This journal utilises an Online Peer Review Service (OPRS) for submissions. By clicking "Continue" you will be taken to our partner site https://www.editorialmanager.com/ashe/default.aspx. Please be aware that your Cambridge account is not valid for this OPRS and registration is required. We strongly advise you to read all "Author instructions" in the "Journal information" area prior to submitting.
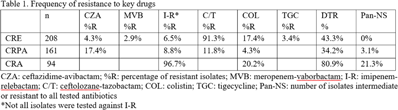
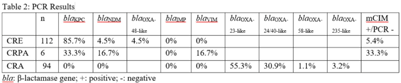
Background: Carbapenem resistance in gram-negative organisms is an important public health problem. The CDC conducted Sentinel surveillance in 2018–2019 to characterize these organisms from 9 facilities in 9 different states. Methods: Carbapenem-resistant Enterobacterales (CRE), Pseudomonas aeruginosa (CRPA), and Acinetobacter spp (CRA) obtained from clinical samples of patients in acute-care or long-term care facilities were submitted to the CDC. Identification was confirmed using matrix-assisted laser desorption ionization time-of-flight (MALDI-TOF), and antimicrobial susceptibility testing (AST) was performed via broth microdilution for 27 antibiotics. All confirmed CRE and CRPA were tested for carbapenemase production (CP) using the modified carbapenem inactivation method (mCIM). The isolates that were mCIM-positive were assessed by real-time PCR for presence of blaKPC, blaNDM, blaVIM, and blaIMP. CP-CRE were also assessed for blaOXA-48-like. All confirmed CRA were tested for the same genes as CRPA and blaOXA-23–like, blaOXA-24/40-like, blaOXA-58–like, and blaOXA-235–like genes. Difficult-to-treat resistance (DTR) was defined as resistance to all β-lactams (excluding newer β-lactam combination agents) and quinolones tested. Results: The CDC confirmed 208 CRE, 161 CRPA, and 94 CRA. Table 1 summarizes AST results for a selection of drugs. We identified 112 (53.8%) mCIM-positive CRE and 6 (3.7%) mCIM-positive CRPA. The PCR results are summarized in Table 2. One mCIM-positive and PCR-negative isolate was positive in a metallo-β-lactamase screen. Conclusions: Resistance among CRE and CRPA to newer β-lactam combination agents was detected. Options for treating CRA are limited. Of 112 CP-CRE, 85.7% harbored blaKPC; CP-CRPA were rare (3.7%); and most CRA harbored blaOXA-23-like (55.3%) or blaOXA-24/40-like (30.9%). Whole-genome sequencing is planned to better understand gene variants, sequence types, and additional resistance markers present among the isolates.
Funding: None
Disclosures: None
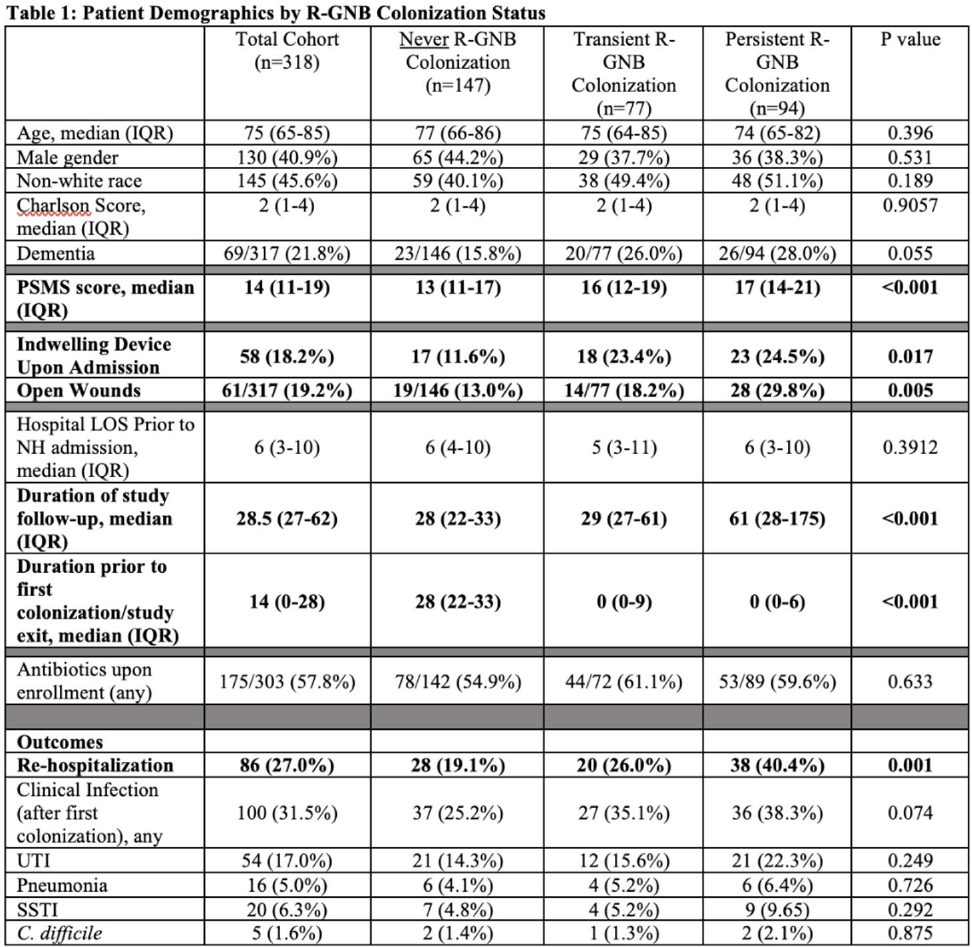
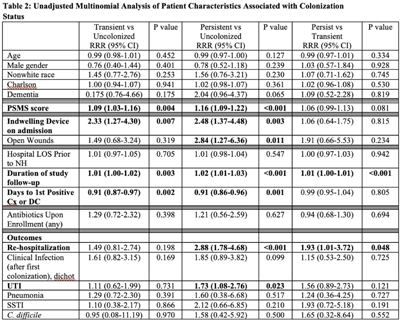
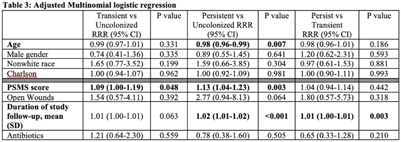
Background: Persistent colonization with resistant gram-negative bacteria (R-GNB) increases risk of clinical infection and intra-facility transmission among nursing home (NH) patients. Limited data exist on the roles of age and function on duration of R-GNB colonization. Methods: Secondary data analysis was performed from a cohort study of patients admitted to 6 Michigan NHs between November 2013 and May 2018. Swabs obtained upon enrollment, day 14, day 30, then monthly until NH discharge from 6 anatomical