although cardiac ejection fraction was around 45 %, the condition of the patient was stable for 40 years without any symptoms of heart failure. However, 40 years after the operation, the patient exhibited shortness of breath. Echocardiogram showed that the amount of ventricular shunt was larger than before. CT revealed that the left ventricular end-diastolic volume index was 213 ml/m2, and right ventricular end-diastolic volume index was 103 ml/m2. The left ventricle was larger than that observed before, and the angiogram showed a large systemic to pulmonary shunt. Cardiac catheterisation showed that a pulmonary to systemic flow ratio (Qp/Qs) was 3.8. CT indicated that the calcified spiral Teflon patch was bent in two, and partially torn, forming a hole that caused a left-to-right shunt (Fig 2).
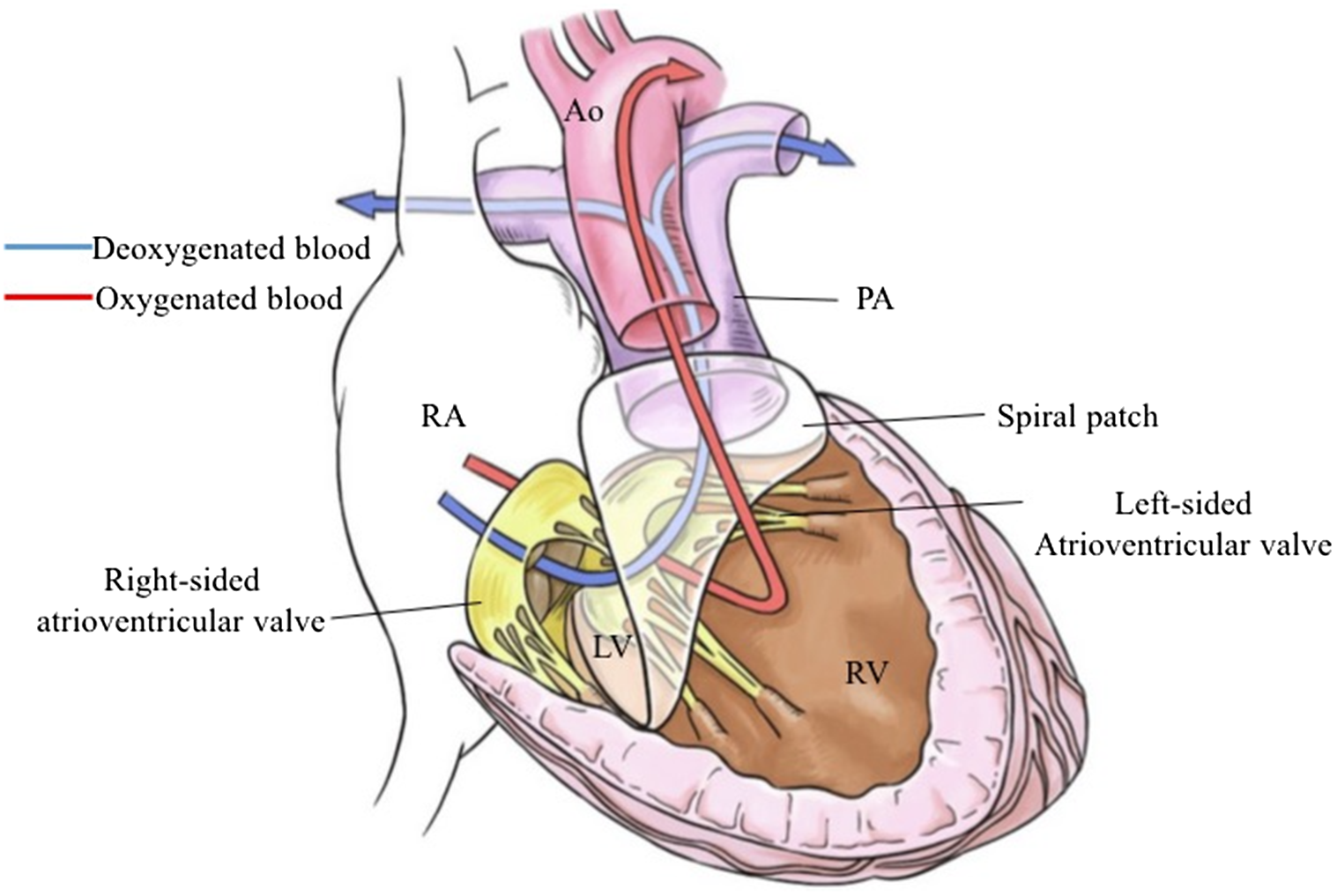
Figure 1. Ventricular septation. A ventricular septum is created using a spiral Teflon patch in childhood, directing the blood flow through the anterior tricuspid valve into the posterior pulmonary artery and through the posterior mitral valve into the anterior aorta. RA, right atrium; LV, left ventricle; RV, right ventricle; Ao, aorta; PA, pulmonary artery.
