
189 results
ELders AT Ease (ELATE): a description of adapting cognitive behaviour therapy for treating mental health issues in nursing homes
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 18 / 2025
- Published online by Cambridge University Press:
- 24 January 2025, e4
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
CBT-E following discontinued FBT for adolescents with eating disorders: time for a more individual approach?
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 18 / 2025
- Published online by Cambridge University Press:
- 03 January 2025, e1
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Exploring the perceptions of people diagnosed with schizophrenia and their family members to inform the cultural adaptation of cognitive behavioural therapy for psychosis in Saudi Arabia: a qualitative study
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 17 / 2024
- Published online by Cambridge University Press:
- 26 December 2024, e43
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Telehealth-delivered recovery-orientated well-being plan group program for bipolar disorder: a pilot randomised feasibility and acceptability study
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 52 / Issue 6 / November 2024
- Published online by Cambridge University Press:
- 11 September 2024, pp. 681-686
- Print publication:
- November 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A CBT-based training module for UK health visitors who support parents with excessively crying babies: development and initial evaluation
-
- Journal:
- Primary Health Care Research & Development / Volume 25 / 2024
- Published online by Cambridge University Press:
- 19 April 2024, e20
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Brief scales for the measurement of target variables and processes of change in cognitive behaviour therapy for major depression, panic disorder and social anxiety disorder
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 52 / Issue 4 / July 2024
- Published online by Cambridge University Press:
- 21 November 2023, pp. 376-393
- Print publication:
- July 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
‘I almost felt like I can be a little bit more honest’: experiences of a telehealth group for bipolar disorder
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 16 / 2023
- Published online by Cambridge University Press:
- 04 October 2023, e26
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
What if we have too many models of worry and GAD? – ADDENDUM
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 6 / November 2023
- Published online by Cambridge University Press:
- 16 June 2023, p. 659
- Print publication:
- November 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Overcoming death anxiety: a phase I trial of an online CBT program in a clinical sample
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 4 / July 2023
- Published online by Cambridge University Press:
- 24 March 2023, pp. 374-379
- Print publication:
- July 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The wellbeing neuro course: a randomised controlled trial of an internet-delivered transdiagnostic psychological intervention for adults with neurological disorders
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 14 / October 2023
- Published online by Cambridge University Press:
- 01 March 2023, pp. 6817-6827
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Cognitive behaviour therapy (CBT) as a psychological intervention in the treatment of ARFID for children and young people
- Part of
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 16 / 2023
- Published online by Cambridge University Press:
- 22 February 2023, e5
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Internet-delivered cognitive behavioural therapy for chronic fatigue among adolescents with a chronic medical condition: a single case study
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 3 / May 2023
- Published online by Cambridge University Press:
- 15 February 2023, pp. 259-264
- Print publication:
- May 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Three ways to change your mind: an epistemic framework for cognitive interventions
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 3 / May 2023
- Published online by Cambridge University Press:
- 06 February 2023, pp. 187-199
- Print publication:
- May 2023
-
- Article
- Export citation