sites were cultured for GNB. R-GNB were defined as resistant to ciprofloxacin, ceftazidime, or imipenem. Positive R-GNB culture from a single visit followed by negative cultures for the same organism from ≥2 subsequent visits were defined as transient R-GNB colonization. All other patients with positive R-GNB cultures from multiple visits were considered persistently colonized. Demographic data, antibiotic use, device use, and physical self-maintenance scales (PSMSs) were obtained upon enrollment. Characteristics were compared between patients with transient versus persistent R-GNB and uncolonized patients using multinomial logistic regression. Results: We recruited 896 patients (median age, 75 years; 41% male; 46% nonwhite) and followed them for 2,437 total visits. Of 896 patients, 407 (45.4%) were colonized with ≥1 R-GNB during their stay. Of 171 patients with ≥ 2 follow-up visits after R-GNB detection, 94 (55%) remained persistently colonized with the same R-GNB (Table 1). Escherichia coli (30%) and Proteus mirabilis (22%) were the most frequently identified R-GNB. The most common anatomical colonization sites were perirectal (368 [24.3%] of 1,147) groin (340 [14.3%] of 2,046), and hands (115 [4.8%] of 2283). Compared to uncolonized patients, patients with persistent (1.09; 95% CI, 1.00–1.19, P = .048) and transient R-GNB colonization (1.13; 95% CI, 1.04–1.23; P = .003) had lower PSMS (Tables 2 and 3). Compared to uncolonized and transiently colonized patients, patients with persistent R-GNB colonization had prolonged lengths of NH stay (1.01; 95% CI, 1.00–1.01; P = .003). Conclusions: R-GNB colonization in vulnerable NH patients is common (407 [45.5%] of 896 and often persistent (94 [55%] of 171 patients with sufficient follow-up to assess persistence). Patients with persistent R-GNB had lower functional status, longer LOS, and higher readmission rates than those without. R-GNB decolonization should be investigated as a strategy to potentially improve outcomes among NH patients.
Funding: None
Disclosures: None
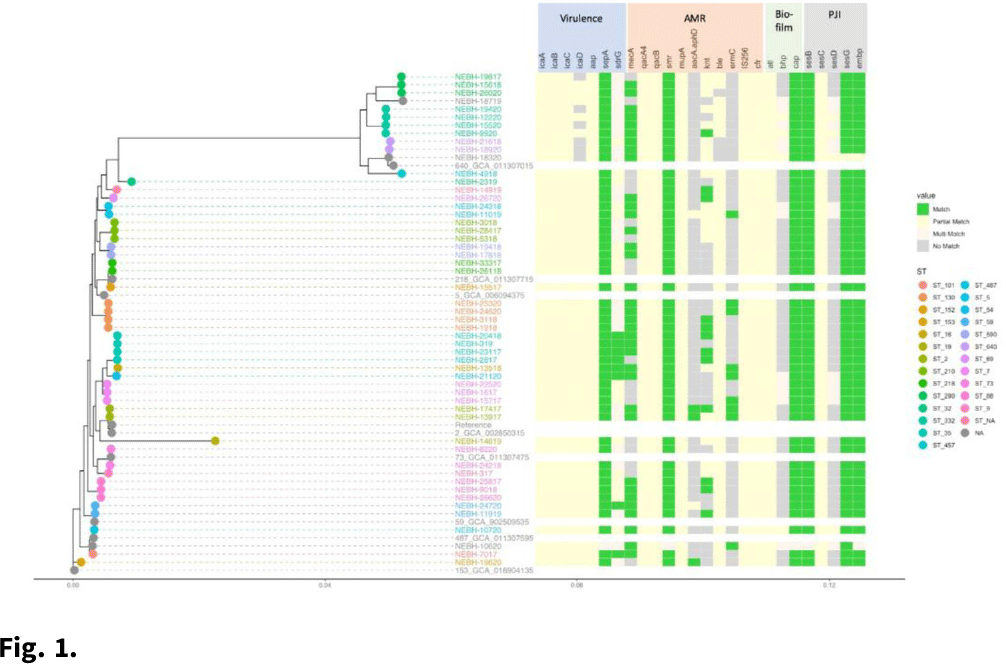
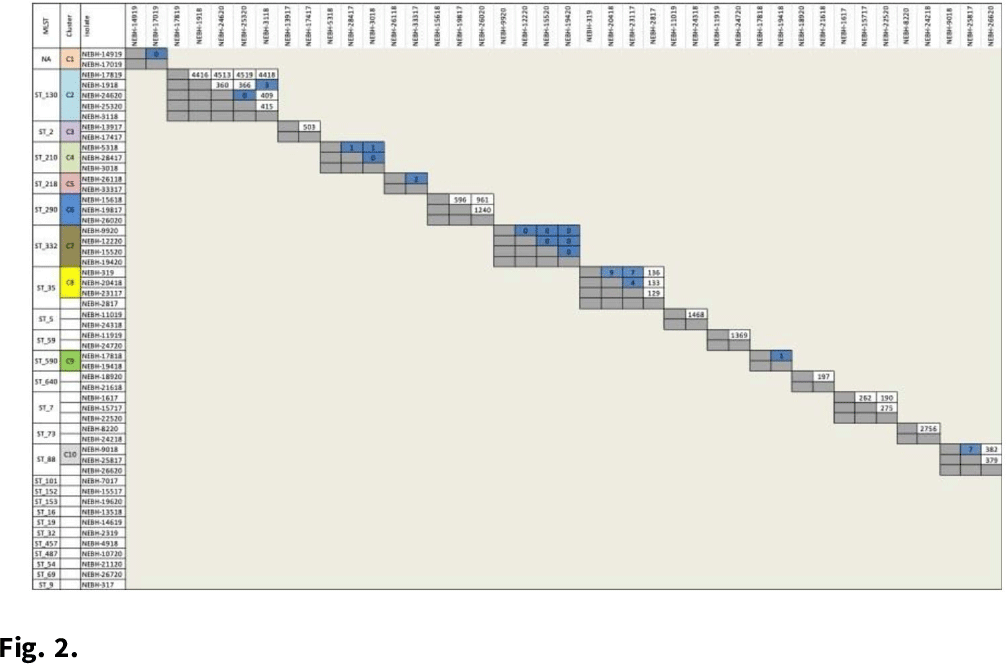
Background: Prosthetic joint infections (PJIs) are costly and cause increased morbidity and mortality for patients. Staphylococcus epidermidis is a common cause of both early postoperative and late-presenting PJIs. Although S. epidermidis is a normal part of the human skin microflora, its ability to form biofilm on implanted medical devices make it an important causative pathogen of PJIs. We investigated genetic, epidemiologic, and environmental factors contributing to S. epidermidis PJIs by performing whole-genome sequencing and clinical epidemiologic investigation of isolates collected from infected patients between 2017 and 2020. Methods: Patients with S. epidermidis isolated from a prosthetic joint that was placed at our orthopedic specialty hospital were identified using the microbiology laboratory records and electronic medical records. Whole-genome sequencing and single-nucleotide polymorphism (SNP)–based clonality analyses were performed using the epiXact service at Day Zero Diagnostics. These