We use cookies to distinguish you from other users and to provide you with a better experience on our websites. Close this message to accept cookies or find out how to manage your cookie settings.
To save this undefined to your undefined account, please select one or more formats and confirm that you agree to abide by our usage policies. If this is the first time you used this feature, you will be asked to authorise Cambridge Core to connect with your undefined account.
Find out more about saving content to .
To send this article to your Kindle, first ensure no-reply@cambridge.org is added to your Approved Personal Document E-mail List under your Personal Document Settings on the Manage Your Content and Devices page of your Amazon account. Then enter the ‘name’ part of your Kindle email address below. Find out more about sending to your Kindle.
Find out more about saving to your Kindle.
Note you can select to save to either the @free.kindle.com or @kindle.com variations. ‘@free.kindle.com’ emails are free but can only be saved to your device when it is connected to wi-fi. ‘@kindle.com’ emails can be delivered even when you are not connected to wi-fi, but note that service fees apply.
The Spring Conference 2021 focused on the theme of the gut microbiome and health that was divided across three separate but inter-related areas from the impact of nutrition on the gut microbiome, the cause and effect of nutrition and health on the gut microbiome to the interaction between pathogens and gut microbiota. The programme was supported by two plenary lectures, the first discussed the computational methods commonly employed to examine gut microbiota and the concluding lecture presented the interaction between the gut microbiome, nutrition and health in older populations. This short report provides a summary and highlights of the conference.
Symposium 1: The impact of nutrition on the gut microbiome
The aim of this review is to provide an overview of the complex interactions between dietary fibre and the resident microbial community in the human gut. The microbiota influences both health maintenance and disease development. In the large intestine, the microbiota plays a crucial role in the degradation of dietary carbohydrates that remain undigested in the upper gut (non-digestible carbohydrates or fibre). Dietary fibre contains a variety of different types of carbohydrates, and its breakdown is facilitated by many different microbial enzymes. Some microbes, termed generalists, are able to degrade a range of different carbohydrates, whereas others are more specialised. Furthermore, the physicochemical characteristics of dietary fibre, such as whether it enters the gut in soluble or insoluble form, also likely influence which microbes can degrade it. A complex nutritional network therefore exists comprising primary degraders able to attack complex fibre and cross feeders that benefit from fibre breakdown intermediates or fermentation products. This leads predominately to the generation of the short-chain fatty acids (SCFA) acetate, propionate and butyrate, which exert various effects on host physiology, including the supply of energy, influencing glucose and lipid metabolism and anti-carcinogenic and anti-inflammatory actions. In order to effectively modulate the gut microbiota through diet, there is a need to better understand the complex competitive and cooperative interactions between gut microbes in dietary fibre breakdown, as well as how gut environmental factors and the physicochemical state of fibre originating from different types of diets influence microbial metabolism and ecology in the gut.
Symposium 2: Gut microbiome, nutrition and health: cause and effect
Research characterising the gut microbiota in different populations and diseases has mushroomed since the advent of next-generation sequencing techniques. However, there has been less emphasis on the impact of dietary fibres and other dietary components that influence gut microbial metabolic activities. Dietary fibres are the main energy source for gut bacteria. However, fibres differ in their physicochemical properties, their effects on the gut and their fermentation characteristics. The diversity of carbohydrates and associated molecules in fibre-rich foods can have a major influence on microbiota composition and production of bioactive molecules, for example SCFAs and phenolic acids. Several of these microbial metabolites may influence the functions of body systems including the gut, liver, adipose tissues and brain. Dietary fibre intake recommendations have recently been increased (to 30 g daily) in response to growing obesity and other health concerns. Increasing intakes of specific fibre and plant food sources may differentially influence the bacteria and their metabolism. However, in vitro studies show great individual variability in the response of the gut microbiota to different fibres and fibre combinations, making it difficult to predict which foods or food components will have the greatest impact on levels of bioactive molecules produced in the colon of individuals. Greater understanding of individual responses to manipulation of the diet, in relation to microbiome composition and production of metabolites with proven beneficial impact on body systems, would allow the personalised approach needed to best promote good health.
The aetiology of inflammatory bowel disease (IBD) is multifactorial, with diet and gut microbiota playing an important role. Nonetheless, there are very few studies, particularly clinical research, which have explored the interaction between diet and gut microbiota. In the current review, we summarise the evidence from clinical trials exploring the interactions between the gut microbiota and diet in the management of IBD. Data from the effect of exclusive enteral nutrition (EEN) on the gut microbiota of children with active Crohn's disease (CD), receiving induction treatment, offer opportunities to understand the role of gut microbiota in underlying disease pathogenesis and develop novel dietary and pharmacological microbial therapeutics. In contrast, the evidence which links the effectiveness of food-based dietary therapies for IBD with mechanisms involving the gut microbiota is far less convincing. The microbial signals arising from these dietary therapies are inconsistent and vary compared to the effects of effective treatment with EEN in CD.
Symposium 3: Pathogens × gut microbiota interactions
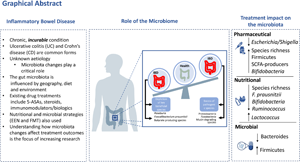
Inflammatory bowel disease (IBD) is a group of immune-mediated disorders characterised by a chronic, relapsing-remitting inflammation predominantly affecting the gastrointestinal tract. IBD is incurable, affecting people in their most productive years. IBD is historically seen as a disease of Westernised nations although in recent times other countries have seen an exponential rise in cases. Although the exact pathogenesis remains unclear, evidence suggests that microbiota changes play a critical role in IBD pathogenesis. Over the past two decades, IBD has become one of the most studied human conditions linked to the gut microbiota. However, deciphering the intricate link between the gut microbiota and therapeutic efficacy remains elusive. This review will summarise the current evidence relating to the gut microbiota and its involvement in IBD pathogenesis as well as the impact of IBD treatments including pharmaceutical-, nutraceutical- and microbial-focused regimens on the gut microbiota.
Conference on ‘Micronutrient malnutrition across the life course, sarcopenia and frailty’
Gene–nutrient interactions (GeNuIne) collaboration, a large-scale collaborative project, has been initiated to investigate the impact of gene–nutrient interactions on cardiometabolic diseases using population-based studies from ethnically diverse populations. In this project, the relationship between deficiencies of vitamins B12 and D, and metabolic diseases was explored using a nutrigenetic approach. A genetic risk score (GRS) analysis was used to examine the combined effect of several genetic variations that have been shown to be associated with metabolic diseases and vitamin B12 and D deficiencies, respectively. In Sri Lankan, Indonesian and Brazilian populations, those carrying a high B12-GRS had an increased risk of metabolic diseases under the influence of dietary protein, fibre and carbohydrate intakes, respectively; however, in Asian Indians, genetically instrumented metabolic disease risk showed a significant association with low vitamin B12 status. With regards to nutrigenetic studies on vitamin D status, although high metabolic-GRS showed an interaction with dietary carbohydrate intake on vitamin D status, the study in Indonesian women demonstrated a vitamin D GRS–carbohydrate interaction on body fat percentage. In summary, these nutrigenetic studies from multiple ethnic groups have provided evidence for the influence of the dietary factors on the relationship between vitamin B12/D deficiency and metabolic outcomes. Furthermore, these studies highlight the existence of genetic heterogeneity in gene–diet interactions across ethnically diverse populations, which further implicates the significance of personalised dietary approaches for the prevention of these micronutrient deficiencies and metabolic diseases.