
102 results
Impaired health-related quality of life, and depressive symptoms in a cohort of healthy adults with symptoms of attention deficit/hyperactivity disorder
-
- Journal:
- European Psychiatry / Volume 68 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 03 March 2025, e44
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Prevalence and comorbidity rates of disruptive mood dysregulation disorder in epidemiological and clinical samples: systematic review and meta-analysis
- Part of
-
- Journal:
- European Psychiatry / Volume 68 / Issue 1 / 2025
- Published online by Cambridge University Press:
- 15 January 2025, e11
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Surge in antidepressant usage among adolescents and young adults during the COVID-19 pandemic: insights from an interrupted time series analysis
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 33 / 2024
- Published online by Cambridge University Press:
- 07 November 2024, e62
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Gender differences in the relationship between depressive symptoms and diabetes associated with cognitive-affective symptoms
-
- Journal:
- BJPsych Open / Volume 10 / Issue 6 / November 2024
- Published online by Cambridge University Press:
- 05 November 2024, e192
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Electroconvulsive therapy response and remission in moderate to severe depressive illness: a decade of national Scottish data
-
- Journal:
- The British Journal of Psychiatry / Volume 225 / Issue 6 / December 2024
- Published online by Cambridge University Press:
- 18 September 2024, pp. 547-555
- Print publication:
- December 2024
-
- Article
-
- You have access
- HTML
- Export citation
Chapter 16 - Inflammation and Metabolic Issues in Mood Disorders
-
-
- Book:
- Clinical Textbook of Mood Disorders
- Published online:
- 16 May 2024
- Print publication:
- 23 May 2024, pp 163-171
-
- Chapter
- Export citation
Association of clinical variables and thyroid-stimulating hormone with psychotic symptoms in patients with first-episode and drug-naïve major depressive disorder with elevated fasting blood glucose: preliminary exploratory study with a large sample
-
- Journal:
- BJPsych Open / Volume 10 / Issue 3 / May 2024
- Published online by Cambridge University Press:
- 03 May 2024, e99
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
A retrospective analysis of iv ketamine outcome on hospitalisations in an unselected psychiatric sample
-
- Journal:
- Acta Neuropsychiatrica / Volume 37 / 2025
- Published online by Cambridge University Press:
- 25 April 2024, e13
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Associations between body weight change and incidence of major depressive disorder in patients with type 2 diabetes mellitus: a nationwide longitudinal follow-up cohort study of 1.1 million
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 10 / July 2024
- Published online by Cambridge University Press:
- 12 March 2024, pp. 2380-2388
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Dysfunction of circulating endothelial progenitor cells in major depressive disorder
-
- Journal:
- Acta Neuropsychiatrica / Volume 36 / Issue 3 / June 2024
- Published online by Cambridge University Press:
- 05 January 2024, pp. 153-161
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Mental illness and cardiovascular health: observational and polygenic score analyses in a population-based cohort study
-
- Journal:
- Psychological Medicine / Volume 54 / Issue 5 / April 2024
- Published online by Cambridge University Press:
- 14 September 2023, pp. 931-939
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
ICD-11 and bipolar II disorder: so much ado and yet nothing new
-
- Journal:
- The British Journal of Psychiatry / Volume 223 / Issue 2 / August 2023
- Published online by Cambridge University Press:
- 01 August 2023, pp. 345-347
- Print publication:
- August 2023
-
- Article
-
- You have access
- HTML
- Export citation
School-based socio-emotional learning programs to prevent depression, anxiety and suicide among adolescents: a global cost-effectiveness analysis
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 32 / 2023
- Published online by Cambridge University Press:
- 12 July 2023, e46
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Lurasidone and risk of metabolic syndrome: results from short and long-term studies in patients with bipolar depression
-
- Journal:
- CNS Spectrums / Volume 28 / Issue 6 / December 2023
- Published online by Cambridge University Press:
- 24 March 2023, pp. 680-687
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The male–female suicide ratio in Denmark plateaus at 2.7: an opportunity for targeted intervention?
-
- Journal:
- Acta Neuropsychiatrica / Volume 35 / Issue 1 / February 2023
- Published online by Cambridge University Press:
- 05 January 2023, pp. 61-62
-
- Article
- Export citation
The role of pre-pandemic depression for changes in depression, anxiety, and loneliness during the COVID-19 pandemic: Results from a longitudinal probability sample of adults from Germany
-
- Journal:
- European Psychiatry / Volume 65 / Issue 1 / 2022
- Published online by Cambridge University Press:
- 03 November 2022, e76
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Resistance or pseudo-resistance?
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S370-S371
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Treatment-Resistant Depression continues to represent a great challenge for clinicians.
ObjectivesWe investigated patients with history of resistance, assessing prognostic factors, response to treatments, and remission over time.