analyses included species identification, in silico MLST typing, phylogenomic analysis, as well as genotypic assessment of the prevalence of specific antibiotic resistance genes, virulence genes, and other relevant genes. For clonal isolates, additional reviews of surgical history and clinical data were performed. Results: In total, 62 S. epidermidis joint isolates were identified from 46 patients. Among these isolates, 52 were of sufficient purity to be used for genomic analysis (Fig. 1). A number of genes appeared in every isolate including sepA, smr, cap, sesB, sesG, and embp. Also, 6 S. epidermidis samples had a discrepancy between phenotypic resistance to oxacillin and the presence of the mecA resistance gene. We also identified 6 distinct clusters of isolates, all of which had SNP distances <10 base pairs (Fig. 2). Each cluster consisted of 2–4 patients. Cluster isolates accounted for 29.8% of all S. epidermidis prosthetic joint isolates. Most clonal isolates occurred in patients who were heavily exposed to different healthcare settings. Further epidemiologic investigation showed that some of these clonal isolates had ties to aspirations or procedures, whereas no clear connection could be determined for others. Conclusions: S. epidermidis isolated from clinical prosthetic joint samples contains a high degree of genetic resistance, including a mismatch between presence of mecA and phenotypic oxacillin resistance and genetic propensity for chlorhexidine resistance. Mupirocin resistance was not observed. Of all isolates, 29.8% belonged to multiple clusters, confirming hospital spread of this commensal organism in some cases.
Funding: None
Disclosures: None
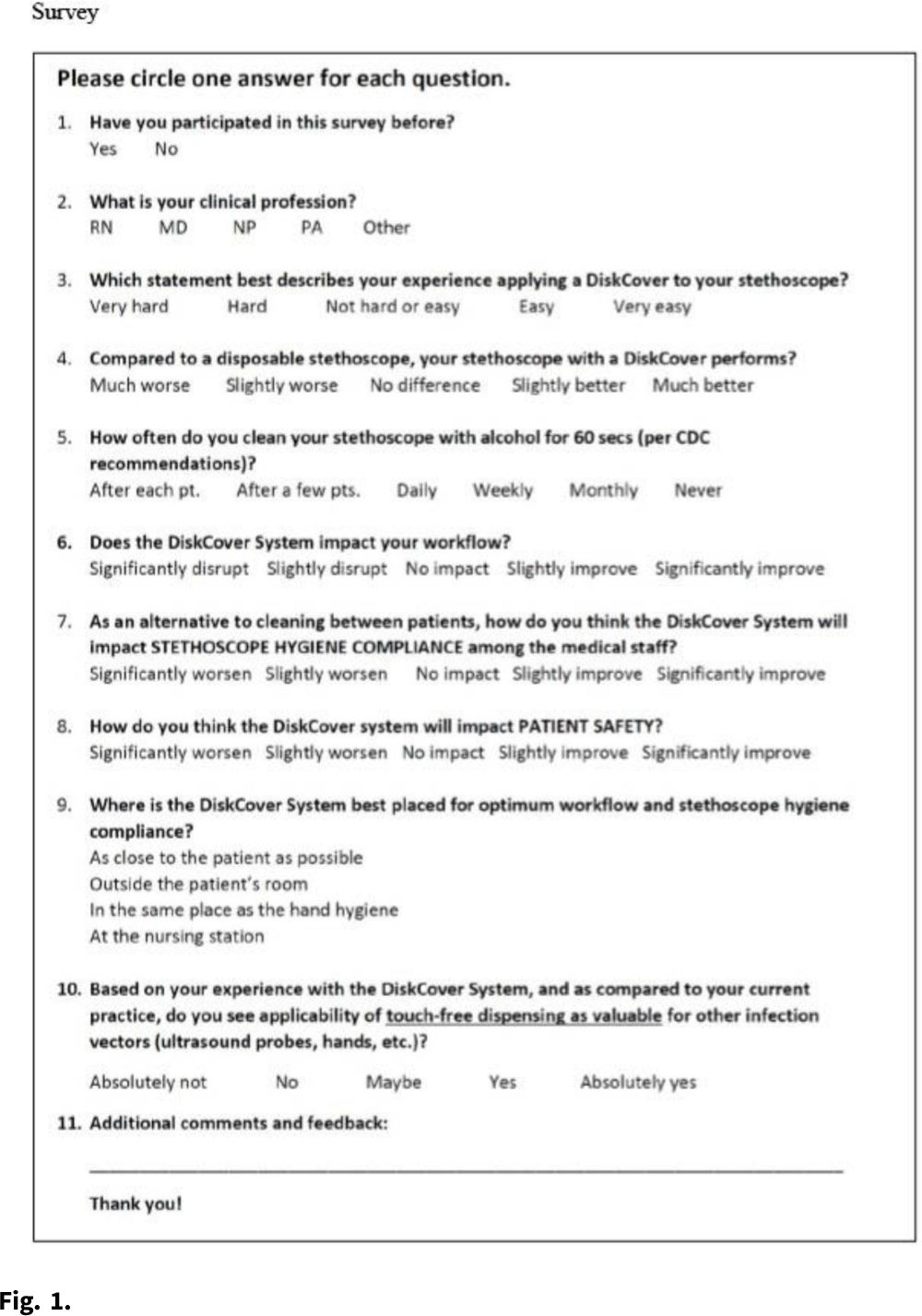
Objective: We evaluated the impressions and perceived workflow consequences following installation of a touch-free aseptic stethoscope barrier dispenser in the clinical environment. Methods: Beginning in 2020, we conducted a volunteer survey of aseptic stethoscope diaphragm barrier (AseptiScope, San Diego, CA) users in multiple departments at 7 US healthcare facilities. A 10-question survey was presented on an iPad near the aseptic barrier dispenser, which was usually located in the patient exam room, to be available immediately after the practitioner completed their examination, which included the use of the stethoscope barrier. This evaluation was considered a quality improvement project and was exempt from institutional review board approval. For this analysis, only 1 survey per practitioner was included. Results: Overall, 147 surveys were obtained from 7 institutions geographically distributed across the United States, immediately after placement of the DiskCover system in the patient care environment. Responses were generally positive and included ease of use (95.2% rated easy or very easy), comparison to a disposable stethoscope (97.9% as similar to, improved over, or significant improvement), workflow changes (53.7% improvement, 97.3% no impact, or improved), and perceived effect on patient safety (90.3% felt that patient safety was improved or significantly improved). Conclusions: The use of a touch-free aseptic stethoscope barrier system was reported to be easy to use, superior to a disposable stethoscope, and an improvement to practitioner workflow and perceived patient safety.