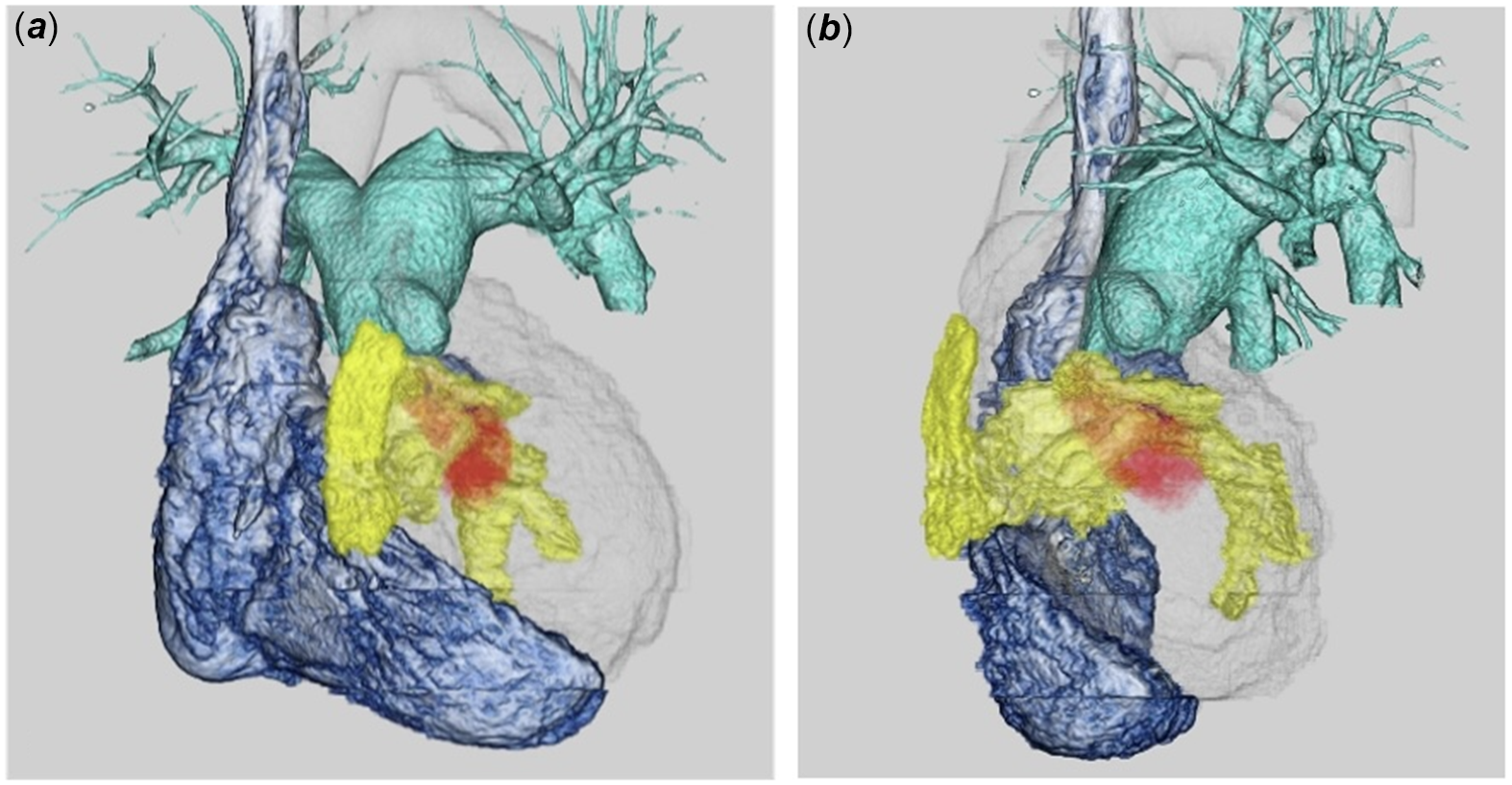
Figure 2. CT findings. (a) Front view. (b) Side view. The blue area shows right atrium and right ventricle. The yellow area is a calcified patch, leading pulmonary valve and artery (green area) which is posterior to the aortic valve and artery. Transparent area shows the left ventricle and ascending aorta which is in front of the pulmonary artery. Red area shows the flow which is through the hole of the calcified patch.