MethodsWe recruited 202 unipolar and bipolar depressed inpatients. According to anamnestic backgrounds, patients were assigned to: A) Non-resistant: responders, with no characteristics of resistance in the current episode. B) Resistant: resistant to two antidepressant trials of adequate doses and duration. C) Pseudo-resistant: non-responders, not classifiable as Resistant because of inadequate trials. During hospitalization, patients were treated by clinical judgment, following a rehabilitation program.
Results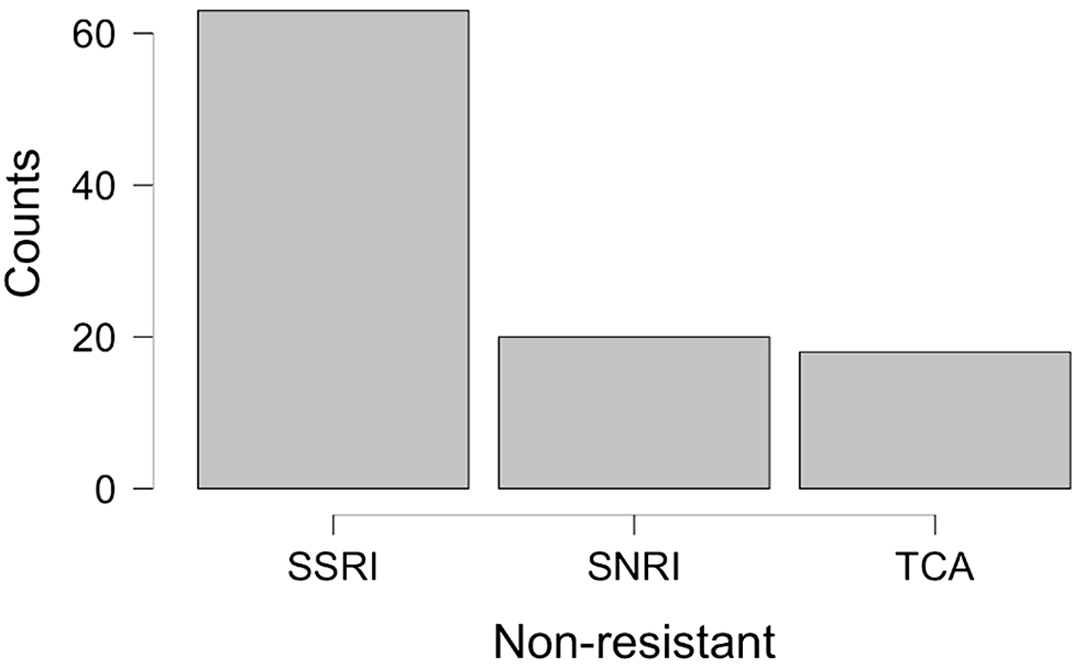
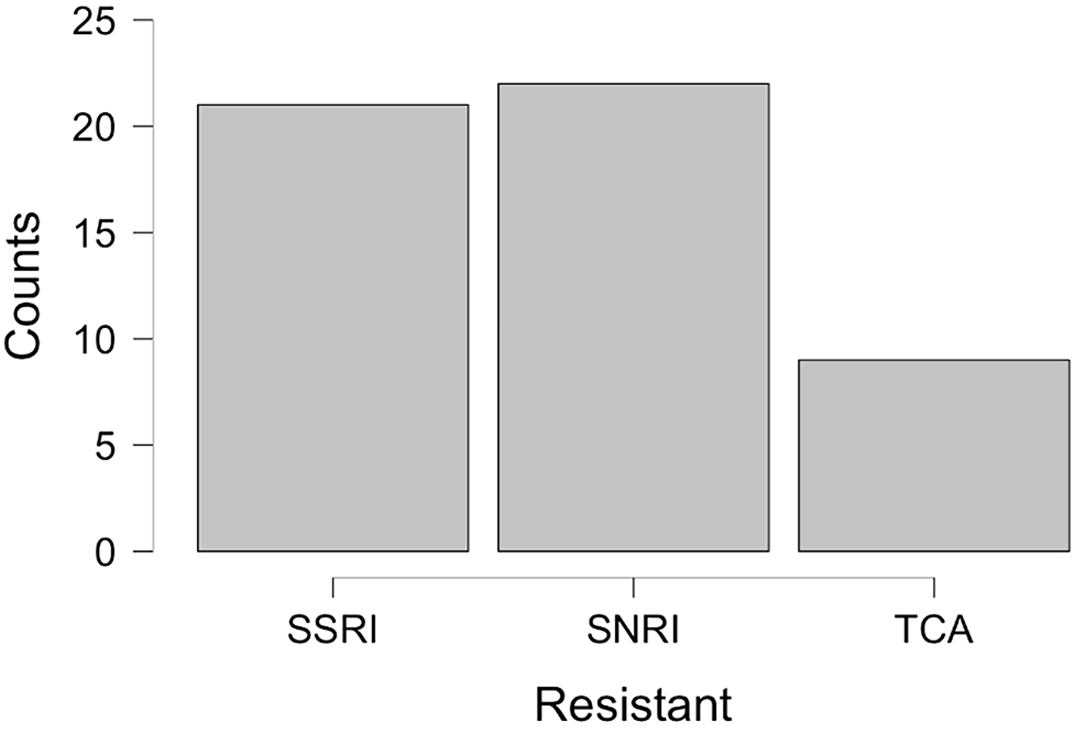
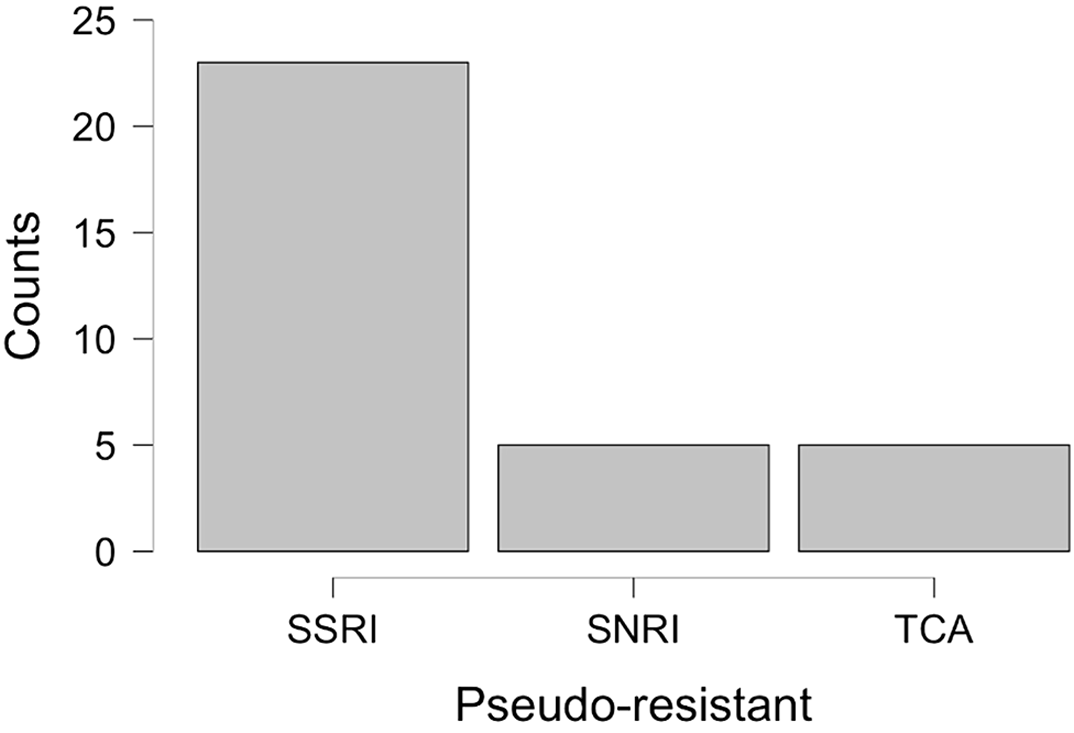
Table 1 Non-resistant (111) Resistant (54) Pseudo-resistant (35) p-value Age 59.1±11.9 63.0±12.6 57.0±11.3 0.036* Episodes of illness 3.8±2.1 4.0±1.9 3.0±1.8 0.036* Personality disorders 27.0% 18.9% 48.6% 0.009** Therapies: 0.014** SSRI 62.4% 40.4% 69.7% SNRI 19.8% 42.3% 15.1% TCA 17.8% 17.3% 15.1% Augmentation 24.3% 38.9% 17.1% 0.05** Remission 76.5% 59.5% 81.2% CvsB:0.045** CvsA:0.587** On the day of admission, non-responders were 44.5% of the sample, but 39.3% of them did not meet the Resistant criteria, defining the Pseudo-resistant group. Pseudo-resistant differed from others by younger age, fewer illness episodes, higher rate of personality disorders, and different therapies during hospitalization [Fig.1,2,3]. Pseudo-resistant remission rate, significantly greater than Resistant one, was comparable to Non-resistant [Tab.1]. *Kruskal-Wallis Test **Chi-Squared Test
ConclusionsThis study outlines a new group of depressed patients that, apparently drug-resistant, displays the same outcome as responders when treated with first-line drugs during hospitalization, certainly taking benefit from the psychoeducational program. Quick recognition of these patients could be crucial to giving optimal care.
DisclosureNo significant relationships.



Association between Mood Disorders, Problematic Internet Use and Online Gambling Addiction: A Systematic Review
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S834
-
- Article
-
- You have access
- Open access
- Export citation
comparisation of ABO blood groups between female patiens diagnosed with depressive disorders an bipolar affective disorders
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S851
-
- Article
-
- You have access
- Open access
- Export citation
Attitudes towards death in adolescents hospitalized with depressive disorder
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S560
-
- Article
-
- You have access
- Open access
- Export citation