Funding: AseptiScope, Inc.
Disclosures: None
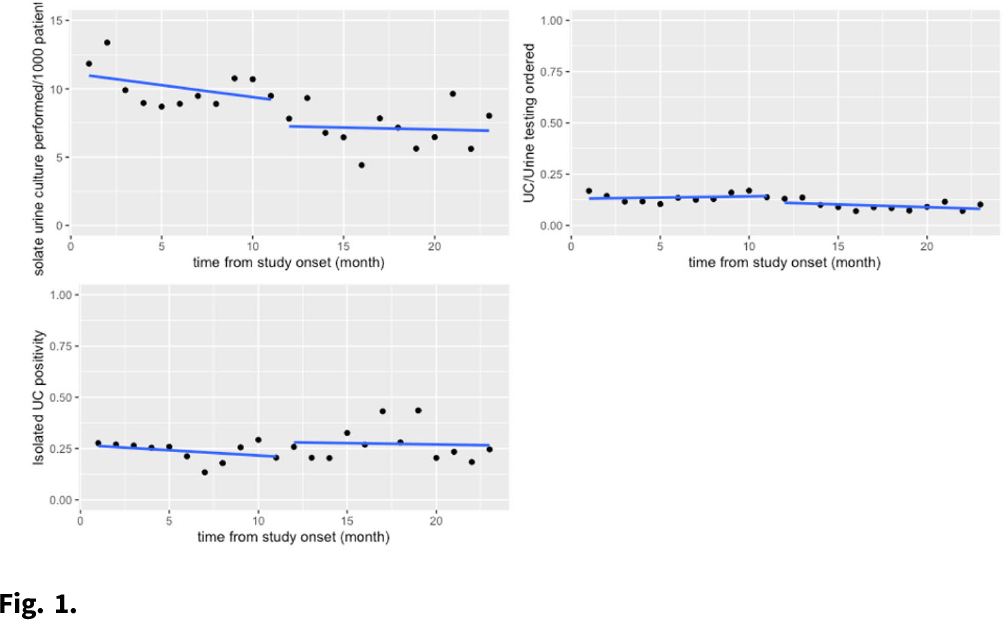
Background: Urine testing is one of the more frequently ordered diagnostic tests among hospitalized patients. Many hospitals have implemented urinalysis with reflex culture (UARC) as a method of diagnostic testing stewardship to guide appropriate use of urine testing. Isolated urine culture, or urine culture without preceding urinalysis, is the most appropriate diagnostic test for patients who are neutropenic, pregnant, or those about to undergo an invasive urologic procedures. This testing is often used beyond these indications in hospitals though, potentially leading to overdiagnosis of UTI and overtreatment of asymptomatic bacteriuria. Methods: We compared outcomes in the preimplementation period (December 2018–November 2019) to those in the postintervention period (December 2019–October 2020) at an academic medical center. The intervention was the addition of an indication selection (ie pregnancy, neutropenia, etc) to the isolated urine-culture order in the electronic medical record (EMR). The primary outcomes were isolated urine culture rate per 1,000 patient days and urine-culture positivity. Our exploratory analysis included a review of selected indications after the intervention was implemented and a chart review of a subset of these tests for appropriateness. The primary analysis was performed using interrupted time-series negative binomial regression. Results: There was no significant change in isolated urine-culture rates after the intervention (11.18 cultures per 1,000 patient days before the intervention versus to 7.75 cultures per 1,000 patient days after the intervention; P > .90), and there were as no significant pre- or postintervention trends. We detected no significant change in isolated urine-culture positivity: 26.9% before the intervention versus 26.7% after the intervention (P > .90). These results are shown graphically in Fig. 1. In the exploratory analysis, of 661 isolated urine-culture tests ordered in the postintervention period, the indication for testing was left blank in 71.9% of tests. The other most common reasons for testing included other (16%), pregnancy (5.7%), and neutropenia (4.4%). In the 100 tests reviewed for appropriateness, only 8% had a documented diagnosis corresponding with the selected indication for testing. Discussion: The addition of an indication selection for isolated urine culture testing did not change the rates of culture ordering or the culture’s subsequent likelihood of positivity. In the exploratory analysis, most providers were incorrectly selecting this testing rather than UARC as prompted. Next steps could potentially be removing the “other” category and requiring a selected answer or requiring approval from stewardship team prior to ordering. Continued education of providers is paramount to the appropriate use of diagnostic testing.