Under cardiopulmonary bypass and cardiac arrest, the right atrium was incised longitudinally. From a precise inspection of the intraventricular structure, a tearing hole of the calcified bending Teflon patch was detected. The chordae of the atrioventricular valve were adhered with the calcified patch. Because the whole patch could not be seen via tricuspid valve, the right ventricle was incised from the base of the pulmonary artery to obtain a clear view. The size of the hole was approximately 2.5 cm and the tearing defect coincided with the bottom of the patch fold. The chordae of the atrioventricular valve were adhered to the calcified septation patch, although it was not discovered during the pre-operative examination. As it was difficult to perform the reconstruction of the entire septation patch because of chordae adhering the patch, we trimmed part of the Teflon patch not to injure the chordae and used a patch of expanded polytetrafluoroethylene with a diameter of 3.5 cm to close the defect. After 1 year, an echocardiogram revealed that the ejection fraction of the left ventricle was 35 % and the right-sided atrioventricular valve function was mildly insufficient, indicating that both were unchanged compared with those before surgery. Echocardiogram after surgery showed that the pressure gradient of the left ventricular outflow tract was 2.5 m/s and the right ventricular outflow tract was 1.1 m/s. On CT, the left ventricular end-diastolic ventricle volume index improved from 213 to 175 ml/m2 and echocardiography indicated no residual left-to-right shunt. The patient is in good condition without any heart failure symptoms.
Discussion
Margossian et al. reported that the cardiac function in long-term follow–ups in the patients after ventricular septation was ambiguous. Reference Margossian, Solowiejczyk and Bourlon4 Additionally, some studies reported the patient with septation for the functional single ventricle after some decade after operation. Reference Chiu, Chen, Lee, Wu and Anderson6–Reference Kurosawa, Arai, Imai and Matsumura8 In this case, the patient underwent reoperation for town patch which is the cause of the pulmonary to systemic shunt 40 years after the ventricular septation.
For the cause of the tearing the patch, we speculated that the patch had been calcified gradually and patch was compressed with cardiac motion leading tearing of the patch. Although Teflon is a soft material first, but it calcifies over time, which is why this rare case occurs.
Chordae of the right-sided atrioventricular valve adhered to the calcified patch. Fortunately, valve function was good before and after surgery; however, adhesion of patch could make the valve function worse. The adhesion of the valve to the patch was first noticed during surgery, but it is entirely possible that the chordae could have been damaged without noticing it. This is a pitfall when this operation is performed.
The cardiac function and balance between right and left ventricle was well preserved for 40 years until the reoperation. This report is never to deny the septation technique itself. Now that the long-term complications of Fontan circulation have been identified, and septation may become an option for biventricular repair in select cases.
Financial support
This report received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Competing interests
None
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional committees (Ethical Review Board Osaka University Hospital).

 Open access
Open access