Cost-effectiveness of transdiagnostic group cognitive behavioural therapy for anxiety disorders v. treatment as usual: economic evaluation of a pragmatic randomized controlled trial over an 8-month time horizon using self-reported data
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 14 / October 2023
- Published online by Cambridge University Press:
- 25 January 2023, pp. 6570-6582
-
- Article
- Export citation
Development of competence in cognitive behavioural therapy and the role of metacognition among clinical psychology and psychotherapy students
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 51 / Issue 3 / May 2023
- Published online by Cambridge University Press:
- 24 January 2023, pp. 200-213
- Print publication:
- May 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Assessing the usability and acceptability of Face IT@home: an online CBT intervention for people with visible differences
-
- Journal:
- The Cognitive Behaviour Therapist / Volume 15 / 2022
- Published online by Cambridge University Press:
- 14 September 2022, e41
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
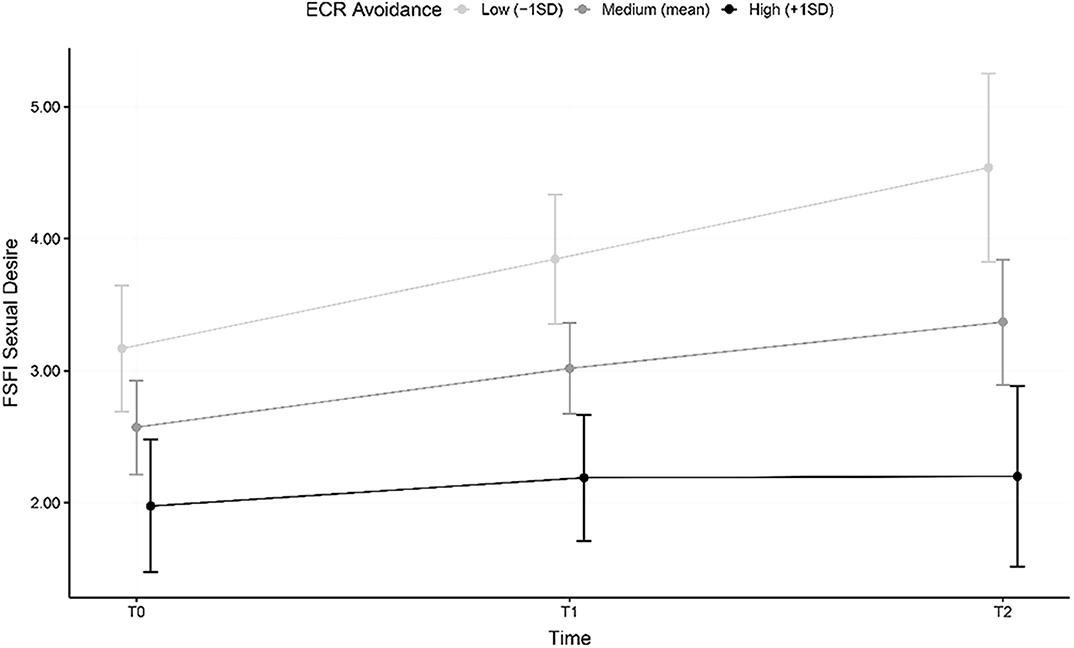
Recovery of healthy sexuality in patients with Anorexia Nervosa treated with Enhanced Cognitive Behaviour Therapy (CBT-E): results from a two-year follow-up study highlighting the role of avoidant attachment style
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S71-S72
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
There is a known association between the core psychopathological features of anorexia nervosa (AN) and sexual dysfunctions, to the point that the recovery of healthy sexuality could be considered a marker of recovery. However, no studies have evaluated the role of insecure attachment in moderating this recovery during treatment.
ObjectivesTo evaluate the role of insecure attachment as a possible moderator of the recovery of healthy sexuality in patients with AN treated with Enhanced Cognitive Behaviour Therapy (CBT-E).
MethodsA total of 65 patients with anorexia nervosa were treated with CBT-E in a multidisciplinary environment, after filling out self-administered questionnaires for the evaluation of general (SCL-90-R) and ED-specific psychopathology (EDE-Q), female sexuality (FSFI) and adult attachment style (ECR). The assessment was repeated after one (T1) and two years (T2).
ResultsAt baseline, all domains of sexual dysfunction were significantly predicted by avoidant attachment. A significant amelioration of both general and eating disorder-specific psychopathology and sexual dysfunctions was observed at all follow-up evaluations with respect to baseline levels. However, only 45% of remitted patients also showed a complete recovery of healthy sexuality: this subgroup reported significantly lower avoidance scores when compared to patients who only recovered from AN. Moderation analysis indicated that sexual desire did not increase in participants with higher levels of avoidant attachment.
 Conclusions
ConclusionsThis study highlighted the crucial role of avoidant attachment in the relationship between AN and sexual dysfunctions, underlining the importance of assessing adult attachment for a better characterization and treatment. Attachment-focused interventions may be beneficial for a full recovery.
DisclosureNo significant relationships.

Group intervention for sexual minority adults with common mental health problems: preliminary evaluation
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 50 / Issue 6 / November 2022
- Published online by Cambridge University Press:
- 11 August 2022, pp. 575-589
- Print publication:
- November 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Internet-delivered cognitive behaviour therapy for post-traumatic stress disorder: a randomised controlled trial and outcomes in routine care
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 50 / Issue 6 / November 2022
- Published online by Cambridge University Press:
- 04 August 2022, pp. 649-655
- Print publication:
- November 2022
-
- Article
- Export citation
More than doubling the clinical benefit of each hour of therapist time: a randomised controlled trial of internet cognitive therapy for social anxiety disorder
-
- Journal:
- Psychological Medicine / Volume 53 / Issue 11 / August 2023
- Published online by Cambridge University Press:
- 15 July 2022, pp. 5022-5032
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