Funding: None
Disclosures: None
Background:Candida bloodstream infections (candidemia) have significant mortality and morbidity rates, as well as healthcare cost implications. Emerging multidrug-resistant Candida spp such as Candida auris, as well as increasing resistance among non–albicans species, which are becoming more prevalent, also raise concern. Understanding the epidemiology of this infection could enhance prevention and management efforts. We studied risk factors for candidemia. Methods: This matched case–control study was conducted at a university hospital from December 2019 through May 2021. Cases of candidemia were identified using positive blood-culture results. Controls were matched 5:1 to cases by age, sex, and month and year of admission. Risk factors of interest included total parenteral nutrition (TPN), central venous access (CVA), neutropenia, Clostridium difficile, pancreatic disease, Candida in urine culture, cancer, invasive procedures, H2 blockers, chemotherapy, antibiotic use, immunosuppression, and antifungal use. Bivariate conditional logistic regression models were used to study the association of individual factors with candidemia. Multivariable conditional logistic regression models were performed using factors with a P Results: Overall, 101 patients with candidemia and 505 matched controls were included. In the bivariate analysis, associations were detected between candidemia and TPN, CVA, pancreatic disease, invasive procedures, H2 blocker use, antibiotic use, and antifungal use (all Ps Conclusions: Associations of candidemia with recent antifungal use and pancreatic disease were relatively novel findings. Neutropenia was not an independent risk factor for candidemia in this study. Future directions include further evaluations of previous antifungal use in patients with candidemia to identify opportunities for possible intervention and antifungal stewardship.
Funding: None
Disclosures: None

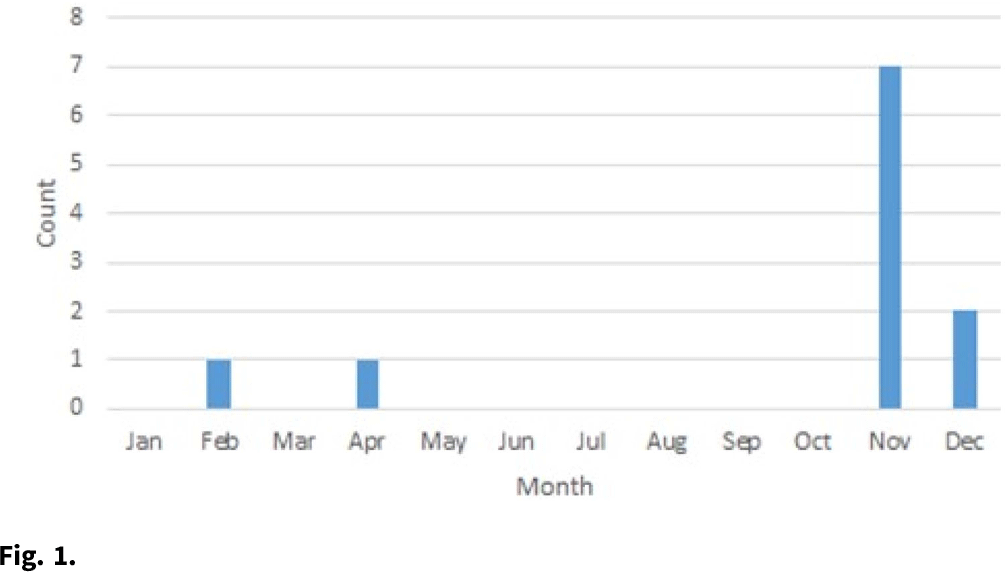
Background:Cutibacterium acnes is normal skin flora as well as a common culture contaminant. It can cause infections in the setting of sterile implants, although clinical presentations can be subtle. Differentiating true infection from sample contamination is challenging and has implications for patient care. We describe an investigation of a cluster of 7 hospitalized pediatric patients with C. acnes isolated from anaerobic cultures of cerebrospinal fluid (CSF) over 3 weeks at a quaternary-care children’s hospital. Methods: An outbreak response was coordinated between the infection prevention and control (IPC), microbiology, and neurosurgery teams. We defined a case as a hospitalized patient with C. acnes isolated from a CSF culture beginning in November 2020. We reviewed charts of all cases and CSF culture collection on all case units, transport to and processing at the microbiology laboratory, and the IPC team measured adherence for all processes. Results: There were 8 positive cultures in 7 cases from November 10 to 27, 2020. The median case age was 2 months (range, 0–119). Cases occurred on 4 different units. All positive patients had at least 1 implanted neurosurgical device used for CSF drainage. There were no clear commonalities in surgeon responsible for device placement, hardware type placed, or staff collecting CSF samples. A standard protocol for CSF collection was followed for all cases. Overall, 3 patients cleared cultures without intervention, 2 received oral antibiotics, and 2 underwent surgical removal of their device. Specimen processing was unchanged, although due to supply issues, an alternative anaerobic culture media (Anaerobic Systems, Morgan Hills, CA) was used for 6 weeks, during which all cases were identified. Compared to routine media, the alternative is known to enhance organism detection. The company reported no concerns for media contamination or C. acnes outbreaks. Once routine media became available, CSF culture positivity for C. acnes returned to baseline (late November or early December) (Fig. 1). Conclusions: We identified a likely pseudo-outbreak related to temporary use of a more sensitive culture media. No direct patient harm was identified, although many had increased risk of harm by surgical intervention or prolonged length of stay. Technological advances may enhance organism identification but challenge existing paradigms of care. More studies are needed to better delineate the intersection of diagnostic advancements with patient care standards.
