Neurofeedback regimes in the treatment of adult ADHD are commonly EEG-based and have several shortcomings, including a weak signal-to-noise ratio, low transfer rates from laboratory to everyday environments and ambiguous evidence in respect to adequate brain signals of interest.
To investigate, if an eyetracking-based real-time feedback in a virtual environment can enhance attentional performance, as measured by behavioral, EEG and eyetracking parameters.
Overall, n=18 adult patients with ADHD and n=18 healthy controls (HC) performed a continuous performance task (CPT) in a virtual seminar room, while distracting virtual events occurred. In case the participant’s gaze drifted away from the task an automated audiovisual feedback indicated the participant to refocus on the task. Three 20-minutes blocks were presented in counter-balanced order, that differed in respect to whether real feedback, sham feedback or no feedback was additionally provided.
Mixed ANOVAs with within-subject factors ‘Condition’ (real feedback, sham feedback, no feedback) and ‘Phase’ (distractor phases vs. non-distractor phases) and a between-factor ‘Group’ (ADHD patients vs. HC) revealed better task performances in HC than ADHD patients in respect to omission errors (p = .023), mean reaction times (p = .042) and reaction time variabilities (p = .007; cf. Figure 1). Moreover, omission errors turned to be higher during distractor-present than distractor-absent trials (p = .007), especially in ADHD.
Figure 1.
CPT results. DP=distractor-phases, NDP=non-distractor-phases
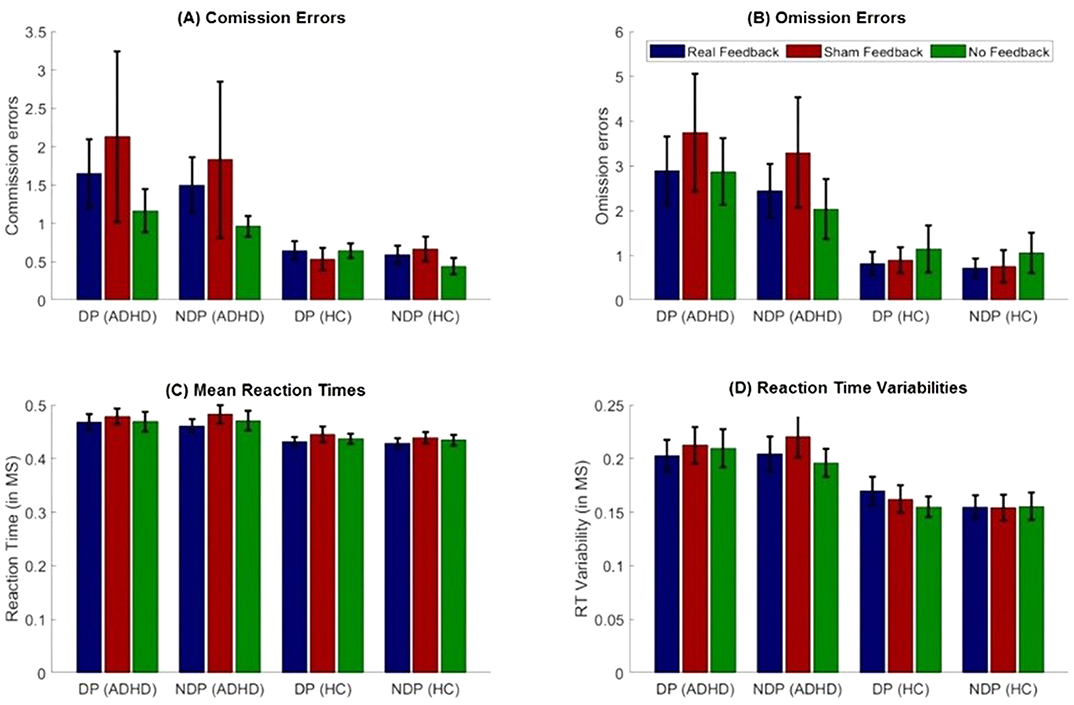
While the virtual CPT turns out to discriminate well between patients with ADHD and HC, the behavioral results do not indicate an attentional performance enhancement based on the gaze-dependent feedback.
No significant relationships.
Attention-deficit/hyperactivity disorder (ADHD) is a psychiatric condition in which children suffer from inattentiveness, hyperactivity, and or impulsivity. ADHD patients frequently present comorbid psychiatric disorders: in adults, the most common are depression, substance-related disorders, anxiety, and eating disorders. Children and adolescents present conduct disorders, learning disorders, anxiety and depression. Since ADHD and its psychiatric comorbidities share similarities, a partial overlap of their pathophysiological mechanisms has been suggested. ADHD, can be treated with lisdexamfetamine (LDX), a prodrug indicated by the FDA as treatment for binge eating disorder (BED) and ADHD.
To evaluate, through a systems biology-based in silico method, the efficacy of LDX as first-line ADHD treatment to improve ADHD psychiatric comorbidities. Furthermore, we explored the molecular mechanisms behind LDX’s action.
We used the systems biology- and artificial intelligence-based Therapeutic Performance Mapping System (TPMS) technology to characterise and model ADHD comorbidities. Artificial neural networks (ANNs) algorithms were used to identify specific relationships between protein sets. Finally, we modelled the mechanisms of LDX for the most relevant comorbidities by using sampling methods and comorbidity-specific virtual patients in each case.
This study predicts a strong relationship between LDX’s targets and proteins involved in BED and depression (Fig 1). Our results could be explained not only by LDX role in neurotransmitter regulation, but also by modulation of neuroplasticity (BDNF/NTRK2, GSK3), neuroinflammation (interleukins, inflammasome), oxidative stress (NOS2, SOD), and the hypothalamic-pituitary-adrenal (HPA) axis (CRH, CRHR1).
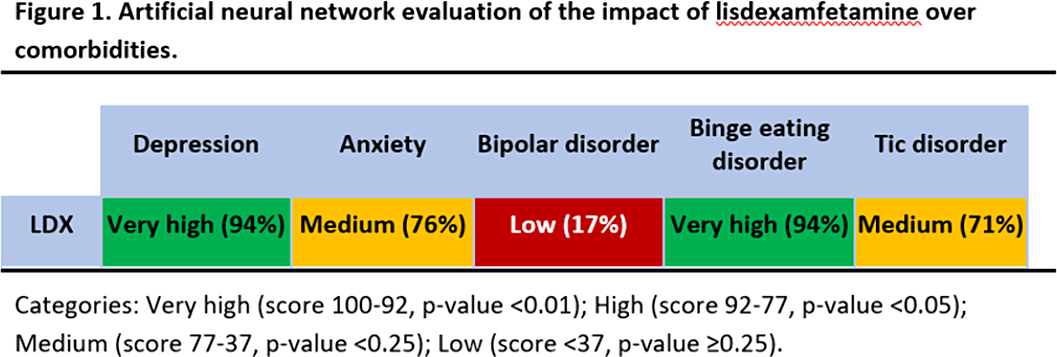
These findings could be used in pre-clinical and clinical future investigations to assess optimal treatment for ADHD patients with psychiatric comorbidities.
JRGC: speaker for Takeda and Shire, research funding from Shire and Lumbeck, collaborations with Laboratoires Servier JQ: speaker or scientific advisor for Takeda, Janssen, Rubio. Investigation funding: Instituto de Salud Carlos III. PR, CM, TPR: full-ti