Funding: None
Disclosures: None
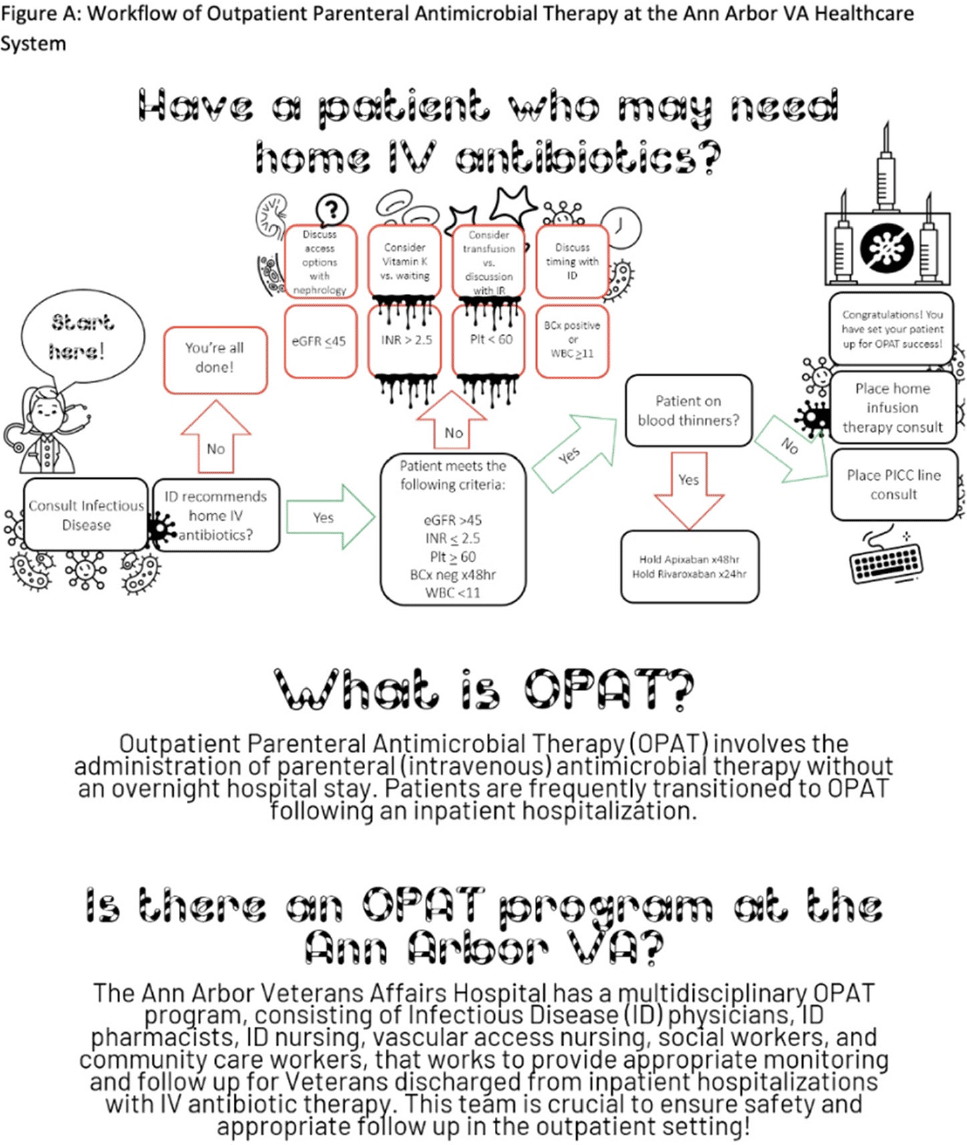
Background: Outpatient parenteral antimicrobial therapy (OPAT) involves the administration of intravenous antimicrobial therapy outside the hospital. The literature suggests that inpatient providers are often unaware of OPAT programs and may not engage this multidisciplinary group in a timely fashion, leading to potentially inappropriate OPAT use. However, few studies have directly addressed this issue. We characterized current practices for coordinating OPAT and assessed provider understanding of OPAT services. We also conducted an exploratory analysis of placement of a peripherally inserted central catheter (PICC) consultation prior to an infectious disease (ID) consultation as a proxy for potentially avoidable OPAT use. Methods: This study was conducted between September and December 2021 at the Ann Arbor VA Healthcare System. All charts (n = 212) in which a consultation for a PICC was placed between January and September 2021 were reviewed, including free-text data entered by patient teams and inpatient progress notes in the days leading up to and following PICC consultation. Additionally, inpatient providers were surveyed using an online format regarding knowledge, utilization, and perceptions of OPAT. Results: Of the 212 charts reviewed, 108 patient encounters resulted in PICC placement; 80 (74.1%) were placed for the indication of home IV antibiotics. Of these, 3 (4.0%) had the PICC consult placed prior to the ID consultation. Of the 104 PICC consultations that were cancelled, 9 (8.7%) were cancelled because the ID staff did not recommend home IV antibiotics. Other reasons for cancellation included alternative device placement, duplicate order, referral to interventional radiology, failure to meet criteria, or unsuccessful placement. Of the 285 inpatient providers sent the electronic survey, 121 (46.9%) completed at least some portion. Overall, 17 respondents (14.0%) were familiar with the acronym OPAT; however, only 10 were able to expand the acronym correctly. Of the 118 respondents asked about their familiarity with the OPAT program at the local institution, 98 (83.1%) were not familiar at all or were only slightly familiar with the program. In contrast, 7 respondents (6.0%) were very or extremely familiar with the OPAT program. Conclusions: Further education and structural interventions are necessary to improve inpatient providers’ awareness and early engagement of local OPAT programs to ensure appropriate OPAT use. An educational intervention with an informative flowchart diagramming the steps for engaging the OPAT team could raise awareness and improve engagement when potential OPAT needs are identified (Fig. 1).
Funding: None
Disclosures: None
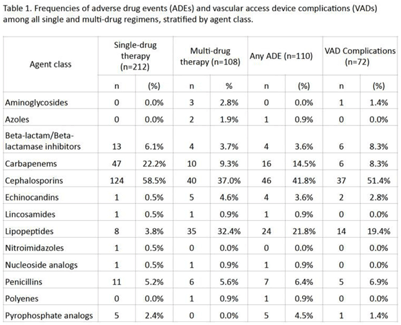
Background: Although many infectious conditions can be safely treated with oral antimicrobials, select circumstances require parenteral antimicrobial therapy. Benefits of OPAT include prevention of hospital-associated conditions and significant cost savings. However, risks of OPAT include adverse drug events (ADEs) and vascular access device (VAD) complications. We analyzed the safety of OPAT regimens as part of implementing a collaborative OPAT program. Methods: We reviewed adult patients discharged home from an academic hospital between January 2019 and June 2021. Patients with cystic fibrosis were excluded. Data on OPAT agents, ADEs, and VAD complications were collected from electronic medical records by 2 reviewers using a standardized REDCap instrument. The institutional review board approved this study. Results: The cohort comprised 265 unique patients; 212 (80%) received single-drug therapy and 53 (20%) received multidrug therapy. In total, 81 patients (31%), who received a total of 110 antimicrobials, experienced an ADE. In total, 55 patients (21%), who received a total of 72 antimicrobials, experienced a VAD complication. Patients who received >1 antimicrobial were more likely to experience an ADE (53% vs 25%; P = .0002) or a VAD complication (32% vs 18%; P = .04). Cephalosporins were the most frequently prescribed antimicrobial class (Table 1). Conclusions: ADEs and VAD complications were frequent in patients on OPAT. Local data should inform (1) the selection of OPAT therapy and (2) the standardized monitoring of patients who receive OPAT going forward in the implementation of this collaborative OPAT program.
Funding: None
Disclosures: None
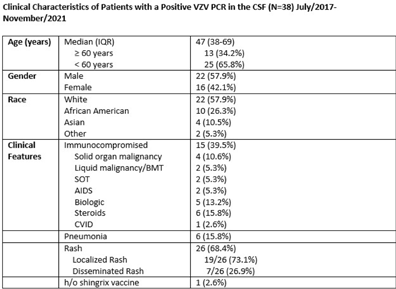
Background: Transmission-based precautions against varicella-zoster virus (VZV) in healthcare settings are determined by the extent of rash (localized vs disseminated) and the immune status of the host. At our facility, immunocompetent patients with localized disease are placed in standard precautions whereas patients with disseminated disease and/or immunocompromised status are placed in airborne and contact isolation. The use of molecular diagnostics has increased recently, and patients can have a PCR positive for VZV in cerebral spinal fluid (CSF) without evidence of pneumonia or disseminated rash. These patients are classified as disseminated disease, but it is unlikely that they are spreading VZV via respiratory aerosols in the absence of other symptoms. Infection prevention guidance is limited in this situation, and these patients may be in unneeded isolation, with the potential for adverse patient effects and overutilizing PPE resources. We have described the clinical characteristics of patients with a PCR positive for VZV in CSF, and we evaluated the risk for transmitting VZV via airborne aerosols. Methods: A retrospective, single-center chart review was performed on all patients admitted with a PCR positive for VZV in CSF between July 2017 and November 2021. Chart review was performed to gather data regarding clinical presentation, patient characteristics, and risk factors. Results: In total, 38 patients were identified who had a PCR positive for VZV in CSF; 22 (57.9%) were male and 16 (42.1%) were female. The median age was 47 years (IQR, 38–69). Also, 15 patients (39.5%) were immunocompromised. Moreover, 26 patients (68.4%) had a rash; 19 (50%) had localized rash; and 7 (18.4%) had disseminated rash involving ≥3 dermatomes. However, 12 patients (31.5%) had neither rash nor pneumonia. Furthermore, 5 patients (13.1%) had PCR positive for VZV in CSF and developed rash within the following 2–7 days (2 with disseminated rash). In addition, 6 patients (15.8%) had pneumonia. Of the 6 patients with pneumonia, 4 (10.5%) were immunocompromised and 3 (7.9%) were above 65-year-old. 32 patients (84.2%) were kept in airborne and contact precautions. 1 (2.6%) patient had a documented record of at least 1 dose of Shingrix vaccine. Conclusions: Most patients with a PCR test positive for VZV in the CSF were not immunocompromised and did not have evidence of disseminated rash or pneumonia. The risk of airborne transmission of VZV via small aerosols appears to be low in patients with a PCR test positive for VZV in the CSF without evidence of disseminated rash or pneumonia. Airborne isolation may not be required for many of these patients.
Funding: None
Disclosures: None
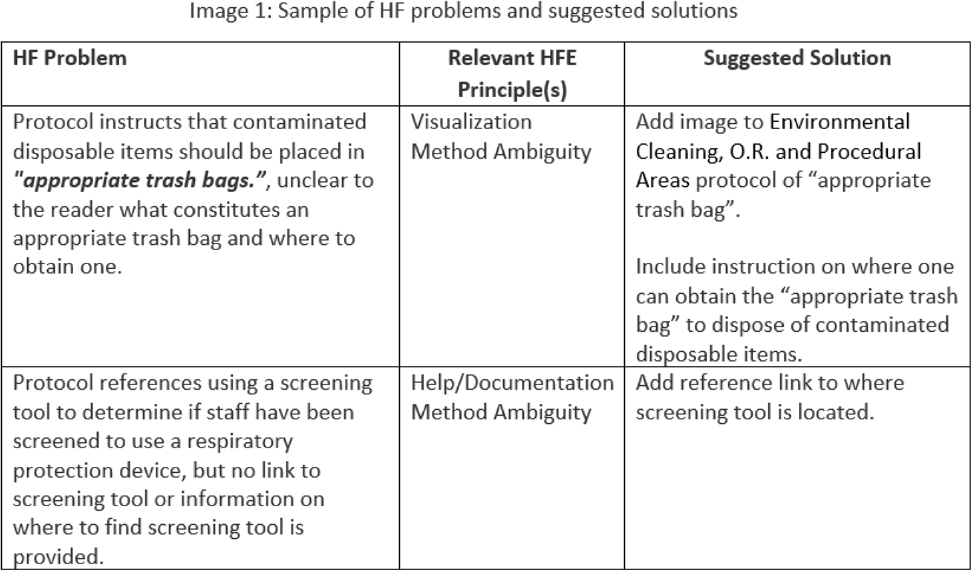
Background: Infection prevention and control (IPC) protocols and guidelines are important quality management tools for educating care professionals and standardizing care processes. However, most of the actual care (ie, work as done) differ from protocol recommendations (ie, work as imagined). No tool or set of criteria has been established for how to develop human-centered IPC protocols. The goal of this research was to develop a standardized human-factors analysis method to provide healthcare organizations with a tangible framework to improve protocol usefulness and usability. Methods: The proposed analysis method combines principles from human-factors engineering (ie, usability heuristics, systems ambiguity framework) and instructional design. Relevant literature was analyzed by experts in human factors and clinical experts to develop a tool with criteria such as visualization and method ambiguity. Overall, 5 IPC-related protocols from a large academic hospital were selected from an electronic database and were evaluated using the proposed criteria. Results: During application of the analysis method, 70 human-factors–related problems were identified across 5 IPC protocols (eg, heater cooler cleaning), including violation of design heuristics and the presence of ambiguity. Frequently violated human-factors design principles included appearance and/or visibility (ie, visual display of content), visualization (ie, providing illustrative examples), and method ambiguity (ie, lack of clarity on how to complete a task). Figure 1 provides a sample of the human-factors problems identified and suggested solutions. Only minor modifications (ie, clarification of criteria definitions) were needed on the final tool. Conclusions: The human-factors–based tool developed in this study can be used both to develop new IPC protocols and to evaluate and improve existing protocols.
Funding: The CDC funded this work. This material is based upon work supported by the Naval Sea Systems Command under Contract No. N00024-13-D-6400, Task Order NH076. Any opinions, findings and conclusions or recommendations expressed in this material are those of the author(s) and do not necessarily reflect the views of the Naval Sea Systems Command (NAVSEA) or the US CDC.
Disclosures: None
Background: Respiratory viral infections are very common among children. Transmission-based precautions are frequently used with patients who test positive for a respiratory virus in pediatric hospitals to prevent transmission of infections, regardless of whether the patient has symptoms of a respiratory infection or not (asymptomatic). However, few data are available on the prevalence of respiratory viral infections in symptomatic and asymptomatic children who are admitted to a pediatric hospital. The study was conducted in 3 hospitals that combine for a 601-bed pediatric healthcare system in northern Texas. Methods: From July 7, 2020, to the present, all patients admitted to the hospital had a nasopharyngeal swab collected and tested with a multiplex PCR panel including SARS-CoV-2 and 8 other common respiratory viruses. Over a 1-year period from October 1, 2020, to September 30, 2021, the prevalences of infection with each of the 9 respiratory viruses were calculated and stratified by respiratory infection symptom status (determined by the ordering provider in an electronic order set) and age group. Results: During this 1-year period, 28,421 PCR panels were collected on patients admitted to the hospital. The median age was 5 years (IQR, 1–12 years), and 15,105 patients were male (53.2%). Overall, 12,792 panels were positive for at least 1 virus (45.0%). Among 26,688 panels on individuals with known symptom status, 26.3% of asymptomatic patients and 69.4% of symptomatic patients tested positive for at least 1 virus. The most common virus was rhinovirus or enterovirus (17.7% asymptomatic positive and 40.2% symptomatic positive) (Fig. 1). Asymptomatic rhinovirus or enterovirus prevalence varied by age group and was greatest in children aged 1–4 years (31.7%) and those aged 5–9 years (23.1%). It was lowest in adolescents aged 15–21 years (7.1%) (Fig. 2). Over time, the prevalence of asymptomatic infections fluctuated with local outbreaks. For SARS-CoV-2, in the resolution phase of an outbreak the prevalence of asymptomatic infections tended to overlap or surpass symptomatic infections. Conclusions: Asymptomatic respiratory viral infections, and in particular rhinovirus or enterovirus infections, were common among pediatric patients admitted to the hospital during the COVID-19 pandemic and were most common among children aged 1–9 years. However, symptomatic patients were still more likely to test positive for a respiratory virus compared to asymptomatic patients. Prolonged shedding of SARS-CoV-2 may explain why asymptomatic prevalence surpasses symptomatic prevalence in the resolution phase after outbreaks.
Funding: None
Disclosures: None


